Influenza B infections in children:A review
2020-11-17YellanthoorRameshBhat
Yellanthoor Ramesh Bhat
Abstract
Key Words:Children;Influenza B;Hospitalization;Oseltamivir;Respiratory infections;Severity
INTRODUCTION
Influenza is a major public health problem worldwide[1-3].It is one of the most common respiratory infectious diseases.The influenza viruses belong to the Orthomyxoviridae family and contain a single-stranded RNA genome.There are three types of influenza viruses A, B, and C based on different structural arrangements of internal nucleoprotein and matrix protein antigens.Influenza A (IFA) causes more severe illness and hence is well studied.Influenza B (IFB) is less studied in children although its impact is substantial.IFB has two antigenically and genetically distinct lineages,B/Victoria/2/87-like (Victoria lineage) and B/Yamagata/16/88-like (Yamagata lineage).Influenza C (IFC) is known to cause upper respiratory tract infection in younger children.It also causes community-acquired pneumonia.The severity of infection is less than that of IFA but more than that of IFB.C/Kanagawa/1/76-related lineages and C/Sao Paulo/378/82-related lineages are the IFC strains identified in the influenza seasons 2008-2009 and 2009-2010 in Milan[4].IFB viruses have circulated worldwide since 1983 causing outbreaks now and then[5-8].IFB usually causes mild to moderate illness in healthy individuals including children.However, severe disease in children, the elderly, and individuals with chronic medical conditions have been reported.Serious illness leading to mortality, although rare, has been described.Worldwide, young children exposed to IFB had a higher disease severity compared with adults[9-13].Antiviral agents decrease the severity of illness and hospitalization[8].Due to the enormous health and economic impact of IFB, these strains are included in vaccines.In this review, the disease burden, clinical manifestations, differences between IFA and IFB illness, treatment, prognosis, and prevention of IFB illness in children are discussed.
EPIDEMIOLOGY AND DISEASE BURDEN
IFB was first identified in 1940.The second lineage was discovered in 1983.Since then frequent outbreaks of IFB have occurred worldwide[1,3,5,6].From 2001 onwards, both IFB lineages have been co-circulating each influenza season.Children are more susceptible to infection.In particular, children under 5 years of age are more susceptible to influenza illness as they are an immunologically naïve population.IFB caused significant morbidity in children in the United States during 2004-2011, and in the United Kingdom during 2010-2011 seasons[1-3,5,6].The influenza-associated disease burden among infants and young children is likely to be underestimated because of the similarity of illness caused by other respiratory viruses during an influenza season.Annual IFA and IFB attack rates among children aged 5 to 9 years reach 35%,compared with those rates among the adult population which approach 13% for IFA and 6% for IFB.IFB outbreaks occurred worldwide from November 2017 to April 2018.The illness caused significant health and economic impacts worldwide[1-3,5-7].
Mancinelliet al[2]reported that among the IFB isolates, 91.54% were the B/Yamagata/16/88 lineage and 8.45% were the B/Victoria/2/87 lineage during the 2012-2013 influenza season in Italy.The B/Yamagata/16/88 lineage was most prevalent in children 3-6 years old.They reported the median length of hospital stay of 3 d for IFB viral illness.An Indian study reported high influenza-associated mortality in children aged less than 5 years in addition to the elderly population[10].Studies on the incidence, clinical burden, and economic impact of IFB helped to include an additional B strain in the vaccine against influenza.A study involving IFB cases across 9 European countries reported wide variations in IFB cases during 1998-2013[5].
The Global Influenza B Study that included 1820301 influenza cases from 31 countries during 2000-2018 reported 419167 (23.0%) cases of IFB[14].Cases from the United States (54.1%) and Australia (25.3%) contributed the maximum number of cases.In countries of the Southern hemisphere, IFA epidemics peak in July-September,and IFB peaks in August-September.In countries of Northern hemisphere, IFA peaks in January-February and IFB peaks in February-March (Table 1).However, there were exceptions to this pattern in some countries.In most countries, IFB/Victoria showed a unimodal curve with a peak below 10 years of age.B/Yamagata cases frequently showed two peaks, one peak below 10 years of age, and another peak between 25 and 50 years of age.In tropical countries, the timing of IFA and IFB epidemics differ.There appears to be no consistent pattern in the timing of the different epidemics.B/Victoria occurs more frequently in tropical countries, while B/Yamagata occurs frequently in temperate climate countries of the Southern and Northern hemispheres.
