Risk prediction rule for advanced neoplasia on screening colonoscopy for average-risk individuals
2020-10-23AlaShararaAliEIMokahalAliHarbNataliaKhalafFayezSarkisMustaphaEIHalabiNabilMansourAhmadMalliRobertHabib
Ala I Sharara, Ali EI Mokahal, Ali H Harb, Natalia Khalaf, Fayez S Sarkis, Mustapha M EI-Halabi, Nabil M Mansour, Ahmad Malli, Robert Habib
Abstract
Key Words: Colon; Adenoma; Cancer; Risk factors
INTRODUCTION
Colorectal cancer (CRC) carries a large burden of cancer-related morbidity and mortality. In 2018, CRC was the 3rdmost common malignancy and the 2nddeadliest cancer, with more than 1800000 new cases and 881000 attributable deaths worldwide[1]. The lifetime risk of CRC in patients at average risk is estimated to be 4.2% in women and 4.6% in men without screening[2]. The pathogenesis of CRC is characterized by its slow progression from a benign preneoplastic lesion to a malignant carcinoma, with an estimated natural history of over 10 years for this process to occur[3]. This allows for prevention by removing precursors prior to malignant transformation, as well as early treatment by detecting the neoplastic lesion at an early stage[4]. Advanced adenomas have a 25%-40% cumulative 10-year risk of progression to CRC depending on patient age[5]. Survival is related to stage at diagnosis[2], and thus earlier detection leads to better outcomes.
Screening through the use of fecal occult blood tests (FOBT), sigmoidoscopy and colonoscopy have been found to decrease both the incidence and mortality of CRC[6]. Screening programs have been instituted in many countries around the world. Published guidelines from multiple medical societies recommend screening all average-risk adults beginning at age 50, with the most commonly used modalities being colonoscopy and stool-based tests such an annual fecal immunohistochemistry testing (FIT) or FOBT. Less commonly employed methods of screening include flexible sigmoidoscopy, virtual colonoscopy and multi-targeted stool DNA testing. Some recommend earlier screening for patients depending on race and/or family history, but these recommendations do not employ risk stratification based on other risk factors of advanced neoplasia (AN) or CRC. Notably, resource-sensitive guidelines for screening have been recently published by the American Society of Clinical Oncology[6-9]. These guidelines recommend screening average risk individuals with colonoscopy only as an option in optimal settings[10]. In resource limited settings, screening through FIT, FOBT or a combination of sigmoidoscopy and FIT is recommended[10].
The Center for Disease Control and Prevention reports that 68.8% of age-eligible patients in the United States were screened in 2018[11]. However, screening rates around the world are not homogenous, with rates of 55% in Canada and 36% in France[12,13]. In Lebanon, CRC incidence is 12.6 and 10.7 per 100000 for men and women respectively[14], with an increasing trend possibly due to the increasing prevalence of risk factors such as obesity, tobacco use and increasing life expectancy. This is the second highest incidence rate of colorectal cancer in the Middle East and North Africa (MENA) region[14]. No formal study has evaluated the percentage of age-eligible patients who have received colorectal cancer screening, but one study reported a rate of 15% in an inpatient cohort aged 25 and older[15]. This makes improved enrollment in screening programs and the subsequent detection of adenomas and AN of crucial importance in Lebanon and similar regions where no national screening programs have been formally implemented.
Clinically usable risk assessment tools are powerful strategies by which healthcare systems and individual providers in resource-limited settings can optimize AN and early CRC detection strategies. Recently, the Lebanese Society of Gastroenterology and the Ministry of Health issued CRC screening guidelines[16]. As new programs can often result in enormous burden on the healthcare system and difficulty with implementation[17], especially in more remote regions, we set out to develop a risk prediction model for AN and CRC risk on screening colonoscopy based on easy to assess, previously validated clinical risk factors given the lack of such tools in Lebanon, the broader MENA region and similar healthcare systems. Quantifying the effect of risk factors on the detection of AN will provide a tailored tool that highlights high-risk characteristics and allow physicians and public health agencies to more efficiently target those at highest risk for both engagement in screening programs and discussion regarding risk factor modification.
