Proton beam therapy of periorbital sinonasal squamous cell carcinoma:Two case reports and review of literature
2020-09-14
Yi-Lan Lin,Department of Radiation Oncology,Rinecker Proton Therapy Center,Munich 81371,Germany
Abstract
Key words:Proton beam therapy;Intensity modulated proton therapy;Sinonasal malignancies;Squamous cell carcinoma;Orbital exenteration;Case report
INTRODUCTION
Sinonasal malignancies (SNMs) occur very seldom and account for only 3% of all head and neck cancers and 1% of all malignant tumor diseases,with a peak incidence in the 5thto 7thdecades and predominance among males.The prodromes,such as nasal congestion and discharge,epistaxis and lacrimation,are often misjudged as rhinosinusitis and consequently neglected by both the patients and physicians.At the presence of late symptoms like facial edema,sensory failures and cranial neuropathy,the patient is first referred to sinonasal endoscopy and imaging[1].At this time,however,over 50% of the cases are diagnosed in an advanced stage (T3/4),with poor prognostic outcome[2,3].Female sex,nasal cavity tumor,adenocarcinoma and low clinical stage have been identified as positive predictors[4].Among the epithelial tumors,the squamous cell carcinoma (SCC) is the most common (80%),followed by adenocarcinoma.Both histological subtypes are etiologically associated with occupational exposure to wood,leather and textile dusts,organic solvents,welding fumes,arsenic,etc.[5,6].
For sinonasal (SN) SCC (SNSCC),higher age and tumor stage are adverse prognostic factors,while surgery has been shown to improve survival significantly[3].Based on the analysis of the United States National Cancer Database,surgical approach represents the therapeutic mainstay of SNSCC,whereas neoadjuvant chemoradiotherapy (CRT) is associated with improved R0 resectability[7].Although recent retrospective studies have validated superior outcomes by multimodality,the optimal combination and sequence of surgery,radiotherapy (RT) and chemotherapy remain controversial[7-9].Furthermore,locally advanced SNM with orbital invasion is actually challenging for clinicians due to the complexity of complete gross resection,that largely requires an orbital exenteration and consecutive aesthetic restoration by means of plastic surgery,prosthesis and rehabilitation.Given the correlated burden to the patient’s psyche and quality of life,the information about prognosis,multimodal therapy approaches and supportive adjuvant measures should be comprehensively discussed between the patient and attending physicians before the therapeutic decision[10].
CASE PRESENTATION
Case 1
Chief complaints:A 62-year-old German male presented with a relapsed tumor in the nasal septum,extending to dual-sided ethmoidal sinuses and abutting frontal skull base,as well as a suspicious lymph node metastasis in the left parotid gland,in an interval of 7 mo after the primary surgery to address a nasal SCC.
History of present illness:The tumor recurrence was confirmed by a sampling excision of nasal mucosa in August 2014,which showed moderately differentiated keratinizing SCC.According to the assessment of otorhinolaryngology,a resection was possible in principle but would have been accompanied by enormous physical defect and face distortion due to the requisite removal of bilateral medial canthi and glabella.The patient rejected the surgery and tried to gain information about RT.Consultation with the radiation oncology team of the university hospital close to his home led to recommendation of a combined CRT or proton beam therapy (PBT).The patient preferred the latter,after he became educated about the more vehement toxicities of conventional RT with photons,such as necessity of artificial nutrition owing to pharyngitis,malfunction of sense of smell and taste,deafness of left ear,and blindness in 2-5 years.Consequently,he contacted three particle therapy institutes in Germany but obtained refusal from two for the following reasons:The benefit of particle therapy for SNSCC was not completely clarified and could not be offered out of clinical trials.Besides,the sinonasal airspaces causing uncertainties in the treatment planning was unfavorable for the exact calculation of dose distribution in the target volume.Therefore,a conventional RTviamodern technique [(e.g.,intensity-modulated RT(IMRT)] with concomitant platinum-based chemotherapy was recommended.On the contrary,Rinecker Proton Therapy Center was the only one of the three consulted institutes which accepted the patient for PBT.
History of past illness:The nasal SCC had been initially noted in October 2013 by recurrent epistaxis with swelling and enlargement of the nose and foreign body feeling.Endoscopy demonstrated an exophytic lesion in the nasal septum,reaching to the nasal floor.Imaging examinations,including computed tomography (CT) scan of head,neck and thorax and ultrasound of neck,showed a tumor perforating the anterior nasal septum with infiltration of nasal bridge and destruction of nasal bone,emphasized on the left side,as well as a suspicious Warthin’s tumor in the left parotid gland.In January 2014,the patient underwent a partial nasal ablation (Figure 1A) and selective neck dissection (level I-III) on both sides,with postoperative tumor stage determined to be pT2 pN0 G3 R0 cM0.
Personal and family history:The patient was in good general condition and worked at his own gym.Apart from chronic nicotine abuse (at least 50 pack-years),there was no relevant comorbidity known.
Physical examination upon admission:There was an obvious substance defect in the middle nasal portion with tumorous skin thickening all-round after the partial amputation (Figure 1B),so that the original nasal epithesis no longer fit within.The common clinical examination yielded normal findings.
Laboratory examinations:No special laboratory test was arranged.