IFB-VIRAL CHARACTERISTICS
IFB viruses belong to the Orthomyxoviridae family[1,5,14].They are single-stranded RNA viruses.They are classified into two lineages:B/Yamagata and B/Victoria.IFB viruses are further classified into specific clades and sub-clades.The B/Victoria clades include V1A and subclades include V1A.1, V1A.2, and V1A.3.B/Yamagata clades include Y1,Y2, and Y3.There are no subclades in B/Yamagata.
The virion of IFB virus consists of an envelope, a matrix protein, a nucleoprotein complex, a nucleocapsid, and a polymerase complex.The IFB virus has eight genome segments.The proteins of the polymerase complexes include PB1, PB2, and PA.The polymerase complexes are located at the ends of the nucleocapsids.These capsids are helical in nature.The nucleocapsids are encircled by the M1 matrix protein and a lipid bilayer envelope.The viral surface has two glycoproteins;hemagglutinin (HA) and neuraminidase (NA).The HA, NA and the M2 matrix protein are embedded in the lipid bilayer envelope.The IFB virus has 500 or more surface projections.These surface projections are made of HA and NA.
The IFB virus undergoes antigenic variation through genetic reassortment among co-circulating strains and antigenic drift from cumulative mutations[5,14].IFB viruses generally change their genetic and antigenic properties more slowly than IFA viruses.IFB virus HAs have a mutational rate about five times slower than that observed for IFA virus HAs.The IFB virus is relatively vulnerable to certain environmental impacts.The virus can survive for several hours in the environment depending on humidity and temperature.In water, at <20°C, the virus can survive for several months.Influenza viruses are sensitive to lipid solvents and detergents.
CLINICAL FEATURES
IFB illness in children ranges from subclinical illness to complicated disease involving multiple organs.The typical manifestations include respiratory tract and systemic signs and symptoms.IFB can present as croup, bronchiolitis, pneumonia and febrile disease mimicking bacterial sepsis.Central nervous system, cardiac, muscle, or renal complications can also occur[1-3,5-7,11-17].IFB illness in children may predispose to bacterial superinfections.IFB viruses tend to persist across multiple seasons and exhibit complex global dynamics[18].A peak between August and September has been observed in countries of the Southern hemisphere.In countries of the Northern Hemisphere, the peak occurs in February-March.There are exceptions to this pattern in certain countries.Generally IFB epidemics tend to peak three weeks after the IFA epidemics during winter in temperate countries of Southern and Northern hemispheres[14,18].An Indian study involving children found more cases from January to May with a peak in March[12].In younger children distinguishing influenza from other febrile illnesses based on clinical manifestations alone is often difficult.
IFB most often causes respiratory infections with cough, fever, myalgia, chills and malaise.The illness may last for two to eight days.The onset is typically rapid.A minority of patients, especially young children, and those with medical comorbidities may have severe disease.Respiratory and multi-organ failure may occur either due to virus or secondary bacterial pneumonia.IFB also affects children with underlying malignancies such as lymphoma, leukemia, solid tumor, or renal tubular disorders.
