Investigation of mental health status of medical staff from Hainan who aided Hubei province to fight against COVID-19
2020-10-22XiangLaiLiuZhanLinHongZhuDaFeiZhanTianMingHanQianKunYao
Xiang-Lai Liu, Zhan Lin, Hong Zhu, Da-Fei Zhan, Tian-Ming Han, Qian-Kun Yao
Anning Hospital of Hainan Province Haikou, Hainan 570206
Keywords:COVID-19 Aid Hainan Province Medical staff Mental health Survey
ABSTRACT Objective: To analyze the mental health status of Hainan Provincial medical staff who aided Hubei Province to combat COVID-19. Methods: The Self-Rating Anxiety Scale (SAS), Self-Rating Depression Scale (SDS), Self-Reporting Questionnaire-20 (SRQ-20) and PTSD Checklist-Civilian Version(PCL-C) were used to evaluate the mental health status of 243 medical staff who aided Hubei Province to combat COVID-19. Results: A total of 221 persons have completed the psychological assessment. The survey showed that 9.05% of the medical staff had different degrees of anxiety, 16.29% had different degrees of depression, 13.12% were abnormal in Self-Reporting Questionnaire-20, and 9.05% were abnormal in PTSD Checklist-Civilian Version. There were difference in scores of Self-Rating Depression Scale across different genders, age groups, profession and educational levels, But Regression analysis rejects the correlation. Conclusions: The mental health status of Hainan Provincial medical staff who aided Hubei Province to fight against COVID-19 was abnormal, regardless of gender, age, profession or education background. Preventative measures at an early stage are warranted to alleviate the psychological problems.
1. Introduction
Since December 2019, Coronavirus Disease 2019 (COVID-19) first appeared in Hubei Province. As the virus continued to spread, new cases were found in other provinces of China. As of March 21, 2020, total confirmed COVID-19 cases in China amounted to 81,054, total deaths amounted to 3,261, according to data collected from 31 provinces and Xinjiang Construction and Production Corp. The pandemic spread internationally had been severe, as of March 21, 2020, total confirmed cases internationally exceeded 200,000[1]. In order to effectively control the spread of COVID-19, National Health Commission of China planned aid and support. Hainan province had sent 7 teams of medical professionals to aid Wuhan. Currently, the 2nd, 3rd and 5th team have returned to Hainan. During this battle with COVID-19, the medical teams were at the front line, undertaking huge pressure physically and psychologically. The purpose of this research is to understand their mental health condition so that necessary measures can be taken to alleviate the problem.
2. Objects and methods
2.1 Sample of the survey
The second, third and fifth batch of the medical aid teams (total 258 members) sent to aid Wuhan had returned home on March 17, 2020. Excluding 15 non-medical personnel, a total of 243 medical personals voluntarily participated in this survey.
2.2 Survey tools
2.2.1 General information questionnaire.
A self-designed general information questionnaire is used, which includes the patient's name, gender, age, education, profession, etc.
2.2.2 Self-Assessment Scale for Anxiety (SAS)
SAS was compiled by ZUNG et al. [2] in 1971 and was used to assess the subjective severity of anxiety. The scale has a total of 20 items, 15 positive scores, 5 negative scores, and a 4-category score. The cumulative score of each item goes the total gross score, which is then multiplied by 1.25 to get the total standard score. A total standard score <50 points means there is no anxiety, 50-59 points means mild anxiety, 60-69 points means moderate anxiety, ≥≥70 points means severe anxiety, the higher the score, the more severe the anxiety.
2.2.3 Depression Self-Assessment Scale (SDS)
SDS was compiled by ZUNG et al.[2] in 1965 and was used to assess the subjective severity of depression. The scale has a total of 20 items, 10 positive scores, 10 negative scores, and a 4-category score. The cumulative score of each item gets the total gross score, which is then multiplied by 1.25 to get the total standard score. A total standard score <53 points means the subject does not show depression, 53-64 points means mild depression, 65-74 points means moderate depression, ≥≥75 points means severe depression, the higher the score the more severe degree of depression.
