Physical exercise in the prevention and treatment of Alzheimer’s disease
2020-10-09ArinDeRosGloriOlsoGonzlezCorlieArChgnuFernnoMillnAnreSlvorPsulConsolionGrLuergCristinBlsoLfrgEstherGriDominguezAitorCrreteroAngelCorresJoseViMriCrmenGomezCbrer
Arin De l Ros,Glori Olso-Gonzlez,Corlie Ar-Chgnu,Fernno Milln,Anre Slvor-Psul,Consolion Gr-ı-Luerg,Cristin Blso-Lfrg,Esther Gri-Dominguez,Aitor Crretero,Angel G.Corres,Jose Vi~n,*,Mri Crmen Gomez-Cbrer,*
a Freshage Research Group,Department of Physiology,Faculty of Medicine,University of Valencia,and CIBERFES,Insitute of Health Research-INCLIVA,Valencia 46010,Spain
b INRA,UMR866 Muscle dynamics and metabolism,University of Montpellier,F-34060,Montpellier,France
c Department of Physiotherapy,Faculty of Physiotherapy,University of Valencia,Valencia 46010,Spain
d Physical Education and Sports Department,University of Valencia,Valencia 46010,Spain
Abstract Dementia is one of the greatest global challenges for health and social care in the 21st century.Alzheimer’s disease(AD),the most common type of dementia,is by no means an inevitable consequence of growing old.Several lifestyle factors may increase,or reduce,an individual’s risk of developing AD.Much has been written over the ages about the benefits of exercise and physical activity.Among the risk factors associated with AD is a low level of physical activity.The relationship between physical and mental health was established several years ago.In this review,we discuss the role of exercise (aerobic and resistance) training as a therapeutic strategy for the treatment and prevention of AD. Older adults who exercise are more likely to maintain cognition.We address the main protective mechanism on brain function modulated by physical exercise by examining both human and animal studies.We will pay especial attention to the potential role of exercise in the modulation of amyloid b turnover,inflammation,synthesis and release of neurotrophins,and improvements in cerebral blood flow.Promoting changes in lifestyle in presymptomatic and predementia disease stages may have the potential for delaying one-third of dementias worldwide. Multimodal interventions that include the adoption of an active lifestyle should be recommended for older populations.
Keywords: Aerobic exercise;Dementia;Exercise training;Lifestyle factors;Multidomain interventions;Resistance exercise
1. Introduction
Alzheimer’s disease (AD) is the most common type of dementia and one of the most frequent neurodegenerative pathologies in elderly people, constituting about 90% of the cases of dementia in this population. AD is characterized by its irreversibility and progressive functional, cognitive, and behavioral loss.It is usually accompanied by various brain disorders such as amnesia,agnosia,apraxia,and aphasia.1
Twenty-four million people in the world suffer from AD,and it is expected that by 2050 this number will be 4 times greater.2These alarming numbers are explained by the fact that the main risk factor for this disease is age,3and by 2050 it is estimated that the population over 65 years will be 3 times larger than it was in 2010, reaching close to 1.5 billion people.
AD is a devastating disease.The social and human cost for patients and caregivers is overwhelming, and the economic cost of AD is unaffordable. For instance, in the United States in 2017,the annual cost of care per patient over 65 with AD or another type of dementia was USD 48,000, or 3.5 times more than for a person without any type of dementia.4,5
AD is characterized by the loss of neuronal synapses and pyramidal neurons accompanied by progressive cognitive neurodegeneration.6The regions associated with more complex brain functions, such as the hippocampus and the neocortex,are the most affected.