MATERIALS AND METHODS
Setting
This was a prospective cohort study conducted at the American University of Beirut Medical Center (AUBMC). Over a 5-year period, 980 consecutive average-risk, asymptomatic patients scheduled for screening colonoscopy were prospectively enrolled in the study if they were aged 50 years or above and presenting for first-time screening. Patients were excluded if they had a prior history of colonoscopy, known colon polyps, inflammatory bowel disease, had undergone previous colonic resection or had family history of CRC or AN in any first-degree relative or two or more second degree relatives at any age. Diagnostic colonoscopies done for symptoms such as bleeding or abdominal pain were excluded. 92% of endoscopic examinations were performed by 4 senior attendings with > 10 years of experience. Only patients with an adequate bowel preparation (defined as excellent or good on the Aronchick scale)[18]were included. The study protocol was approved by the AUBMC Institutional Review Board and all patients provided informed consent. AUBMC is an urban, private notfor-profit, academic tertiary care center in Beirut, Lebanon.
Data collection
The study coordinator approached eligible patients prior to their procedure, obtained informed consent and then interviewed the patients using a paper-based questionnaire. This questionnaire included questions on 18 factors on the following categories: Demographics, Tobacco and alcohol use, Dietary Patterns, and concomitant medical history and medication use. We specifically inquired about the use of medications and supplements such as aspirin, nonsteroidal anti-inflammatory drugs, oral contraceptive pills/hormone replacement therapy and calcium supplements. We also inquired about the consumption of poultry, red meat, dairy and vegetables.
Information on withdrawal time, quality of bowel preparation, location, size, number and histology of polyps was collected. AN was defined as a tubular adenoma or serrated lesion ≥ 10 mm in size, any adenoma with villous features, or any lesion with high-grade dysplasia or carcinoma. In cases of multiple polyps, classification was based on the most advanced histology.
Statistical analysis
Patients’ socio-demographics, clinical and dietary habits and colonoscopy results were compared by univariate analysis for patients with and without confirmed AN. Continuous variables were summarized as mean ± SD and as median + interquartile range. Categorical factors were summarized as counts and percentages (%). Group comparisons of qualitative variables were performed usingχ2tests and Analysis of variance (ANOVA) tests as applicable, and post-hoc analyses were also conducted. For comparisons of quantitative variables, independentt-test or Mann Whitney tests were used based on the normality of data. A two-sidedPvalue less than 0.05 was used to indicate statistical significance. Statistical analyses were conducted using IBM Statistical Package for Social Sciences (SPSS), version 24 (IBM SPSS Statistics for Windows, Version 24.0. Armonk, NY: IBM Corp). A backward multivariable binary logistic regression was used to determine independent predictors of AN in the study population. For each risk factor, we derived odds ratios (OR) and corresponding 95% confidence intervals (CIs). Model results were confirmed in forward fashionviabootstrapping 1000 times and were used to derive the adjusted ORs with 95%CIs for all predictor variables.
The discriminatory ability of this model was assessed using the area under the Receiver-Operator-Characteristic (ROC) curve. Model calibration was examined using observed versus expected AN rate in logistic regression model derived probability of AN decile groups. The robustness of the model estimates was further tested using a 1000 bootstrap from which the correspondingPvalues and 95%CIs were derived and compared to those derived by the backward model. The multivariate model coefficients were used to calculate % Risk of (AN) in nomogram format as a function of patient age and separately for normal body mass index (BMI), overweight and obese patients. The model coefficients were then used to develop a risk calculator. The risk calculator provides an output percentage risk of AN as a function of patient age, BMI, smoking status and daily consumption of red meat.