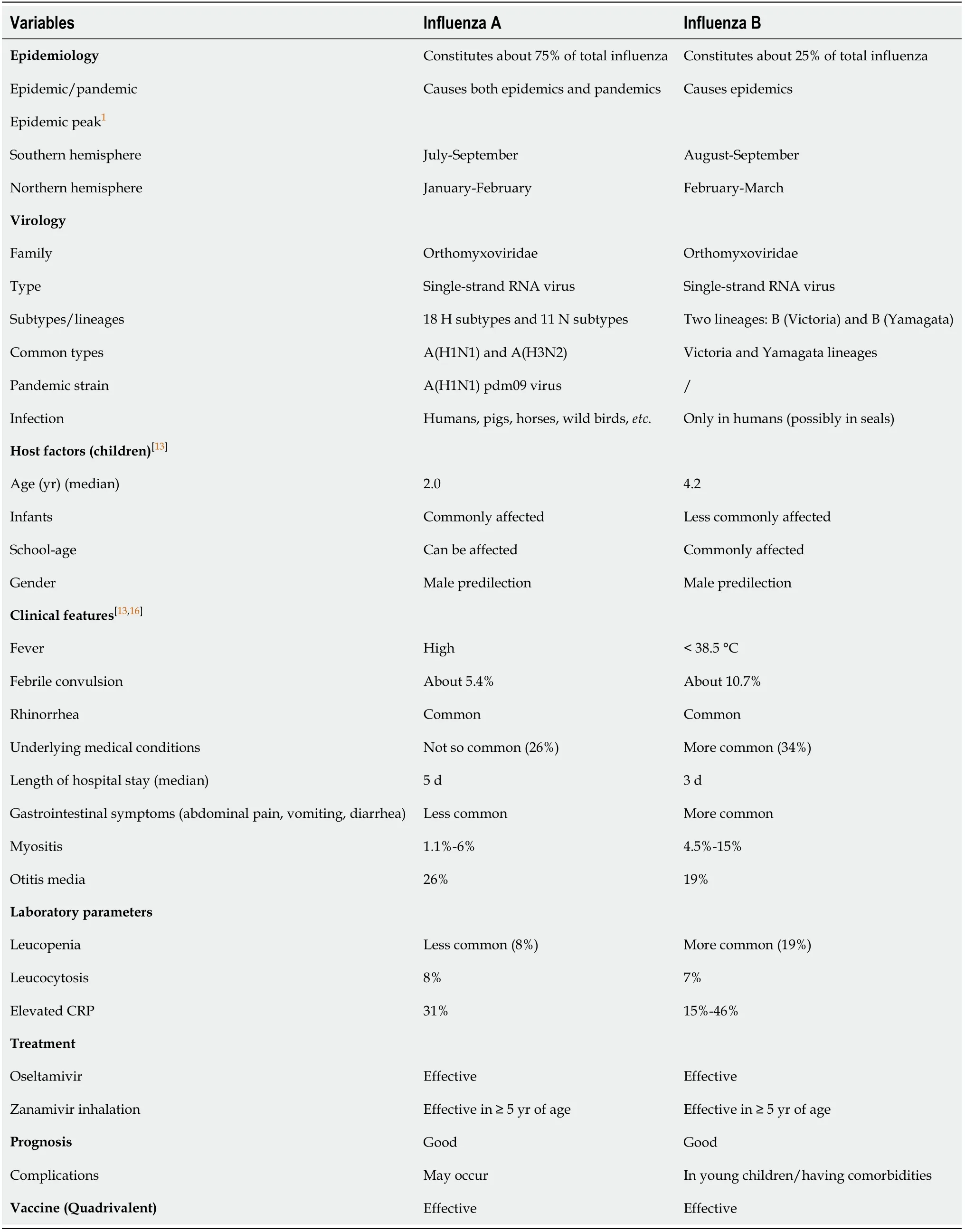
Table 1 The differences between influenza A and influenza B illness in children[2,13-16]
The highest frequency of IFB infections is said to occur in infants less than one year of age.The median age of children with IFB viral illness is 4.2 years[13].High fever especially an abrupt onset is common.Febrile convulsions are reported in 9% of children.Rhinorrhea and cough are the usual manifestations.Vomiting or diarrhea may occur in 25% of cases.Myalgia or myositis may be present in 15% and headache occurs in 25%.Pneumonia, otitis, and encephalitis may occur in a small percentage of children.
An Indian study involving IFB in children found upper respiratory tract infections in 78.5% cases followed by pneumonia in 19.6% and severe pneumonia in 1.7%[12].The peak of the illness was observed in March.Male children predominated in the study.Male predominance in IFB illness has also been reported in other studies[14-19].
Gastrointestinal symptoms such as abdominal pain, diarrhea, and vomiting in IFB children were reported by Lennonet al[16].Encephalitis is a rare manifestation of IFB.A 6-year-old girl with acute IFB virus encephalitis resulting in neurological sequelae was reported by McCullerset al[20].IFB associated encephalitis, profound weakness, and response to oseltamivir in a 10-year-old boy was reported by Straumaniset al[21].
Chiet al[19]studied 118 cases of IFB in Taiwan with characteristics of Yamagata and Victoria strains.They reported a higher incidence of lower respiratory tract infections with Yamagata-like strains.All invasive diseases particularly occurred with this strain.Children infected with the Victoria-like group had the longest hospital stays.