Imaging examinations:The magnetic resonance imaging (MRI) prior to PBT showed intensive contrast enhancement in the central nasal cavity with soft tissue swelling of nasal bridge until nostrils,measuring approximately 29 mm × 15 mm × 22 mm,abutting the frontal sinus and skull base (Figure 2A-C).The ethmoidal air cells were partially involved by tumor infiltration as well as mucosal swelling.Apart from at least one strong enhancing nodule of 8 mm × 11 mm diameter at the lower pole of left parotid gland,no pathological cervical lymph node was detected.To complete the restaging examination,the patient underwent additional positron emission tomography with 2-deoxy-2-fluorine-18-fluoro-D-glucose (18F-FDG-PET/CT).Both suspicious tumor recurrences in the nasal bridge and left parotid gland exhibited a maximum standardized uptake value [SUV(max)] of 5.2 and 2.7 in each (Figure 3A-C).Although the parotid lesion was initially interpreted as Warthin’s tumor,which is FDG-avid on principle,this finding was assessed by our specialist of nuclear medicine and radiology as highly suspicious of intraparotid lymph node metastasis.
Final diagnosis:Recurrent periorbital SNSCC,tumor stage rpT4a rpN1 G2 cM0.

Figure1 Patient’s images prior to proton beam therapy.
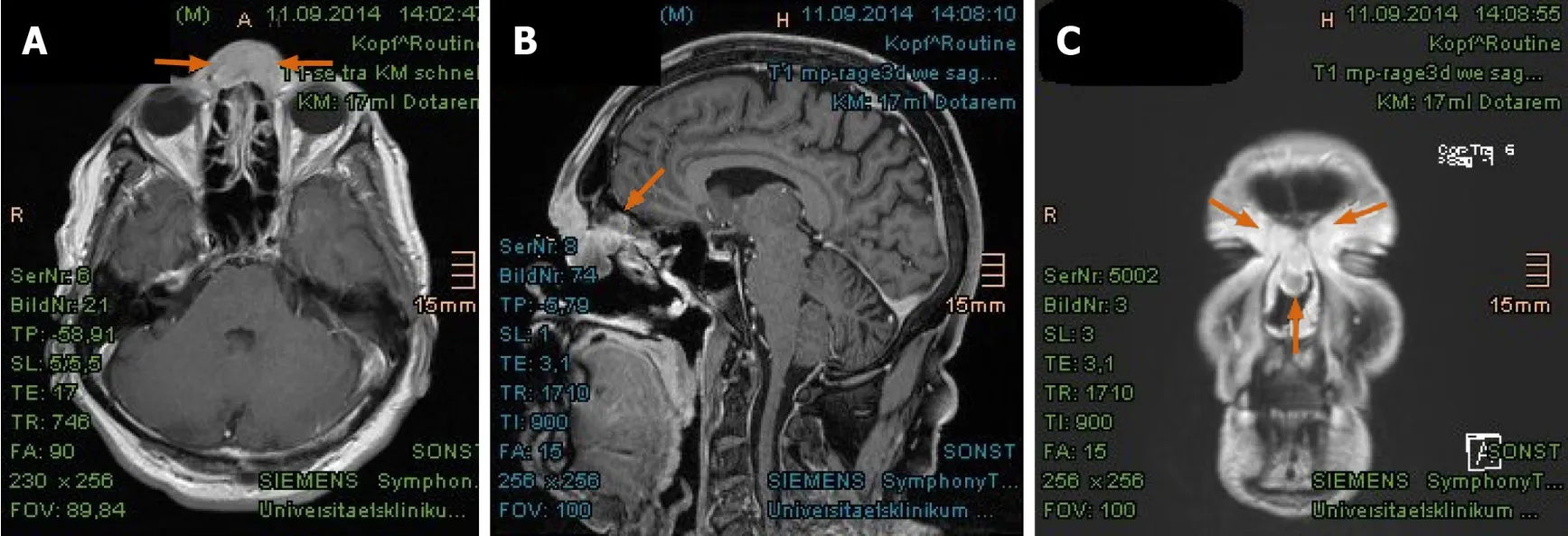
Figure2 Magnetic resonance imaging from September 2014 revealed tumorous enhancement in the nasal bridge abutting frontal sinus and skull base.
Treatment:At express request due to continuation of working during the treatment,the patient was treated with hyperfractionated accelerated scheme within 37 d,from October to December 2014.The informed consent was obtained prior to the initiation of the treatment.The PBT was delivered in 44 fractions and single dose of 1.50 Gy[relative biological effectiveness (RBE)],twice a day with minimum interim of 4 h,at a total dose of 66.00 Gy (RBE) to the tumor recurrences in the nasal bridge and left parotid gland.Simultaneously,the left cervical lymphatic drainage,including nodi lymphatici parotidei,submandibulares and jugulares superiores,received 52.80 Gy(RBE) in total,with single dose of 1.20 Gy (RBE).The entire target volume was irradiated from three gantry angles of 30°,330° and 80° using the pencil beam scanning technique (Figure 4A).After 28 fractions,the safety margin to both eyeballs was reduced because of incipient tumor shrinkage,noticed by weekly-performed lowdose CT scans,as well as for the purpose of better eye sparing (Figure 4B).Since the statutory health insurance refused to reimburse the cost of PBT,the patient deliberately declined a concurrent chemotherapy,in order to demonstrate afterwards that he was exclusively cured by PBT alone.
Outcome and follow-up:Generally,the patient tolerated PBT well and drove 300 km daily between our center and his home.At the beginning of the treatment,he complained of intumescence of the nose,with boring pain in the evening,that was mitigated by anti-edematous medication (dexamethasone 8-16 mg per day) and analgesics.In the further course,he developed increasing radiation dermatitis with superinfection in the middle face,especially at the inner corners of both eyes,corresponding to grade 2-3 by Common Terminology Criteria for Adverse Events(commonly referred to as CTCAE).At the final examination,the skin finding was improved by intensified skin care and disinfectant measures taken immediately after daily irradiation.The patient denied visual impairment and dry eyes as well as dysphagia and changes in taste and smell.Xerostomia only occurred temporarily.