RESULTS
Patient characteristics
The characteristics of the patients enrolled are listed in Table 1. The mean age of the patients was 61 ± 8 years; 501 females (51.1%) and 479 (48.9%) males were enrolled. Of those, 330 patients had a BMI < 25 kg/m2(34%), 454 (46%) had a BMI between 25 and 30 kg/m2and 196 (20%) had a BMI > 30 kg/m2. More than half the patients (53%) were smokers. Daily red meat consumption was reported by 9.2% of the enrolled patients and 10.2% consumed alcohol daily.
Colonoscopy and Pathology Findings
Of the 980 patients enrolled, 62.7% were found to have no polyp, 36.6% had tubular adenomas, 3.5% had adenoma ≥ 1 cm, 1.4% had villous histology, and 0.8% had carcinoma. The overall adenoma detection rate was 36.6% (F 29%: M 45%;P< 0.001). In total, 50 patients were found to have AN, making up 5.1% of the patients (F 3.8%; M 6.5%) enrolled in the study. The distribution of the adenomas was as follows: 29.2% of the patients had right sided adenomas, 37.7% had left sided adenomas, and 33.1% had adenomas on both sides.
Univariate analysis of risk factors for AN
The following factors were found to be significantly associated with AN risk on univariate analysis (Table 1): BMI both when categorized into obese, overweight and
normal, and when taken as a continuous variable. Daily red meat consumption, smoking as a qualitative variable and pack years smoked (both when grouped and when treated as a numeric variable), and exercise. Factors that were not associated with AN risk were age, alcohol consumption, or the presence of diabetes.

Table 1 Univariate analysis of clinical features and detection of advanced neoplasia
Development of a risk model for AN
We used backward binary logistic regression. Variables were removed from our model in case thePvalue found on logistic regression was ≥ 1. BMI values were grouped into 3 categories (< 25, 25-30 and > 30), smoking was quantified by pack years and age was taken as a continuous variable. Daily red meat consumption was categorized as yes or no. Independent predictors of AN were age [OR = 1.036 (CI = 1.00-107),P0.048], higher BMI (vsNormal BMI ≤ 25) if [Overweight: OR = 2.21 (CI = 0.98-5.00); Obese: OR = 3.54 (CI = 1.48-8.50)P0.018], tobacco pack-years [< 40: OR = 2.01 (1.01-4.01); ≥ 40: 3.96 (1.86-8.42);P0.002] and daily read meat consumption [OR = 2.02 (0.92-4.42)P0.079] (Table 2).
Internal validation of the model was doneviabootstrapping and the results are shown in Table 2. The discrimination of the model was then assessed by the Area Under the Curve (AUC) of the ROC (Figure 1). We found an AUC of 0.73 (CI = 0.66-0.79,P< 0.001). Model calibration was assessed by plotting observedvsexpected results of AN (Figure 2). A linear trend of y = 0.9204x + 0.0041 was found, with anR2of 0.8509. Using the β coefficients derived from the regression, the percent risk of AN was then calculated through a 4-factor model (age, BMI, smoking, pack years). We plotted the percent risk of AN as a function of age for the 3 separate categories of BMI, and we plotted multiple lines to show the effects of pack years smoked and the daily consumption of red meat. (Figure 3) Finally, we used the β coefficients derived by multivariate analysis to construct a risk calculator for the detection of advanced neoplasia for individuals undergoing initial screening with endoscopy. We published this risk calculator (Risk Calculator for Advanced Neoplasia for Average Risk Individuals Undergoing Screening Colonoscopy) online at http://anriskcalc.000webhostapp.com.
DISCUSSION
This cross-sectional prospective study resulted in the development of the first internally validated risk assessment tool for predicting presence of AN in an average risk cohort from the MENA region. Previous studies on Middle Eastern populations had only assessed the factors associated with development of CRC and not AN in case control studies[19-21]. Our model has good discriminatory ability through internal validation by bootstrapping. The AUCs of similar models have ranged from 0.65-0.75, showing that the discriminatory ability of the developed model is on the higher end of this range[19]. The model was also found to be well calibrated, meaning that the probabilities predicted matched the empirically derived probabilities well. We found that age, smoking and BMI were the most important risk factors for the detection of AN. These are well established risk factors that have been used in many models of colon cancer risk with biological plausibility previously explored[15,19].