HOST FACTORS
Influenza is a major cause of morbidity and mortality in humans globally.Certain age groups are more susceptible to influenza.Children and the elderly are more vulnerable to influenza.IFB commonly affects younger children.Eşkiet al[22]reported that children less than 5 years of age had a higher hospitalization rate (82.9%).The strongest association between hospitalization and age was observed for children ≤ 2 years of age (63.6%) compared with other age categories (36.4%).
IFB related childhood morbidity and mortality increases with certain comorbidities.Underlying medical comorbidities such as asthma, neurologic deficits, or malignancies were documented in one-fourth of the children with IFA or IFB[13].Congenital heart disease, neuromuscular disease, immunosuppression, presence of neutrophilia,lymphopenia, severe bacterial infections, and late initiation of antiviral therapy were found to be independent risk factors for prolonged hospitalization in patients with IFB-related lower respiratory infections.Prolonged hospitalization was more common in children with comorbidities (24.3%) compared to children without comorbidities(10.4%).
HOW IS IFB DIFFERENT FROM IFA?
Among influenza viruses, IFA virus causes more severe disease.Certain differences in median age, clinical manifestations, illness severity, risk factors, and length of hospitalization were observed between IFA and IFB illness in various studies[2,6,11,15].Peltolaet al[13]reported that the median age of children with IFA was 2.0 years and was 4.2 years in children with IFB.Infants accounted for 27% of children with IFA and 24%of those with IFB.Boys predominated in both IFA and IFB infected children.Underlying medical conditions were present in 26% of the children with IFA and in 34% of those with IFB.Fever is a common symptom in both IFA and IFB affected children.High fever and rhinorrhea were more common in IFA than in IFB.Respiratory symptoms were more prevalent in patients affected by IFA than by IFB.
Mancinelliet al[2]reported more IFA cases in children less than one-year-old and more IFB cases among school-age children.The length of stay in children with IFA was significantly longer than those infected with IFB.The median length of stay was 5 d(range:0-59) for IFA and 3 d (range:0-116) for IFB.IFB children mostly had a fever <38°C.An Indian study also observed more IFB cases in the older age group[12].Respiratory symptoms dominate in IFA children.Lennonet al[16]found that gastrointestinal symptoms such as abdominal pain, diarrhea, and vomiting were more common in IFB than IFA infection.Children with IFB were more likely than those with IFA to be diagnosed with upper respiratory tract infection, myositis, and gastroenteritis.Children with underlying malignancies such as lymphoma, leukemia,and solid tumor were more susceptible to IFB infection.
LABORATORY TESTS
Several different approaches are currently available for the diagnosis of influenza infections in children[23-25].These include nucleic acid amplification tests (NAT),immunochromatography-based rapid diagnostic tests, immunofluorescence assays and viral isolation in cell culture[23].Rapid molecular assays are the preferred diagnostic tests.The advantages of these tests include accuracy, faster results and ease of the test at the point of care[24].
Rapid molecular assays are more sensitive compared to antigen-based tests.They can detect viruses much earlier in clinical samples.The tests for the diagnosis of influenza infections include reverse transcriptase polymerase chain reaction (RT-PCR),next-generation sequencing, ligase chain reaction, sequencing-based tests including pyrosequencing, DNA microarray-based tests, nucleic acid sequencing-based amplification, loop-mediated isothermal amplification-based assay, simple amplification-based assay,etc.[23].Most of these tests take 2 to 4 h to complete.They demonstrate higher sensitivity and specificity compared with antigen-based tests.RTPCR, a gold standard assay for influenza diagnosis involves three essential steps:extraction of viral RNA from clinical specimens;reverse transcription of viral RNA to a single-stranded cDNA using the enzyme reverse transcriptase, and amplification of the PCR product is coupled to fluorescent detection of labeled PCR products[23,24].RTPCR is the most powerful NAT used to identify influenza viruses across many laboratories in the world.
Nasopharyngeal and nasal swab samples should be obtained from influenza affected children and transported to the laboratory in a universal viral transport medium.Samples of throat and nasal swabs, nasopharyngeal aspirate,bronchoalveolar lavage, and sputum may also be taken depending upon the clinical situations.The samples should either be processed immediately or stored at -80°C before testing.Nucleic acid extraction and reverse transcription should be performed initially.Samples positive for IFB are further characterized by genotyping analysis to identify the subtype;the B/Yamagata/16/88 and B/Victoria/2/87 lineages.Different primers are used to identify the Victoria lineage and Yamagata lineage[23-25].