In the first follow-up,at 3 mo after the PBT,MRI scan displayed a significant tumor reduction in the nasal bridge (Figure 5A-C).At this stage,it was normally hard to distinguish between residual tumor and inflammation tissue.Nonetheless,the biopsy from the nasal bridge revealed a chronic granulating mucosal ulcer with no evidence of malignancy.As post-radiogenic changes,the mucosa of the nasal cavity and paranasal sinuses was still distinctly swollen,accompanied by fluid accumulation in the left petrous bone.Subjectively,the patient reported,first,deterioration of moist desquamation after finishing the PBT,which was alleviated by use of a special ointment mixture containing cortisone (prescribed by his dermatologist) after 10 d.Second,he complained of excessive lacrimation,lymphedema of the face and hypacusis on account of post-radiogenic tympanic effusion in the left ear.Other late toxicities,such as visual,olfactory and gustatory disturbances and dry mouth,were absent.

Figure3 Positron emission tomography with 2-deoxy-2-fluorine-18-fluoro-D-glucose/computed tomography validated tumor recurrence in the nasal bridge and left parotid gland.
The PET/CT and MRI scans performed at 8 mo after PBT showed a complete tumor remission (Figure 6A-F).The lymphedema in the facial and left retroauricular area regressed by frequent lymphatic drainage massage.Except sustained reinforced shedding of tears,no sensory impairment was present,and the epithesis of nose fit in again.At the 23rdmo after PBT,the patient reported bilateral cataracts,dry eyes,permanent loss of medial eyebrows,eyelashes and nasal hair,and use of lubricating eye drops steadily.Since a tumor recurrence was continuously excluded in the PET/CT and MRI scans (Figure 7A-E),the patient was accepted to undergo a nasal reconstruction in five sessions,carried out between 2016-2017,in cooperation with the otorhinolaryngology and plastic surgery departments[40](Figure 8A-C).To date,the patient is content with the cosmetic result (Figure 8D) and remains free of tumor recurrence as well as visual and auditory impairment.Despite his objection in view of the successful treatments,the health insurance still declines to refund the expenditure of PBT and reconstruction surgery.
Case 2
Chief complaints:A 59-year-old Polish female was diagnosed with a space-occupying lesion of the right lacrimal sac adjoining nasal cavity and maxillary sinus in the ophthalmology,initially in summer 2017 (Figure 9A).
History of present illness:The patient was referred to the otorhinolaryngology department for the further examinations.Owing to lack of an apparent tumor in the nasal cavity,presence of ulceration and unfavorable curvature of the nasal septum,instead of an endoscopic approach,the histopathology was obtained in January 2018 by an open biopsy through the lower eyelid,submitting moderately differentiated keratinizing SCC.Because the tumor invaded the medial orbit and adjacent paranasal sinuses (Figure 9B and C),an orbital exenteration on the right was defined as the therapy of choice but was rejected by the patient.She then contacted our center for the purpose of organ preservationviadefinitive RT with PBT.

Figure4 Treatment plans of proton beam therapy with isodose distributions in all three planes and dose-volume-histogram.
History of past illness:Not specified.
Personal and family history:The patient was in reduced general condition,being wheelchair-bound (Karnofsky Performance Score 60) by rheumatoid arthritis and on long-term treatment with methotrexate.
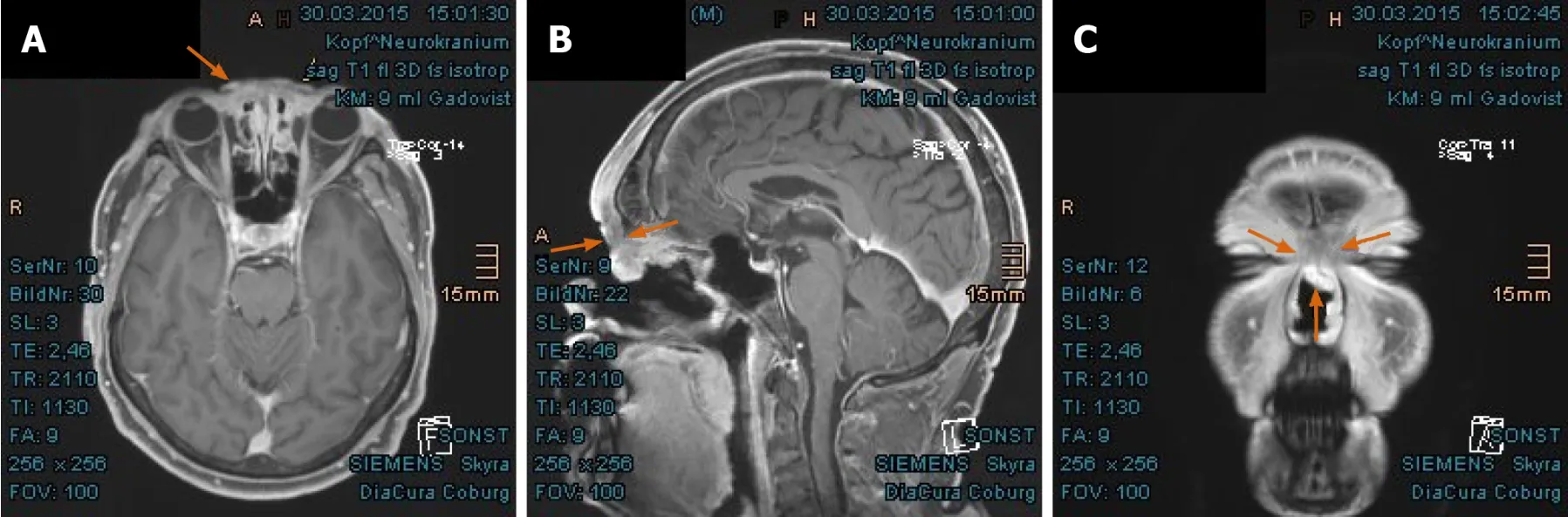
Figure5 Significant shrinkage of recurrent tumor in the nasal bridge with mucosal swelling in the first follow-up at 3 mo after proton beam therapy.