We chose to exclude any patients who underwent prior CRC screening, and patients with a positive family history. As previously argued[22], prior colonoscopy is an extremely powerful surveillance tool that is able to overshadow any baseline risk stratification. A family history positive for CRC has a similar impact. Including these patient populations serves as a significant source of bias when attempting to develop risk prediction models for true average-risk individuals. In our review of the literature (Table 3), we found that of the 22 risk prediction models for average-risk individuals undergoing screening colonoscopy[24-29,33-48], only 2 excluded patients who underwent a prior colonoscopy and those with a family history of colon cancer[34,41]. One was based on a retrospective study, limiting the ability to assess the influence of life-style factors[41], while the second enrolled any patient above the age of 20[34], inconsistent with guidelines-based recommendations for CRC screening.
Although the association between age and AN was not found to be a strong one when analyzed as the variable of interest in logistic regression it remains a well-known important predictor of AN, clearly demonstrated by the nomograms in Figure 3, in which the risk of AN increases after age of 50, with steeper slope after the age of 65.
Our data also supports age as a risk factor for AN with an additive effect when combined with other risk factors such as increasing BMI and smoking. Age has been used in all 17 risk prediction models identified by a systematic review[23]. The effect ofage in our study is considerably weaker than in other models[24-26]however, in all of those models, patients were included if their age was greater than 40, while in our study patients were only included if they were older than 50, and the age spread was fairly narrow (mean 60 ± 8) limiting our ability to capture the full effect of age on AN risk. Since more than 90% of cases of CRC occur after the age of 50[27]this may have made the effect of age more pronounced in the other studies, and this may account for the discrepancy with our model. The Lebanese Ministry of Public Health has put forth screening guidelines[16]that state that screening for average risk patients should be done with FIT testing annually from age 50-75[16]however, the guidelines do not take into consideration risk factors other than age and conditions that predispose to the development of CRC, a gap our findings help fill.

Table 2 Binary logistic regression and internal validation
We found a strong increase in the risk of CRC with increased cumulative exposure to smoking. Smoking more than 40 pack-years was associated with a 4-fold increase in the odds of AN, making it the strongest risk factor in our study. This finding is particularly striking when we note that amongst our study population, 46.9% of the patients reported to be smokers[28]. The large prevalence of smoking may explain the discrepancy in the effect of smoking in our model compared to other models in which it seems to carry less influence on risk[25-27,29]. BMI was another factor found to significantly influence the risk of development of AN. Overweight individuals (BMI 25-30) have 2 times the odds of developing AN, though this did not attain statistical significance. However, obese individuals (BMI > 30) had a 3.5 times increased risk of developing AN, and this was found to be statistically significant, supporting the influence of BMI on risk in our population. This effect seems to be much larger than those found in other prediction models[24-26]. Our study population had an average BMI of 26.7, and approximately two-thirds of participants were obese or overweight. For Beteset al[25]the average BMI was 27 kg/m2, while Kamniskiet al[29]had a nearly identical distribution of BMI to our study. Indeed, the effect of BMI seems to be magnified amongst our population. A pooled analysis on the effect of obesity on the detection of adenomas showed an OR of 1.47, and our odds ratio was much larger than any of the studies in the systematic review[30]. Although reasons for this are unclear, this points to the importance of BMI as a risk factor in our population.