Although there are several hypotheses to explain the origin of AD,the 2 main neuropathological features include the extracellular accumulation of senile plaques around the neurons and the glia,and the intracellular formation of neurofibrillary tangles(NFTs).Senile plaques are formed mainly by the accumulation of insoluble amyloid b (Ab) protein, especially its isoform Ab42, which is formed by the enzymatic cleavage of the transmembrane amyloid precursor protein (APP).7,8NFTs are formed from the hyperphosphorylation of the tau protein. The main function of this protein is to stabilize the microtubules so that they connect with other elements of the neuronal cytoskeleton,such as neurofilaments and actin.9
Another feature in AD is the inflammatory response at the brain level. In the early stages of the disease, the immune response results in a removal of Ab, ameliorating its symptoms.10,11To generate a balance between the deposition and the clearance of Ab,microglia plays a fundamental role by engulfing insoluble deposits of this peptide through the activation of receptors that promote phagocytic action,such as cluster of differentiation 36 (CD36), and receptors for advanced-glycosylation end products.12,13Microglia also activates extracellular proteases such as neprilysin, the insulin degrading enzyme, endothelin converting enzyme 1, angiotensin converting enzyme, matrix metalloprotease, and the presequence peptidase.14-16 During advanced stages of the disease there is a prolonged stimulation of the immune response caused by Ab,which leads to a decrease in the efficiency of the microglia to degrade it.17In turn, this leads to the release of several proinflammatory products,such as cytokines, reactive oxygen, and nitrogen species, leading to an increase in the production of Ab and the hyperphosphorylation of tau, generating more damage and neuronal death.18-20 This state contributes to an increase in cognitive decline and the development of the disease.
The risk factors associated with AD,apart from age,are low educational level, diabetes, genetics, belonging to certain minority ethnic groups (prevalence of dementia is higher in British African-Caribbean people),21diet, previous brain injuries, sleep disorders, hypertension, hearing loss, and low levels of physical activity.22Physical activity(“any movement of the body”) and exercise (“physical activity that is typified by specific and purposeful training”)constitute 2 different concepts.23However,for the sake of clarity we refer to both these concepts interchangeably since some of the reports we refer to in this review use these expressions as synonyms.Older adults are considered physically active when they perform moderateintensity aerobic physical activities for a minimum of 30 min,5 days/week,or vigorous-intensity aerobic activity for a minimum of 20 min,3 days/week.23Also,combinations of moderate- and vigorous-intensity activity can be performed to meet this recommendation. Moderate-intensity aerobic activity involves a moderate level of effort relative to an individual’s aerobic fitness.On a 10-point scale,where sitting is 0 and allout effort is 10,moderate-intensity activity is rated as a 5 or 6 and produces noticeable increases in heart rate and breathing.Using the same scale,vigorous-intensity activity is rated as a 7 or 8 and produces large increases in heart rate and breathing.Thus,physical inactivity,a concept that has also been included in this review,is defined as not meeting any of the following 2 criteria: 30 min of moderate-intensity physical activity on at least 5 days/week or 20 min of vigorous-intensity physical activity on at least 3 days/week.
Gender is also considered a risk factor for AD;two-thirds of AD patients are women.5This proportion is mainly attributed to the greater longevity of women over men, which makes them more susceptible to this and other age-associated diseases and syndromes.24Apart from this fact, if there is a real relationship between sex and AD risk,it is not clear.In the literature, epidemiological studies with controversial results can be found.25-27 Several results point to sex hormones as responsible, at least partially, for the higher incidence of AD in women. The important changes in sex hormone concentrations associated with a woman’s age,the role of sexual dimorphism in the neuronal structures development,the gene-by-sex interactions, and the increased specific immune response of women, have all been associated with an increased risk of AD.26
In this review,we mainly discuss the role of physical exercise as a therapeutic strategy for the treatment and prevention of AD.