Physical examination upon admission:The patient presented with a bean-like flushed elevation inferiorly to the medial canthus of the right eye (Figure 10).The cervical lymph nodes were not as enlarged as to be palpable.No suspicious findings of tumor spread were apparent in the common clinical examination.
Laboratory examinations:No special laboratory test was arranged.
Imaging examinations:The MRI scan in February 2018 demonstrated nodular progress of the naso-orbital tumor up to 3.7 cm × 2.5 cm × 2.5 cm with bony destruction of the right infero-medial eye socket,possible invasion of the muscle cone and shift of the right eye to apico-lateral (Figure 11A and B).Furthermore,the tumor penetrated the neighboring ethmoidal sinus and nasal cavity with involvement of turbinates as well as the antero-medial recess of right maxillary sinus and facial soft tissue in the naso-labial fold and zygomatic area (Figure 11C-E).The18F-FDG-PET/CT revealed an increased uptake [SUV(max):12.0] of the multi-compartment SCC in splanchnocranium without definite evidence of metastasis (Figure 12A and B).
Final diagnosis:Periorbital SNSCC,tumor stage cT4a cN0 G2 cM0.
Treatment:The patient has undergone a normofractionated PBT in 33 fractions,from February to April 2018.The informed consent was obtained prior to the initiation of the treatment.The primary tumor manifestation was treated with single dose of 2.10 Gy (RBE) at a total dose of 69.30 Gy (RBE),while the right lymphatic basins including buccofacial,parotideal,retropharyngeal,submandibular and suprajugulary nodal stations received 59.40 Gy (RBE) overall with a single dose of 1.80 Gy (RBE).Under immobilization with head,neck and shoulder mask and vacuum cushion (BlueBAGTM;Medical Intelligence,Schwabmünchen,Germany),the target was irradiated from two gantry angles of 5° and 300° using the pencil beam scanning technique (Figure 13).Because of lack in remarkable change of tumor size (according to weekly-performed low-dose CT scans),adaptation of the treatment plan was not required.Given the aforementioned comorbidity,simultaneous chemotherapy was dismissed by the patient.
Outcome and follow-up:During the treatment,the patient developed moderate dysphagia,odynophagia,nasal congestions,and conjunctivitis.The greatest effect was painful radiation dermatitis (CTCAE grade 2-3) on the right cheek,extending from the right orbit to the lips.In the first follow-up at 3 mo after PBT,the patient reported significant amelioration of pharyngitis,dermatitis,and swelling of the nasal mucosa.The motility disorders of eye muscle regressed as well.In the first MRI scan in June 2018,the tumor mass was found to have dwindled considerably (Figure 14A-D).The consequent control at 8 mo and 14 mo showed complete tumor remission (Figures 15A-D,and 16A-D).As late toxicities,telangiectasia on the right infraorbital fold and cataract of the right eye were indicated at 18 mo after the PBT (Figure 17).The first was corrected by laser skin treatment,while a cataract surgery is still pending as of the writing of this report.Apart from nasal mucosa dryness,repeated conjunctivitis and right nasolacrimal duct obstruction,the patient is continuously free of tumor recurrence and radiation-related symptoms to date.

Figure6 Complete tumor remission demonstrated in the positron emission tomography with 2-deoxy-2--fluorine-18-fluoro-Dglucose/computed tomography and magnetic resonance imaging at 8 mo after proton beam therapy.
DISCUSSION
SNSCC is not only related to occupational exposures,as mentioned above;in a population-based case-control study,tobacco smoking emerged as a strong risk factor for nasal cancer,with 60% increased risk in ever-smokers and an increment of 6%annually[11].Smoking also favored malignant transformation and relapse of sinonasal inverted papilloma after surgical resection[12,13].Similar to pharyngeal and cervical SCC,the impact of human papillomavirus (HPV) on the carcinogenesis and prognosis of SNSCC was investigated progressively.HPV positivity is more common in SCC of nasal cavity and nonkeratinizing SNSCC,yielding improved overall survival[14,15].With reference to this,both cases presented herein were not attributed to professional exposures,as the HPV status remained unknown because of missing testing at the time of tumor diagnosis.Nevertheless,the patient with recurrent nasal SCC showed long-standing smoking habits,and the other with right periorbital SCC was under long-term immunosuppression with methotrexate,that is significantly associated with various malignancies[16].