Other laboratory tests include white blood cell (WBC) counts and serum C-reactive protein (CRP) levels.The WBC counts and CRP levels may be helpful in detecting bacterial co-infections.Both WBC counts and CRP levels are low in uncomplicated IFB illness.A decreased WBC count of less than 4000/mm3or more than 15000/mm3can occur in approximately 10% of children with IFB[13].Leukopenia and lymphopenia are common in IFB illness.Hence, these isolated findings need not be considered for further evaluation.IFB is more likely associated with leukopenia than IFA.One study reported an elevated CRP level in 46% of IFB children[2].
TREATMENT
The children affected by IFB need supportive care and antiviral agents[26-30].The neuraminidase inhibitors are effective for IFB illness in children.Oral oseltamivir is effective in children aged 1-12 years.This drug efficiently metabolizes to the active carboxy metabolite.The oseltamivir carboxylate is primarily eliminated by renal excretion.A pharmacokinetic model in children indicated that a dose of oseltamivir 2 mg/(kg·dose) twice a day would be safe and effective[29].
Early administration of oseltamivir can reduce the risk of IFB virus-associated pneumonia[8].In-field trials supported the benefit of anti-influenza drugs especially when they are administered within 48 h after the onset of symptoms[13,28,29].Whitleyet al[29]in their randomized controlled study enrolled 144 IFB infected children.In the subgroup analyses they showed a significant reduction in the median duration of fever, cough, coryza and other symptoms in the oseltamivir group (Placebo, 100 h;Oseltamivir, 73 h;P=0.01).Other benefits of oseltamivir include a rapid decline in viral shedding and a significant reduction in complications, particularly otitis media.Oseltamivir is well tolerated in children.Vomiting may be observed in a few children.Oseltamivir treatment might also reduce the likelihood of the spread of influenza to close contacts.Mathesonet al[30]also found that oseltamivir was effective in reducing secondary complications.Satoet al[26]in Japan found that oseltamivir was effective in IFA and IFB, and the benefit was higher among younger children.On the other hand,Suzukiet al[27]found that oseltamivir was less effective against IFB than IFA.If clinical suspicion is strong for influenza infection, it is also advisable to start antiviral treatment without waiting for laboratory confirmation in special categories of children;those with comorbidities and unvaccinated children <6 mo of age[22].
The main advantages of neuraminidase inhibitors compared with amantadine and rimantadine, are fewer adverse effects, activity against both IFA and IFB, and rare resistance.Zanamivir is another drug effective in shortening the duration and severity of influenza.A 5-d course of twice-daily inhaled zanamivir, 10 mg, was compared with placebo in symptomatic IFB children aged 5 to 12 years[28].The zanamivir group had a reduction in the duration of IFB symptoms.
PROGNOSIS
Prognosis is generally good for children affected by IFB.Some of the affected children may require hospitalization for 2 to 8 d.The average length of hospital stay of 3 d has been documented[2].The majority (78.5%) with upper respiratory infections recovered without any complications[12].The authors reported pneumonia in 14.2% children aged>5 years, and in 5.3% children aged between one to five years.The disease tends to be severe in young children and those with comorbidities.Mortality due to IFB in children remains low.
VACCINATION
World Health Organization and Centers for Disease Control and Prevention recommend that children between 6 mo and 5 years should be vaccinated against IFA and IFB.Inclusion of this age category in vaccination helps in decreasing hospital admissions for influenza.As there is no licensed influenza vaccine for children younger than 6 mo, alternative strategies including maternal vaccination during pregnancy and household vaccination are likely to reduce the burden of influenza[22].Multiple influenza vaccine manufacturers have brought out quadrivalent seasonal influenza vaccines consisting of B strain to provide immunity against both lineages of IFB.The influenza vaccine including B strain is likely to offer benefit in children with chronic pulmonary, cardiac, or renal disease, diabetes mellitus, immunosuppression,or in those receiving long-term salicylate treatment.
CONCLUSION
IFB illness affects children worldwide during epidemics.The clinical manifestations vary depending on the lineages.The illness tends to be severe in younger children and those with comorbidities.The antiviral drug, oseltamivir is effective in children especially in reducing the duration of symptoms, viral shedding and secondary complications.The quadrivalent flu vaccine which includes IFB strain is recommended in children.