2. Physical exercise and physiologic brain aging
Physical inactivity contributes to about 5 million deaths in the world each year from noncommunicable diseases.28The inverse relationship between a physically active life and the risk of suffering cognitive decline is widely documented,29and aerobic exercise training has been the most extensively used option for the study of the effect of physical activity in alleviating the negative impact of aging in cognitive function.29,30The first evidence was published in the 1970s, when it was shown that middle-aged sports practitioners had better response in cognitive tasks that involved a psychomotor component when compared with sedentary aged-matched subjects.31More recently, one study found a significant improvement in memory among middle-aged trained individuals,compared to sedentary subjects, when the Free and Cued Immediate Recall test was administered to both groups.32The positive impact of long-term exercise training by delaying the onset of physiologic memory loss suggests the effectiveness of exercise as a preventive strategy against age-related memory loss and neurodegeneration. However, it is worth mentioning that late-onset exercise interventions have also shown positive results in the delay of brain aging. For example, in a groundbreaking paper published in 2011, the authors found that 1 year of moderate-intensity exercise (40 min duration, 3 days/week) increased the size of the hippocampus, as well as increasing spatial memory,in healthy older individuals.33The anatomic changes induced by aerobic exercise have also been confirmed by other research groups. For instance, it has been found that 6 months of exercise (60 min duration, 3 days/week) is sufficient to increase both the gray and white matter in the anterior cingulate cortex,as measured by magnetic resonance imaging,in older,cognitively healthy subjects.34Longer aerobic exercise training protocols (3 years’ duration) in sedentary older women have shown improvements in reaction time,motor function, and cognitive processing speed, indicating that exercise is effective in reversing or at least slowing the age-related declines in motor performance and in speed of cognitive processing.35However, some evidence shows that aerobic exercise interventions do not always induce improvements in cognitive function in older subjects (60-80 years).36-38These contradictory results may be explained by the training duration, frequency, and/or intensity of the interventions.
The impact of resistance exercise on cognitive function has gained notice in the past few years.In a recent meta-analysis,more than 24 studies were reviewed that investigated the effects of weight lifting on different cognitive outcomes in older individuals. According to the results, resistance training has positive effects on measurements related to the detection of cognitive impairment and executive functions. However,resistance training has no effect on working memory measurements.39Although a high heterogeneity was observed in all analyses, the authors concluded that resistance training seemed to have positive effects on cognition. However,future research will need to determine why the effects are so variable.
From this first part of the review, we can conclude that exercise programs with components of both aerobic and resistance training, of moderate intensity, and lasting at least 45 min per session on as many days of the week as possible, are beneficial in terms of cognitive function in older healthy adults.40
3. Physical exercise and multimodal interventions for the treatment and prevention of AD
Dementia is by no means an inevitable consequence of reaching retirement age. There are lifestyle factors that may decrease, or increase, an individual’s risk of developing dementia.22Around 35%of dementia is attributable to a combination of 9 risk factors: low education level, midlife hypertension, midlife obesity, hearing loss, later-life depression,diabetes, smoking, social isolation, and, of course, low physical activity.41
A meta-analysis that included 16 studies with more than 160,000 participants found a 45% reduction in the risk of developing AD due to the regular practice of physical activity(hazard ratio=0.55, 95% confidence interval: 0.36-0.84,p=0.006).42In a sample of 716 older subjects followed for 3.5 years,similar results were found when assessing the risk of suffering AD.Those individuals with low daily physical activity levels were 53% more likely to suffer AD than those who reported more active lives (hazard ratio=0.477, 95% confidence interval:0.273-0.832).43
Although there are discrepancies,36,44-49the benefits of engaging in physical activities have also been seen in populations diagnosed with mild cognitive impairment (MCI) and AD. Several studies have found improvements in executive functions,memory,and cognitive tests in individuals with MCI who engaged in an aerobic exercise program.50-55Improvements in the cognitive function of individuals with MCI through physical activity are important in preventing the progression of the disease and in decreasing the number of AD in older people. In individuals diagnosed with AD, and, in general, at early stages of the disease, aerobic exercise alone, or accompanied with cognitive stimulation, induces improvements in some aspects of brain function,56-65although in some studies exercise was accompanied with cognitive situation.
Few studies have been published on the effects of resistance training in people with MCI or AD.44,66-68Prominent among them is the randomized, double-blind trial that included 100 people between 55 and 86 years of age with MCI.69In this study it was shown that 6 months of resistance exercise induced improvements in memory, attention, and executive functions. Moreover, those benefits persisted 12 months after the end of the intervention period.
Prevention through the promotion of changes in lifestyle in presymptomatic and predementia disease stages may have the potential for delaying one-third of dementias.70Engaging in physical exercise programs seems to be effective, but it is clearly not enough.Studies that examine multimodal interventions hypothesize that an integrated approach to addressing multiple risk factors for AD may be more successful than single-component interventions in producing benefits. Multimodal interventions often include changes in diet, physical activity,and cognitive training(Fig.1).