2.2.4 The Mental Health
Self-Assessment Questionnaire (SRQ-20) is a simple and quick screening tool issued by the World Health Organization (WHO)[3], which has been translated into more than ten languages and used globally. The Crisis Intervention Training Manual has included it in its toolbox as a professional way for assessing the mental health of people affected by crisis. There are 20 questions in the questionnaire. "Yes" scores 1 point and "No" scores 0 point. A score above 7 points indicates emotional pain, in which case, professional help is recommended.
2.2.5 Post Traumatic Stress Disorder Checklist Civilian Version (PCL-C).
This measure is designed to evaluate the post-traumatic experience of ordinary people in their daily lives[4], consisting of 17 items, which can be classified into four factors, namely: increased alertness response, avoidance response, repeated recurrence of traumatic experience response, social function loss response. The cumulative total score of each item is 17-85 points. 17-37 points: no obvious symptoms of post-traumatic stress disorder; 38-49 points: some degree of symptoms of post-traumatic stress disorder; 50-85 points: there are more obvious symptoms of post-traumatic stress disorder, which may be diagnosed as post-traumatic stress disorder (the results are non-diagnostic and are for reference only). PCL-C is commonly used to evaluate the effects of diagnosis, intervention and treatment of post-traumatic stress disorder. It is reliable, reputable, and is one of the most widely used tools in this field.
2.3 Methods of data collection.
The tool “Questionnaire Star” is used to distribute and retrieve the questionnaires. The online questionnaires use unified instructional terms to explain the purpose of the survey and provide detailed instruction. The medical staff who returned to Hainan voluntarily filled in the survey by scanning the QR code on WeChat. The researchers then observe, collect, and cross-validate the survey data obtained from "Questionnaire Star” to ensure data accuracy and completeness.
2.4 Software SPSS22.0 is used for statistical and data analysis.
Descriptive data is described in percentages. Numerical data is tested for normality and variance homogeneity. Numerical data that follows a normal distribution is described by (mean ± standard deviation); numerical data that does not follow a normal distribution is described by median and quartiles. For data with normal distribution, T test is performed to compare the mean and homogeneity of variance; for data with non-normal distribution, Mann-Whitney test and Kruskal-Wallis test are used for mean comparison. Spearman rank correlation analysis is used to analyze the factors influencing the mental health of medical staff, and binary logistic regression was used to analyze the statistical significance of influencing factors. P<0.05 was considered statistically significant.
3. Results
3.1 General Information of Survey Objects.
In this study, a total of 243 questionnaires were issued, 221 questionnaires were collected, all of which were valid questionnaires. The effective questionnaire recovery rate was 90.9%. For specific general data survey results, see Table 1.

Table 1 General information of medical staff
3.2 The mental health status of medical staff surveyed.
Among the 221 medical staff: 9.05% show anxiety symptoms, the median anxiety level is 37.50; 16.29% show depression symptoms, the median depression level is 37.50; 13.12% self-assess their mental health as abnormal, the median mental health level is 1.00; 9.05% show symptoms of post-traumatic stress disorder, the median of post-traumatic stress disorder level is 22.00. The scores of each measure are shown in Table 2 and 3.

Table 2 Mental health status of medical staff assisting Hubei in combating COVID-19

Table 3 Statistical description of each measure
3.3 Cross section analysis of the demographic impact on different mental health measurement scoring.
We regress mental health measurement against demographic data. We observe that demographic factors such as gender, age, education level, profession all have statistical significance on explaining depression scoring. Demographic factors do not show any statistical significance in other mental health measures. See Table 4.
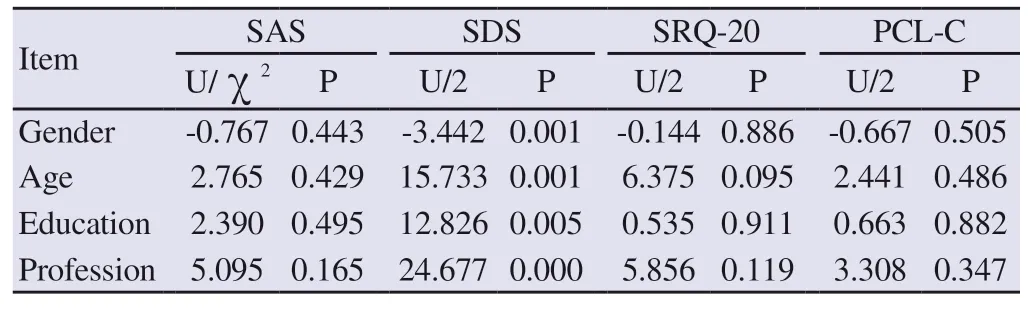
Table 4 Demographic factors and their statistical significant on mental health measurement