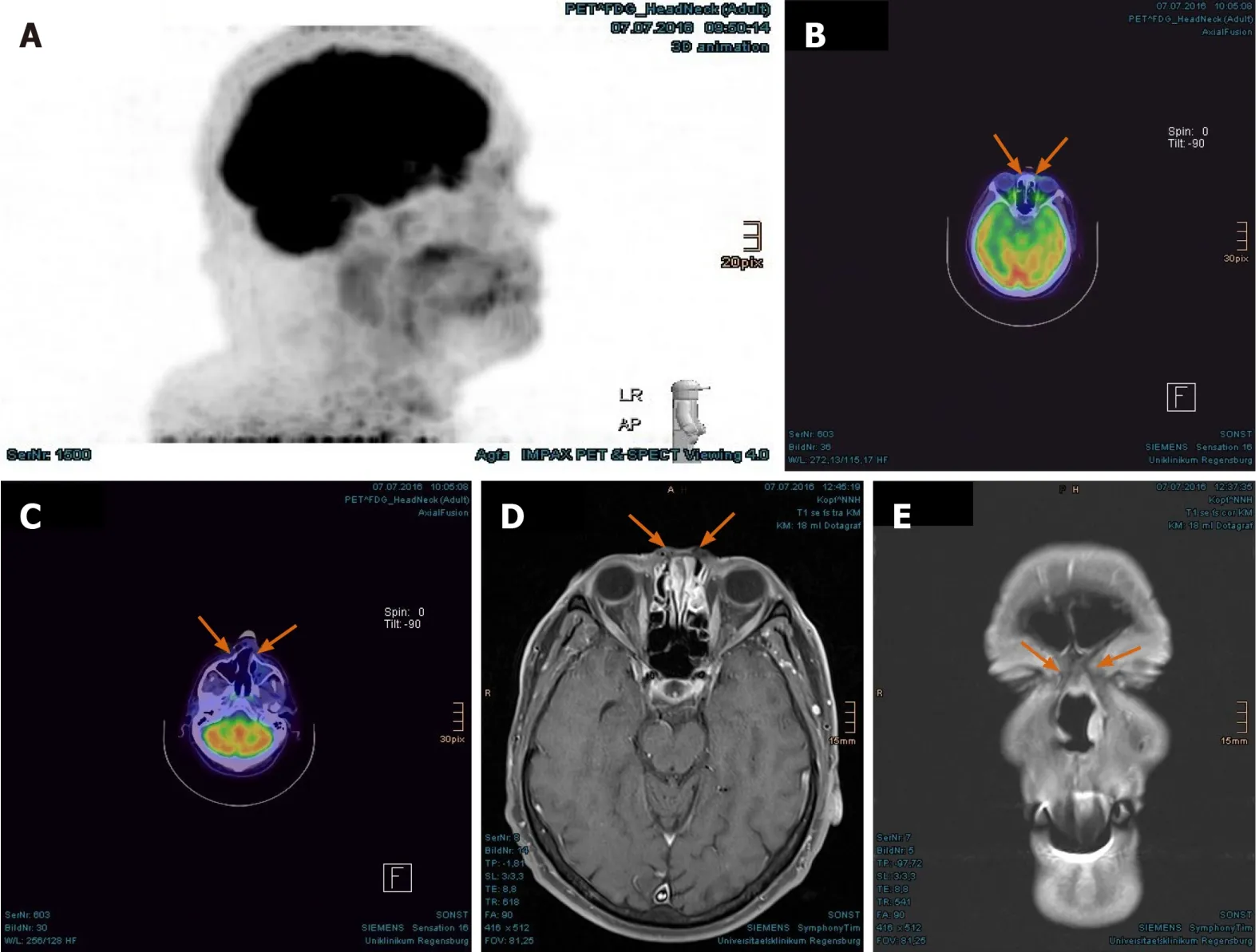
Figure7 Persisting tumor remission evidenced in the positron emission tomography with 2-deoxy-2--fluorine-18-fluoro-Dglucose/computed tomography and magnetic resonance imaging at 20 mo after proton beam therapy.
SNSCC is typically earmarked by bony destruction of the adjoining sinus walls and oftentimes accompanied by invasion of the orbital wall,infratemporal fossa,skull base and contralateral site,owing to delayed diagnosis.Besides,complex anatomy and diverse normal variants of the sinonasal tract aggravate the identification of tumor origin and extension[17].In case of tumor invasion of orbit,orbital exenteration - one of the most face-deforming operations - with removal of all the orbital contents,including eyelid and periosteum,is indicated to achieve better survival outcomes[18,19].Flaps,such as temporoparietal,galeal,free gracilis and free vastus lateralis musculocutaneous flap,are available for the reconstruction of defects;however,they should be employed with special diligence,due to the known comorbidities and postoperative complications[20,21].In the recent publications,there is a trend of eyesparing surgery without previously assumed survival disadvantages,especially in combination with adjuvant RT[22-25].
In the past few decades,there have been progressions in endoscopic endonasal surgery,microvascular reconstruction,RT,and systemic therapy.Even though surgery,with or without subsequent RT or CRT,remains the standard regime in most of the cases,Cracchioloet al[26]pointed out that the choice of therapeutic strategy was influenced by multiple tumor and non-tumor factors,stating apparent deviation from the National Comprehensive Cancer Network guidelines for the treatment of SNSCC.When utilizing a primary surgical approach,constant tumor factors and variable treatment factors,preeminently negative margin resection,were associated with improved survival.Additionally,patients with advanced tumor stage and positive margin resection profited significantly from adjuvant RT or CRT.