Several studies attribute to the diet a key role in delaying the progression of AD.Some of these studies have tested diets considered as heart-healthy,such as the Dietary Approaches to Stop Hypertension diet(DASH),Mediterranean-DASH Intervention for Neurodegenerative Delay diet (MIND), or the Mediterranean diet.71The inflammatory component of AD has been treated by supplementation with fatty acids,vitamins,flavonoids, polyphenols, probiotics, and dietary advanced glycation end products.72Ketogenic diets, which are protective in other neurological disorders,also seem to have great potential in the prevention and treatment of the disease.73In humans,few clinical trials have been carried out using ketogenic diets;instead, ketogenic agents have been used.74In animal models of AD,the increase in ketone levels in the body through intermittent fasting or supplementation with ketone esters have shown promising results.75,76
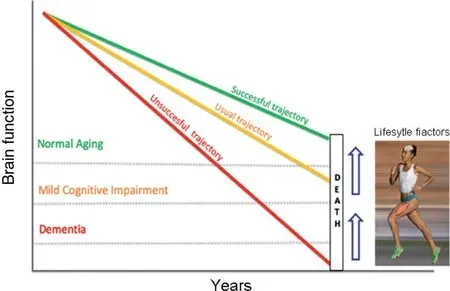
Fig. 1. Brain function in normal aging and Alzheimer’s disease is influenced by lifestyle factors.The usual trajectory for brain aging(orange line)indicates that, years before death, an individual shows signs of mild cognitive impairment. In some cases, that cognitive damage takes place many years before death and even leads to dementia(red line).By modifying lifestyle factors through multimodal interventions, an individual can delay the onset of cognitive impairment until a very advanced age(green line).
The Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability (FINGER), a multidomain intervention consisting of diet,exercise,cognitive training,and vascular risk monitoring, resulted in an improvement or maintenance of cognitive functioning in at-risk elderly people from the general population.77This trial was the first methodologically robust study showing that with a 2-year intervention,it was possible to reduce the risk of cognitive decline among the general elderly population, rather than solely with patients in a clinical setting.More recently,it has been found that engaging in physical activity and lowering vascular risk may have additive protective effects on delaying the progression of AD.22Greater physical activity and lower vascular risk independently attenuated the negative association of Ab burden with cognitive decline and neurodegeneration in asymptomatic individuals.78
4. Potential protective mechanisms of physical exercise on brain aging,from mice to humans
The beneficial effects of physical activity go beyond skeletal muscle and involve adaptations in other organs. Exercise causes changes in the brain at the anatomic, cellular, and molecular levels by inducing a cascade of cellular and molecular processes that promote different physiologic phenomena,including angiogenesis, neurogenesis, synaptogenesis, and stimulation of neurotrophic factors that enhance learning,memory, and brain plasticity(Fig. 2).53,60,79-84The availability of transgenic murine models that simulate the main neuropathologic characteristics of AD has enabled the study of the main protective mechanisms of exercise on brain aging.Among these mechanisms is an increase in cerebral blood flow(CBF)in several cortical and subcortical areas,85together with the decrease in the formation of Ab and the phosphorylation of the tau protein.86,87