3.4 Spearman rank correlation analysis.
Gender, age group, education level and profession are correlated with depression self-rating score. Specifically, age group and education level are positively correlated with depression selfrating scale score (rs=0.222, rs=0.216), gender and profession are negatively correlated with depression self-rating scores (rs=-0.232, rs=-0.173). See table 5.** When the confidence (double test) is 0.01, the correlation is significant.* When the confidence (double test) is 0.05, the correlation is significant.

Table 5 Correlation between different demographic data and depression self-rating score
3.5 Binary logistic regression analysis.
For the binary logistic regression analysis: the presence of depression symptoms is chosen as dependent variable (SDS score <53 is defined as "no depression symptoms”, dependent variable = 0; SDS score ≥53 is defined as “with depression symptoms”, dependent variable = 1). Gender, age group, education level, and profession are chosen as independent variables. The results suggest that gender, age group, education level, and profession have no effect on depression symptoms. See Table 6.
4. Discussion
4.1 Mental health status of medical aid team members
The new coronavirus pneumonia infection is a sudden public health incident. Since it was first discovered, many aspects werestill unclear, coupled with its strong infectivity, it has caused great public panic. Hubei Province, as a core epidemic area, is on the cusp of the storm. It is conceivable that as a medical member who assists Hubei to fight COVID-19, he/she has taken on a lot of mental burden and pressure. The survey results show that out of 221 medical staff who assisted Hubei in combating COVID-19, 9.05% show anxiety symptoms with median anxiety level at 37.50; 16.29% show depression symptoms with median level of depression at 37.50; the mental health self-assessment scale shows that 13.12% have mental health abnormalities; 9.05% show symptoms of post-traumatic stress disorder. The result show relatively low level of mental health deterioration, compared to that in other related domestic research. For example, Mei Junhua et al. [5] used the Anxiety Self-rating Scale and Depression Self-rating Scale to survey medical staff who were confirmed or suspected to have coronavirus in several hospitals in Wuhan. The survey showed that the level of anxiety was 45.47±1.405, and the level of depression was 51.25±1.611; Xu Yuanping [6] also used the self-assessment scale for anxiety to survey the psychological status of the first batch of “Aided Hubei Anti-epidemic” military nurses. Military nurses were shown to have anxiety problems after completing their tasks, with anxiety level that were significantly higher than that in this study. Li Wei et al. [7] Meta analysis of the psychological state of different populations during the new coronavirus pneumonia epidemic found that the detection rate of anxiety symptoms was 44.5%, the detection rate of depression symptoms was 18.9%, and the detection rate of comprehensive psychological symptoms was 72.9%. Li Chuansheng et al [8] conducted a post-traumatic stress disorder survey on the front-line nurses of COVID-19 combat and found that the selfassessment scale of front-line nurses'post-traumatic stress disorder score was 40.85±15.81, and the positive detection rate of PTSD was as high as 50.73% . The above differences may be related to the type of population, the baseline level of the surveyed population, and the survey period, but it is undeniable that the mental health of the medical personnel assisting Hubei is abnormal, and early intervention is warranted.