Concerning the regional metastases of SNM,levels I,II and III,and retropharyngeal lymphatic basins are frequently involved.Notwithstanding,the accurate assessment of elective nodal treatment in clinically N0 neck is fastidious,with an estimated risk for occult disease of 10%-20% or more.Notably,in tumor stage III-IV of SNSCC,elective neck irradiation should be intended in absence of selective neck dissection[27].In a retrospective review,Pecket al[28]identified the histologic types of SNM as the most impacting factors in predicting regional metastases,whereas the invasion of adjacent structures like dura,infratemporal fossa,palate and facial soft tissue was associated with increased occurrence of regional metastases.Taking this into account,we had decided to perform an elective nodal irradiation of the ipsilateral neck for both patients,surrendering an effective locoregional control and adequate tolerability.
Because of the rare occurrence and heterogeneous histologic subtypes and primary sites of SNM,there have been no randomized clinical trials to compare the various treatment modalities.In principle,early stage tumor is adequate to be managed with surgery alone,while locally advanced disease requires multimodality approaches.For patients who refuse up-front surgery,a RT-based approach is a legitimate option as well.In view of rapid growth and aggressive local spread of SNSCC to the neighboring organs at risk,such as optic nerves,eye globes,orbitofrontal and temporopolar cortex,as presented in our case report,sufficient local control (LC) is crucial for improved survival.Among SNMs,SCC incidentally seems to submit lower survival rates in comparison to other histologies[29,30].Novel development of RT technique,above all PBT and carbon ion therapy (CIT),should be generally considered to ameliorate treatment outcomes,to prevent long-term radiation-induced toxicities,and to facilitate organ preservation.Although photon irradiation stays the RT paradigm,more and more particle therapy institutions,mainly in the United States and Japan on account of generous availability,have delivered convincing results in the treatment of SNM[29-34].In their multi-institutional Proton Collaborative Group registry study,Yuet al[30]reported promising outcomes of 69 patients with SNM treated with PBT predominantly,which was provided as de novo RT or reirradiation in curative intention.Late ≥ grade 3 toxicities,such as vision loss and symptomatic brain necrosis,were not notified.

Figure9 Continuously growing tumor lesion in the right lacrimal sac invading the adjacent orbit and sinonasal spaces,presented as magnetic resonance imaging.

Figure10 “Case 2” patient’s image showing a tumorous nodule beneath the medial canthus of the right eye.
As recapitulation,the advantages of charged particle therapy are known to be comparatively low entrance dose and minimum exit dose,according to the physical feature of PBT and CIT,the so-called Bragg peak,as well as higher RBE and linear energy transfer than photons,which is utterly relevant for treating radioresistant tumor histologies.Based on the privileged physical and biological characteristics,the sophisticated amendment of dose distribution may provide superior conformality of target coverage with feasible dose escalation.Particularly,locally advanced,unresectable gross tumors may benefit from higher dose regimes.Toyomasuet al[33]reported 3-year/5-year overall survival and LC rates of 56.2%/41.6% and 54.0%/50.4%in the largest retrospective study of SNSCC treated with particle therapy alone.Of the patients,over one-third had unresectable disease,while almost half of the entire cohort obtained 65.0 Gy (RBE) in 26 fractions.Another study dealing with dose-intensified,hyperfractionated PBT to SNM with or without concurrent chemotherapy[29]also showed magnificent 3-year LC rates (of 90% for gross total resection and PBT,61% for primary PBT,and 59% for patients with gross residual disease).Analogous to our patient in “Case 1”,these patients obtained 1.20 Gy (RBE) twice daily,to a median total dose of 73.80 Gy (RBE).The incidence of ≥ grade 3 late toxicities was 24%,and in another study with CIT of SNM,the high-grade late toxicities occurred in 17% of the cohort[34].