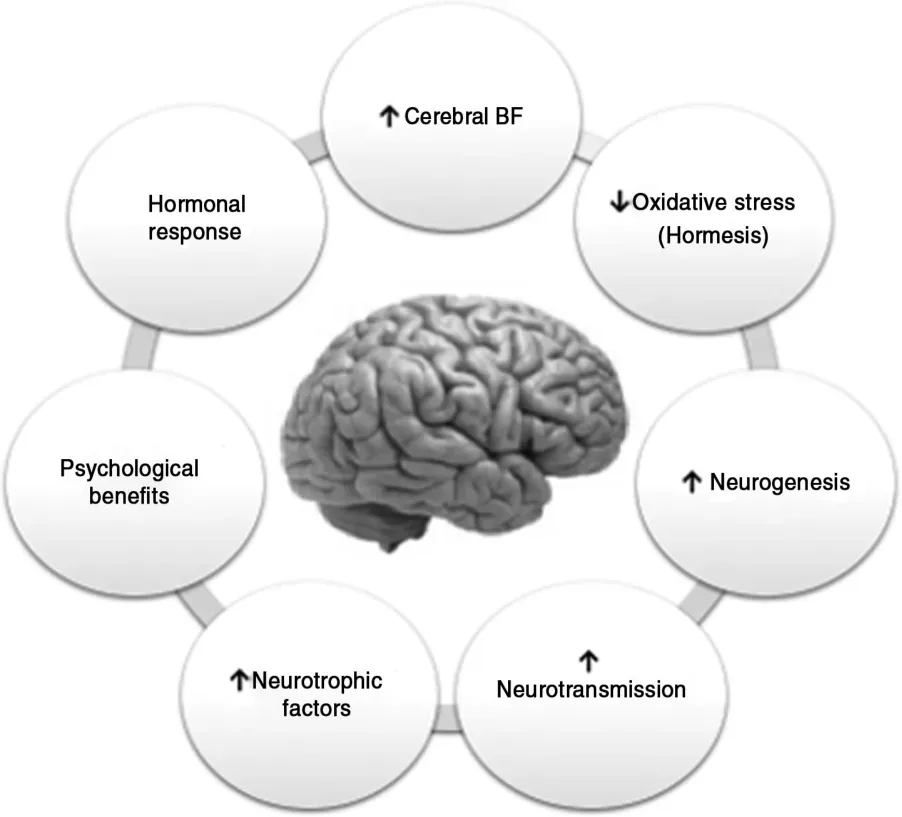
Fig.2. Potential protective mechanisms of exercise on brain aging.BF=blood flow.
5. Summary of the main mechanisms that exercise can activate at the brain level
5.1. b-Amyloid peptide,tau protein,and exercise
In transgenic mice models for AD,a decrease in Ab plaques and NFTs after both voluntary and forced exercise interventions has been found.In some cases,these findings have been accompanied by improvements in learning and memory.86-89 APP/PS1 are double transgenic mice expressing a chimeric mouse/human amyloid precursor protein (APP) (Mo/HuAPP695swe)and a mutant human presenilin 1 (PS1-dE9), both directed to central nervous system(CNS)neurons.In a recent study in double transgenic APPswe/PSEN1DE9 mice,10 weeks of voluntary exercise decreased both the load and the size of the Ab plaques,as well as the phosphorylation of tau in the hippocampus.Improvements in spatial memory, a decrease in hippocampal neuronal loss, and an increase in neurogenesis in the Cornu Ammonis 3(CA3)zone and the dentate gyrus were also reported in the study.90These results have been supported by studies in other AD transgenic mice models such as hPS2m (overexpress human Presenilin 2 mutant),89Tg-NSE/htau23 (overexpress human tau23 under the control of the NSE promoter),88Thy-Tau22 (human 4-repeat tau mutated at sites G272V and P301S under the control of Thy1.2 promoter),91P301S-tau(overexpress the P301S-mutant human tau gene),87and Tg2576(overexpress human APP 695).92It is assumed that a successful therapy for AD would both remove the pathologic hallmarks of the disease and provide some functional recovery.However,there are studies that have not found a decrease in Ab load and/or tau phosphorylation despite improvements in learning tasks and/or memory in the exercised mice.93-95A key factor with exercise interventions is to start them in an early pathologic state. Exercise cannot counteract the formation of plaques and the cognitive deterioration if the intervention is carried out after their appearance.86Moreover,it has been shown in mice models that voluntary exercise may be superior to forced exercise if certain aspects of the disease, such as plaque deposition and memory impairment,are to be reduced.92
Studies in humans have also found an inverse correlation between physical activity levels and the plasma and brain Ab load in elderly people without cognitive disorders.96,97Moreover, it has been found that a 6-month aerobic exercise intervention in individuals with MCI induced a 24%decrease in the plasma Ab1-42levels when compared with the levels found in the control group.50Jointly, all of these results indicate a potential role of exercise in modulating the Ab turnover.