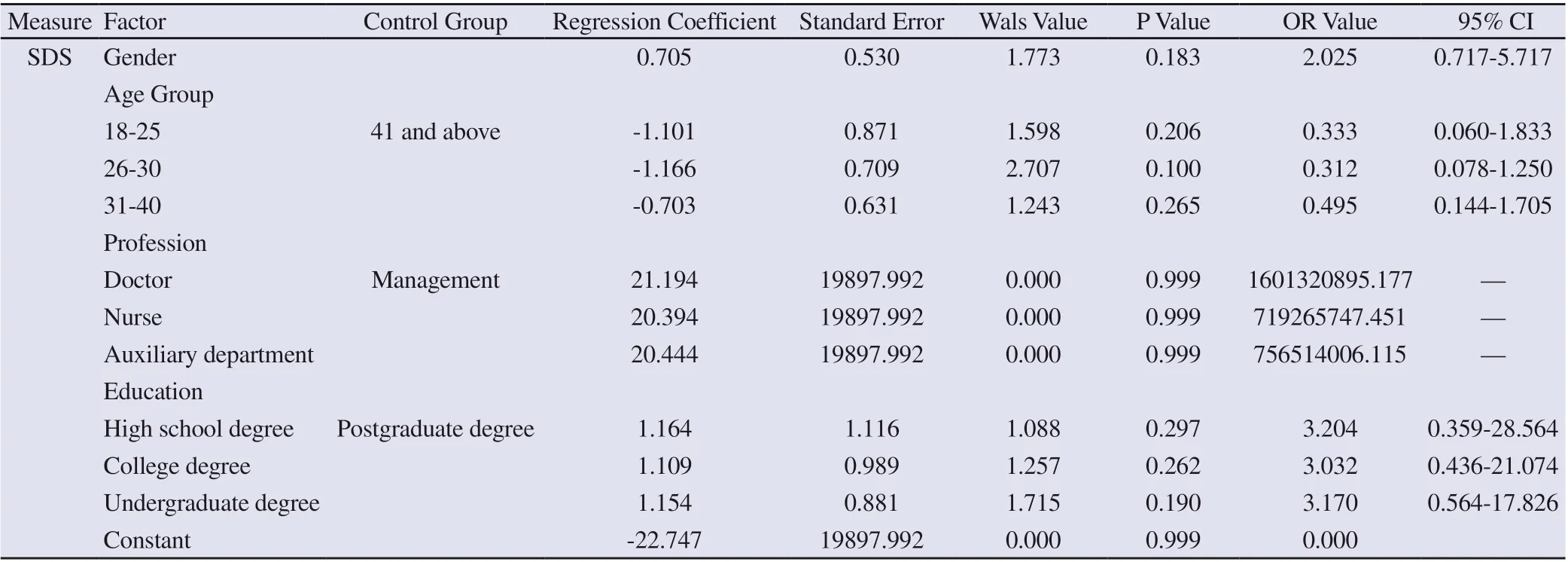
Table 6 Binary logistic regression analysis on demographic data and depression symptoms
4.2 Influencing factors of the mental health of medical personnel assisting Hubei
In this survey, only the depression self-assessment scale score was weakly correlated with gender, age group, profession, and educational level. The older the age and the higher the educational level, the higher the depression self-assessment score; however, after regression analysis this correlation significance is rejected, which is different from other domestic surveys. In the survey by Li Chuansheng et al [8], the PTSD level of nursing staff with undergraduate degree is lower than that of postgraduate degree and junior college degree, and the PTSD level of technical secondary school degree is the highest. Luo Qianyi et al [9] have surveyed the medical staff from the designated hospitals in Guangdong that receive and treat COVID-19 patients. The survey result shows that different regions, marital status and living status have influence on anxiety. There are many confounding factors that influence mental health and must be treated with caution.
5. Conclusion
The mental health status of medical staff, who returned to Hainan from aiding Hubei in the COVID-19 combat, is different from that of ordinary people. There is no significant difference in mental health measures between medical staffs with different genders, ages, profession and educational levels. The mental health status of these medical staff warrants sufficient attention and early Intervention measures. The shortcomings of this study is: this study did not do before-and-after control, it is therefore difficult to eliminate the interference of the baseline effect.
杂志排行

Journal of Hainan Medical College的其它文章
- Role of 18F-FDG SPECT / CT imaging in the diagnosis and initial staging of lymphoma
- Target prediction and mechanism of Shiyangning in treatment of perianal eczema
- Association between polymorphism of MC4R rs489693 gene and disorder of glucose and lipid metabolism in schizophrenia patients treated with olanzapine
- The value of real-time three-dimensional echocardiography in evaluating left ventricular function for different degrees of heart failure
- Meta-analysis of traditional Chinese medicine and western medicine in treating retinal vein occlusion complicated by macular edema
- Analysis of two cases of patent ductus arteriosus ligation in preterm identical twins and literature review