Red meat consumption was found to correlate with AN on univariate analysis when participants were categorized by daily consumptionvsnot, but not when participants were subcategorized by frequency of consumption. This either suggests that our study was not powered to adequately detect subtle differences in red meat intake, or possibly that red meat consumption only causes a significant effect when larger quantities are consumed. Other factors that were not found to correlate with risk of AN were alcohol use and the presence of diabetes, in contrast to findings of prior studies[31]Regarding alcohol use, 18% of patients with AN reported intake of at least one drink daily, compared to 9.8% of those with no AN, a non-significant difference.Similarly, 12% of those with AN reported diabetes, compared to 8% with no AN. Likely we were not able to find an association between these factors and AN risk due to overall low prevalence of exposure in our study population, due in part to differences in lifestyle between our population and other previously studied populations.

Table 3 Existing risk prediction studies by design, age, exclusion of family history and previous colonoscopy
The overall prevalence of AN in our cohort was 5.1%, which is comparable to rates reported in the United States[32], Europe[25,29]and Asia[26,27]. In a country like Lebanon, where resources are scarce and there is no formal national screening program for CRC, the costs of screening colonoscopy for an average-risk population may be too great to bear at the current time. In resource-limited contexts, risk stratification models could play an important role in prioritizing delivery of care. For instance, our predictive model show that the risk of advanced neoplasia in a 65 year old non-smoker male with a BMI < 25 is approximately 2%, while the risk for a 65 year old male with a BMI between 25-30 who has smoked between 10-40 pack years and consumes meat red meat daily is approximately 14%,i.e., more than 7 times the risk of the first patient. However, most published guidelines on screening with colonoscopy do not distinguish between these 2 hypothetical patients. In resource-limited settings, it may be advantageous to reserve screening colonoscopy for patients found to be at high-risk through risk stratification models, while screening low risk patients with FIT testing for cost-effectiveness. The presented model can be considered a prototype tool for underserved countries, as CRC incidence is increasing in developing countries, and has particularly been increasing in Lebanon, which currently has the second highest rate of CRC in the MENA region[11].

Figure 1 Receiver operator curve (Area under the curve = 0.73).
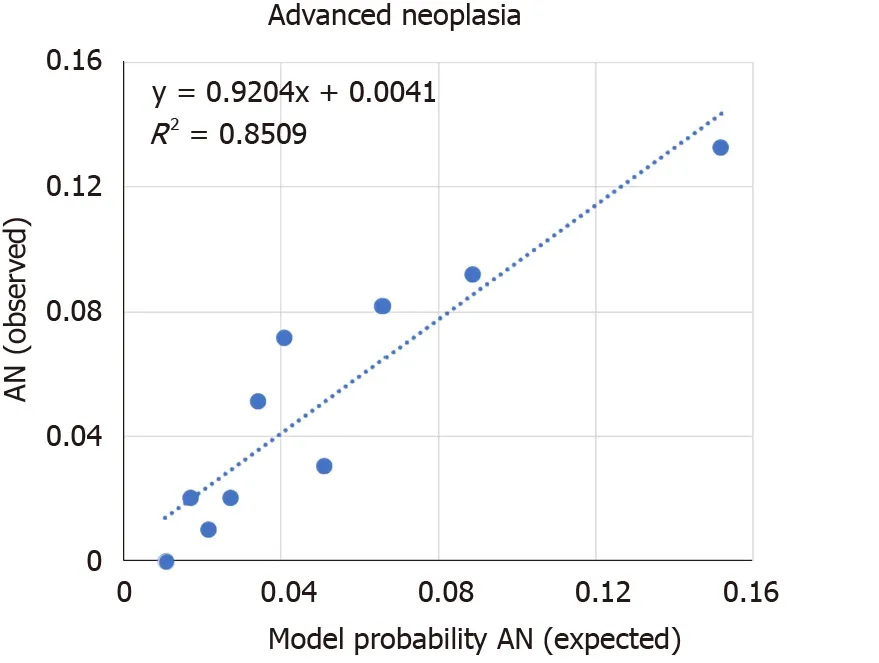
Figure 2 Model calibration plot. Each data point represents the comparison of observed (y) to expected (x) rates of advanced neoplasia in ten decile size groups (n = 98 each). The dashed line represents the linear trend with the corresponding line equation. (linear trend of y = 0.9204x + 0.0041 ; R2 = 0.8509). AN: Advanced neoplasia.