5.2. Exercise and inflammation
The term “inflammaging” characterizes a widely accepted hypothesis that aging is accompanied by a low-grade chronic upregulation of certain proinflammatory responses. It is characterized by a relative decline in adaptive immunity and T-helper 2 responses and is associated with increased cellmediated responses.98Inflammaging has been considered to be a “prodrome” to AD and microglial malfunction, a common feature during aging.99
Exercise has important modulatory effects on immune function.100Systemically, physical exercise has been shown to have a positive effect on markers of inflammation,and recently those effects have been extended to the CNS.101
In the Tg2576 AD animal model,it was shown that 3 weeks of voluntary exercise were sufficient to decrease the concentration of Ab and the proinflammatory cytokines interleukin-1b(IL-1b) and tumor necrosis factor-a (TNF-a). These changes were accompanied by an increase in proteins related to the immune response, such as interferon-g and macrophage inflammatory protein-1a,in the hippocampus.102
The anti-inflammatory effects of exercise on the CNS have also been evaluated in older animals. Higher levels of hippocampal IL-10(the main anti-inflammatory cytokine)and lower IL-1b/IL-10, IL-6/IL-10, and TNF-a/IL-10 ratios have been found in rats exercised for 10 days.103Barrientos et al.104found that the long-term memory impairment in older rats injected with Escherichia coli(E.coli)intraperitoneally could be prevented when they had free access to running wheels.Along with these findings, voluntary exercise also prevented the reduction in brain-derived neurotrophic factor (BDNF)expression in the CA1 zone of the hippocampus. Finally,the microglia of the exercised rats had a lower inflammatory response than the control rats, as measured by the expression of TNF-a, IL-1b, and IL-6. These findings highlight the capacity of exercise to modulate inflammatory responses on CNS and reinforce its potential in minimizing the risk of suffering diseases related to neuroinflammation,such as AD.
Particularly in elderly people, regular physical activity has been shown to have a positive effect in the reduction of inflammatory markers such as Creaction protein, IL-6, and TNF-a105-110at the systemic level.In many cases,this has been associated with better performance in cognitive tests in both cross-sectional111-113and longitudinal studies.114-117
Aerobic exercise lasting more than 2 weeks118-121has been shown to improve the immune system in healthy elderly people by increasing the activity of the natural killer cells,the proliferation of T lymphocytes, hematopoietic stem cells, and endothelial progenitor cells.However,it is noteworthy that the results achieved with resistance exercise interventions have been more heterogeneous.122
5.3. Neurotrophins,cognitive function,and exercise
Neurotrophins are growth factors belonging to the family of neurotrophic factors, which regulate axonal growth, synaptic plasticity, neurotransmission, hippocampal neurogenesis, synaptic protein expression,and long-term potentiation.123-128
Among neurotrophins,BDNF has been extensively studied,and its relationship with exercise and cognitive function has been widely established.32,50,129-135 The brain synthesizes about 75% of BDNF under normal conditions. During prolonged exercise,this synthesis is increased by 2-to 3-fold,and there is evidence indicating that circulating BDNF levels correlate with brain tissue BDNF levels.132,136
Exercise provides cognitive benefit in 5xFAD mice(express human APP and PSEN1 transgenes with a total of 5 AD-linked mutations: the Swedish (K670N/M671L), Florida(I716V), and London (V717I) mutations in APP, and the M146L and L286V mutations in PSEN1), a mouse model of AD, by inducing both adult hippocampal neurogenesis and by elevating the levels of BDNF.137This combination seems to generate an adequate brain environment for the maintenance and survival of the new neurons in regions of the brain affected by AD. The induction of adult hippocampal neurogenesis in combination with the elevation of BDNF levels successfully mimic the beneficial effects of exercise in AD mice.137However,the induction of hippocampal neurogenesis alone did not benefit cognition or AD markers. Exercise has also shown its effectiveness on cognitive function and BDNF levels in mice models of accelerated aging.130Four weeks of moderate exercise were sufficient to improve recognition memory and increased hippocampal BDNF expression in 13-month-old mice.