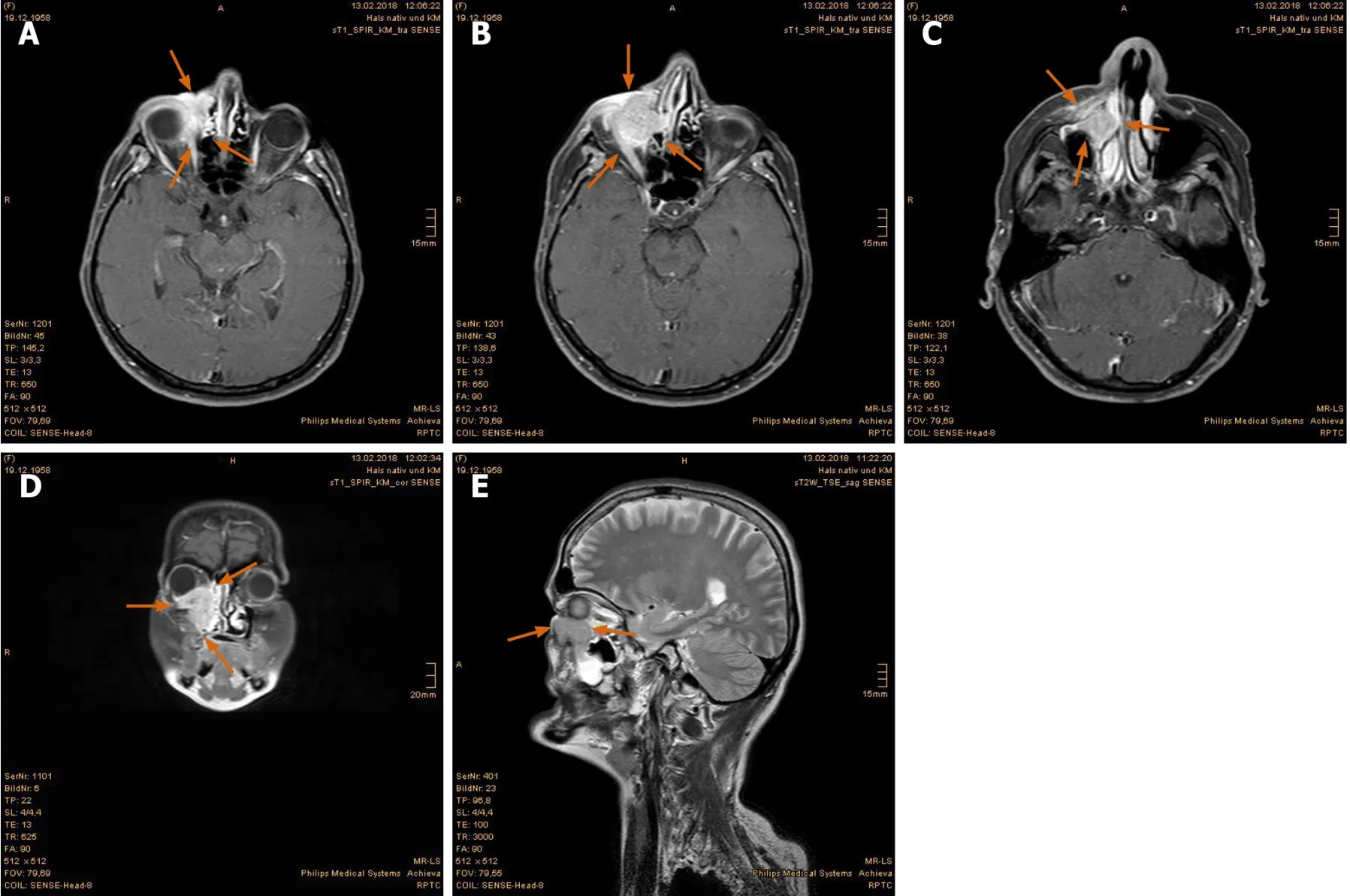
Figure11 Magnetic resonance imaging prior to proton beam therapy.
On the other hand,the utility of dose escalation in the former investigations using photons and neutrons was equivocal.Hoppeet al[35]demonstrated improved progression-free survival and overall survival in patients receiving RT dose ≥ 65 Gy,while other studies exhibited poorer survival outcomes as this dose limit was surpassed[36,37].That might be ascribed to increment of potentially life-threatening doserelated toxicities,like radiation necrosis of temporal lobe and blindness.However,the utilization of pencil beam scanning technique allowing for intensity modulated proton therapy (IMPT,used on our patients presented) may reduce overall toxicities,largely by sparing of adjoining normal tissues,and increase LC,by delivering higher dose to the target[38-39,41-42].In the setting of extended ipsilateral orbital invasion as reported in“Case 2”,moderate excess of maximum dose to the right optic nerve [65.30 Gy (RBE)]and right eyeball [70.11 Gy (RBE)] was deliberately permitted due to decreased integral dose of the critical structures by means of IMPT.Herein,the mean doses for the right optic nerve and eyeball were 60.06 Gy (RBE) and 52.36 Gy (RBE) respectively.At a follow-up period of 2 years,severe ocular toxicity was not observed.
Furthermore,unlike CIT,with confined irradiation field size,and aforementioned publications,mostly on the ground of obsolete passive scattering PBT,IMPT using active scanning technique facilitates the implementation of an elective neck irradiation simultaneously at uncertain nodal metastases.Even for manifest nodal disease as our patient in “Case 1”,PBT can be affiliated with an inferior demand of opioids and a reduced rate of gastrostomy tube dependence.In comparison of acute toxicities between PBT and IMRT for nasopharyngeal and sinonasal cancers with comprehensive head and neck irradiation,the mean doses to the oral cavity,esophagus,larynx and parotid glands was significantly lower when utilizing PBT,corresponding to a retrospective study of McDonaldet al[43].To estimate the potential benefit for PBT over IMRT in terms of dose reduction in organs at risk,normal tissue complication probability models may support treatment selection for head and neck cancer patients[39,42].

Figure12 Positron emission tomography with 2-deoxy-2--fluorine-18-fluoro-D-glucose/computed tomography exhibited remarkably increased uptake in the right periorbital sinonasal squamous cell carcinoma.
CONCLUSION
Both cases with locally advanced periorbital SNSCC treated with PBT alone demonstrate excellent results in view of tumor control and quality of life at a followup period of 5 years and 2 years.In general,the therapy regimes of SNM should be managed individually according to histology,tumor stage,prior treatments,personal risk factors,and patient preference.Both multimodality and non-surgical approaches are overdue to be reviewed profoundly in prospective randomized trials.Still,given the dosimetric advantages of PBT,especially in reducing the ocular and brain toxicities for unresectable gross disease,it is somehow unethical to withhold IMPT from the patients on account of random allocation of study design,limited availability of IMPT,lack in clinical experience,and insurance status.A model-based approach on normal tissue complication probability may relieve the selection of suitable patients with clinically significant benefit from PBT.

Figure13 Treatment plan of proton beam therapy with isodose distributions in all three planes and dose-volume-histogram.
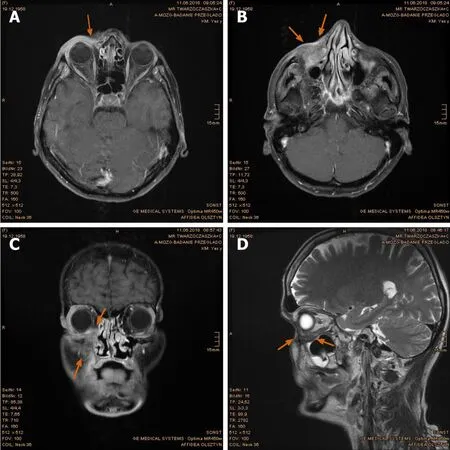
Figure14 Pronounced tumor reduction in the first follow-up magnetic resonance imaging scan.