Our study has important strengths and a few limitations. The sample size is large for a country the size of Lebanon constituting 1:1000 of the at-risk population aged 50-75 in Lebanon (n= 798440)[16]. The variables used in our model are easy to ascertain clinically and often already elicited by healthcare professionals as they require only history taking, weight and height measurements in order to quantify the risk. In addition to stratification leading to more efficient CRC screening, this model can be used to educate patients on the magnitude of their risks, potentially spurring them to take an active role in modifiable risk factor modification. Our study is subject to some limitations. While internal model validation was performed, external validation in a separate population is needed to optimize model performance and increase generalizability. This study was only conducted at one large hospital, where the majority of patients have private insurance. Thus, patients from low socioeconomic status may have not been adequately represented in our sample. The patient population was also derived from patients willing to undergo screening colonoscopy, and so we may have excluded less health-conscious patients from our study. These patients may be less likely to have lifestyle-related risk factors to their health and excluding these patients may have led us to underestimate the effect of these risk factors on the presence of AN.

Figure 3 Nomograms showing the predictive model. These nomograms are a function of age and show the risk of advanced neoplasia for (BMI < 25), overweight (BMI 25-29.9) and obese (BMI > 30).
CONCLUSION
This prospective cross-sectional study identified age, obesity, smoking, and daily red meat consumption as significant predictors of advanced colorectal neoplasia in a multivariate-logarithmic analysis. Our prediction rule was internally validated by bootstrapping, and this model exhibited good calibration and discrimination. This model, available through a free online calculator, may aid in risk-stratifying patients presenting for screening for CRC in Lebanon, with the caveat that external validation is still required for this model.
ARTICLE HIGHLIGHTS


Research results
Adenoma detection and advanced neoplasia detection rates were 36.6% (F 29%: M 45%;P< 0.001) and 5.1% (F 3.8%; M 6.5%) respectively. On multivariate analysis, the predictors of AN were age [1.036 (1.00-1.07);P= 0.048], BMI [overweight 2.21 (0.98-5.00); obese 3.54 (1.48-8.50);P= 0.018], smoking [< 40 pack-years 2.01 (1.01-4.01); ≥ 40 pack-years 3.96 (1.86-8.42);P= 0.002], and daily red meat consumption [2.02 (0.92-4.42)P= 0.079]. The model had an AUC = 0.73 (CI = 0.66-0.79,P< 0.001) andR2= 0.8509.
Research conclusions
The prevalence of adenoma and AN in the average-risk Lebanese population is 5.1%, similar to those in the West. Age, smoking and BMI are important predictors of AN in our study cohort, and our model had good calibration and discrimination.
Research perspectives
In this project, we developed a risk prediction tool for advanced neoplasia at first screening colonoscopy for average risk individuals. We provide an important platform for improved risk-stratification for screening programs in resource limiting settings, although external validation of our model is needed.
ACKNOWLEDGEMENTS
The authors would like to thank the following clinicians for contributing their patients to the study: Kassem Barada, Fadi Mourad, Assaad Soweid.
杂志排行

World Journal of Gastroenterology的其它文章
- Artificial intelligence technologies for the detection of colorectal lesions: The future is now
- Transjugular intrahepatic portosystemic shunt in cirrhosis: An exhaustive critical update
- Abernethy syndrome in Slovenian children: Five case reports and review of literature
- Endoscopic retrograde cholangiopancreatography in the treatment of pancreaticopleural fistula in children
- Endoscopic ultrasound-fine needle biopsies of pancreatic lesions: Prospective study of histology quality using Franseen needle
- Helicobacter pylori infection with atrophic gastritis: An independent risk factor for colorectal adenomas