Low levels of BDNF have been found in brains of people with AD,138,139which supports the hypothesis that improving its production may be an effective alternative that delays the onset of the disease. In humans, several studies indicate that both acute and chronic exercise140-146contribute to an increase in the peripheral levels of BDNF,and,in some cases,it is related to gains in cognitive function.131,147-149Moreover,aerobic exercise-induced increments in hippocampal volume are associated with greater serum levels of BDNF in cognitively healthy older individuals,33and high serum levels of BDNF have been associated with low risk of AD.150
The pathways responsible for the synthesis and release of BDNF in AD patients seem to be susceptible to stimulation with exercise. In fact, one bout of acute aerobic exercise increased the BDNF plasma levels in patients with AD and in healthy controls. Additionally, BDNF was associated with their physical activity levels.151
5.4. AD,CBF,and exercise
Aging has been associated with progressive losses in cognitive function and CBF.152-156It has been shown that the rate of decrease with age of the CBF is 0.35%-0.45% per year in middle-aged and elderly subjects (Fig. 3).157,158This leads to an accelerated decline in cognitive function and an increased risk of suffering dementia in the general population.159
Although the cause of the CBF decrease in aging is not entirely clear,it has been postulated that changes in the density and elasticity of cerebral blood vessels,as well as the degeneration of pericytes and a reduction in the activity and number of neurons,could explain it.161,162
Compared with healthy people, individuals with AD show a decrease of up to 40% in the CBF. Regions such as the precuneus, the hippocampus, the posterior cingulate gyrus,and the temporal, occipital, and parietal lobes are mainly affected.163-167
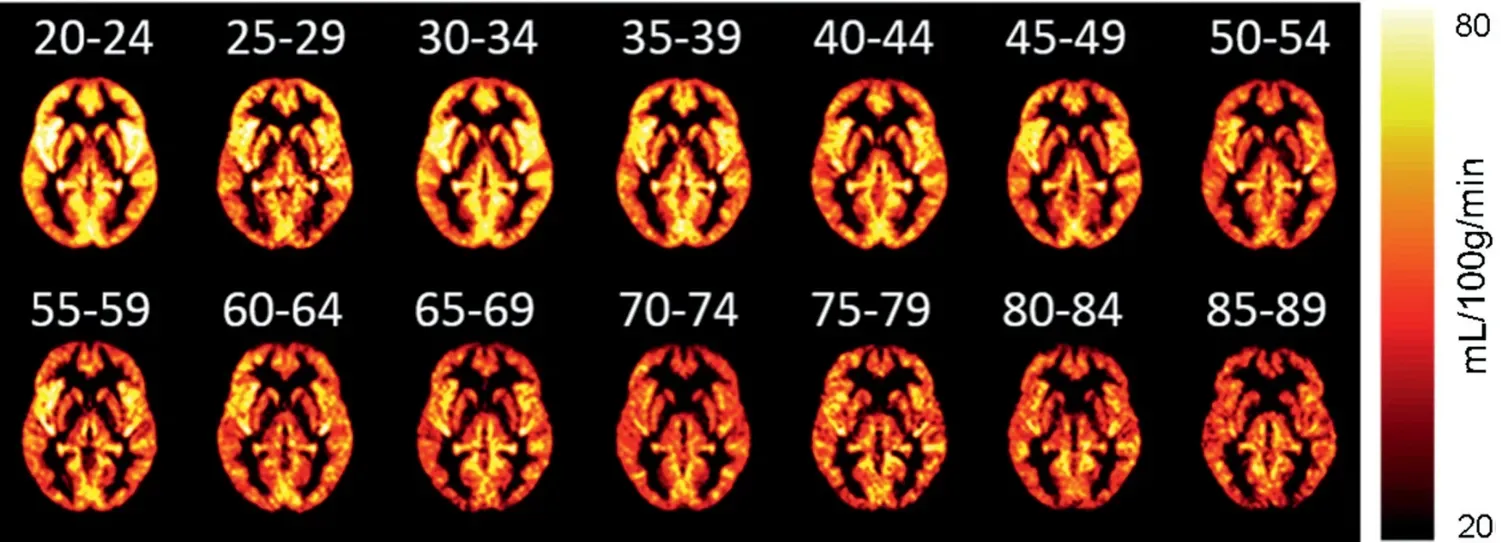
Fig. 3. CBF by age groups(at an interval of 5 years), measured by MRI(De Vis et al.,160 used with permission of John Wiley and Sons). CBF=cerebral blood flow;MRI=magnetic resonance imaging.