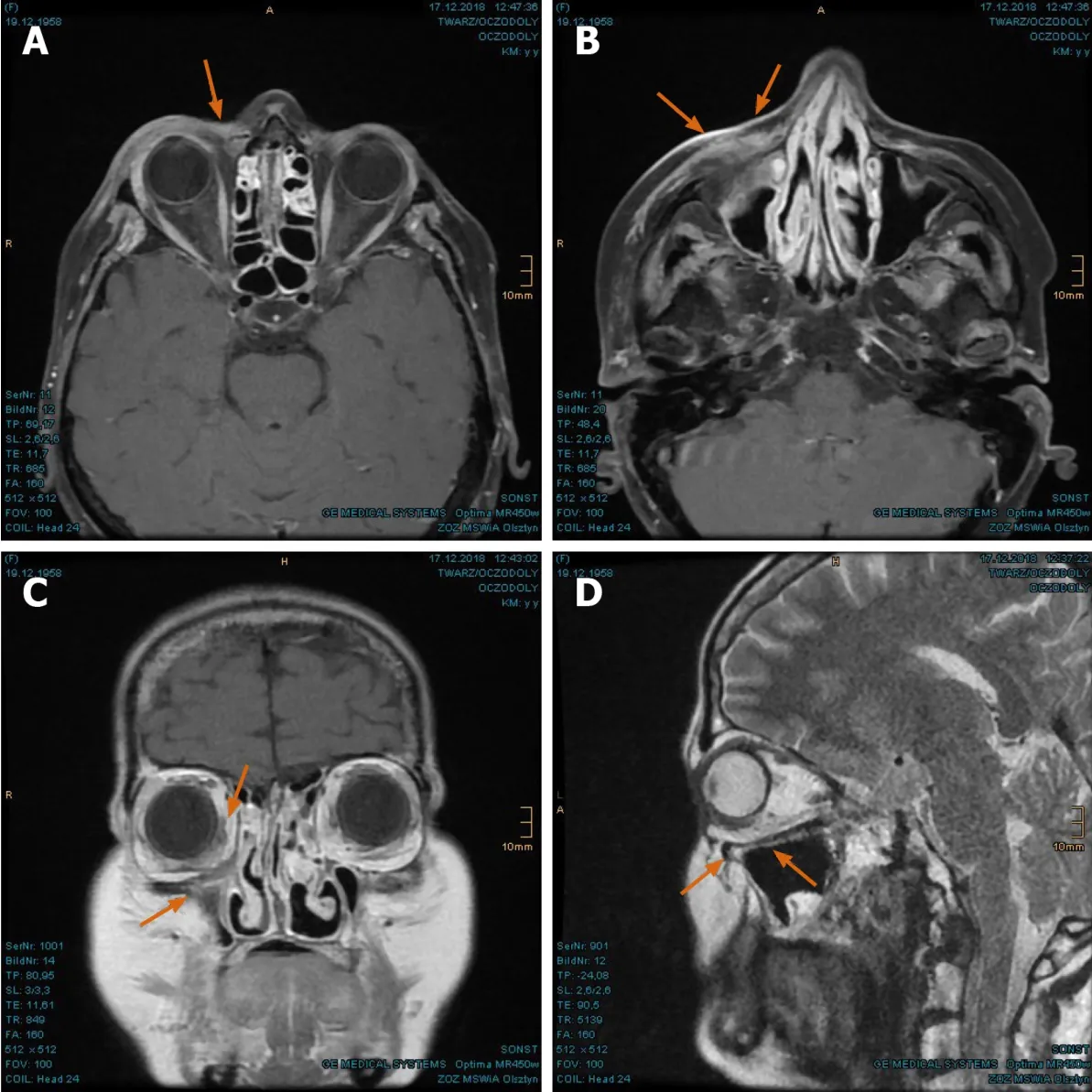
Figure15 Complete tumor remission verified in the magnetic resonance imaging at 8 mo after proton beam therapy.
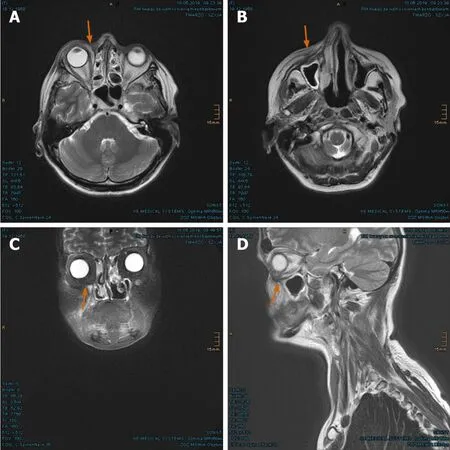
Figure16 Sustained full remission in the magnetic resonance imaging at 14 mo after proton beam therapy.

Figure17 “Case 2” patient’s current image at 2 years after proton beam therapy.
杂志排行

World Journal of Clinical Oncology的其它文章
- GOECP/SEOR clinical recommendations for lung cancer radiotherapy during the COVID-19 pandemic
- B-cell lymphoma-2 inhibition and resistance in acute myeloid leukemia
- Combination drug regimens for metastatic clear cell renal cell carcinoma
- Circular RNA and its potential as prostate cancer biomarkers
- Statins in risk-reduction and treatment of cancer
- Novel molecular targets in hepatocellular carcinoma