In animal models, it has been shown that the soluble form of Ab protein can accumulate in cerebral blood vessels(which is known as amyloid angiopathy), generating a decrease in CBF and a vasoconstriction effect,possibly affecting neuronal activity.168,169Intra-arterially injected solubilized Ab1-40in rats of 7-8 months of age decreased CBF and increased vascular resistance in the cerebral cortex of the animals, indicating that Ab could contribute to the hypoperfusion observed during AD.170
In older adults, the regular practice of exercise has a positive effect both on peripheral endothelial function171and on the increase of CBF in areas such as the hippocampus.156,172,173In middle-aged, cognitively healthy subjects, even short-term exercise programs, such as 3 h of aerobic exercise per week for 12 weeks,are sufficient to improve CBF at rest in regions such as the anterior cingulate and the hippocampus.174,175However, even in physically active people,short periods of inactivity can decrease CBF in up to 8 regions of the brain,including the hippocampus.176Thus,CBF is sensitive to small changes in people’s lifestyle,thus making it necessary to maintain a regular practice of exercise to preserve brain health.
Regarding AD patients and exercise, the results from studies have not been consistent.177For instance, in a study,exercise did not lead to any improvements in CBF,178concentrations of Ab,total tau,or phosphorylated tau in the cerebrospinal fluid of people with AD.179This indicates that,although functional parameters are still likely to be positively affected in people with AD, changes in brain function may require an adjustment in the different components of the load,such as the duration of exercise sessions and the frequency,intensity, and type of exercise during the intervention.
Finding mimetics of physical exercise for those patients who have very compromised functionality is not easy,because physical exercise is a very systemic intervention and targets at several potential causes of AD.The possibility of using molecular mimetics,such as 5-aminoimidazole-4-carboxamide ribonucleotide(AICAR),is known to only improve brain function transiently180and does not achieve the same positive effects as,for instance,running.Another option would be to use neuromuscular electrical stimulation or vibration in people who are unable to perform physical exercise, but this has not yet been tested in AD patients.181
6. Conclusion
Promoting changes in lifestyle in presymptomatic and predementia disease stages may have the potential for delaying one-third of dementias worldwide. Exercise modulates Ab turnover, inflammation, the synthesis and release of neurotrophins, and CBF. Multimodal interventions that include the adoption of an active lifestyle should be recommended for older populations.
Acknowledgments
This work was supported by the following grants: Instituto de Salud Carlos III and co-funded by FEDER (Grant number PIE15/00013); SAF2016-75508-R from the Spanish Ministry of Education and Science(MEC);CB16/10/00435(CIBERFES);PROMETEOII2014/056 from Conselleria,de Sanitat de la Generalitat Valenciana and EU Funded CM1001 and FRAILOMICHEALTH.2012.2.1.1-2; and ADVANTAGE-724099 Join Action(HP-JA)3rd EU Health Programme and DIALBFRAIL-LATAM(825546 H2020-SC1-BHC).
Authors’contributions
ADR and GOG performed the literature search and review and wrote the manuscript;ASP,CAC,FM,CGL,AGC,CBL,AC, and EGD analyzed and discussed the data and reviewed the manuscript; MCGC and JV designed and supervised the review,secured funding,and wrote the manuscript.All authors have read and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interestsThe authors declare that they have no competing interests.
杂志排行

Journal of Sport and Health Science的其它文章
- The role of mitochondria in redox signaling of muscle homeostasis
- The roles of microRNA in redox metabolism and exercise-mediated adaptation
- Exercise-induced oxidative stress:Friend or foe?
- Epidemic-specific social capital and its impact on physical activity and health status
- Team sport,power,and combat athletes are at high genetic risk for coronavirus disease-2019 severity
- Exercise immunology:Future directions