Androgen receptor in bladder cancer: A promising therapeutic target
2020-07-30AbhishekTripthiShilpGupt
Abhishek Tripthi , Shilp Gupt
a Section of Hematology Oncology,University of Oklahoma Stephenson Cancer Center,Oklahoma City,OK, USA
b Department of Hematology and Medical Oncology, Cleveland Clinic Taussig Cancer Institute,Cleveland, OH, USA
KEYWORDS Androgen receptor;Urothelial carcinoma;Bladder cancer;Targeted therapy;Enzalutamide;Cisplatin;Testosterone
Abstract There has been a significant progress in the treatment of metastatic urothelial carcinoma in the last few years with the advent of immunotherapy after a long gap of no drug approvals for over 4 decades.While immunotherapy with checkpoint inhibitors has revolutionized the treatment of urothelial carcinoma, unfortunately, only a minority of patients respond to immunotherapy.Treatment options for patients who do not respond and/or progress on immunotherapy are very limited and overall prognosis remains dismal in metastatic urothelial carcinoma. The first targeted therapy targeting the fibroblast growth factor receptor (FGFR)was recently approved for bladder cancer, but it is effective only in select patients harboring the FGFR2 and FGFR 3 mutations. Antibody drug conjugates like enfortumab vedotin have shown promising activity in clinical trials. Development of novel targeted therapies remains an area of investigation and an unmet need in bladder cancer.Exploitation of androgen receptor (AR) is a potential strategy for targeted drug development in bladder cancer. A significant proportion of urothelial carcinoma patients express AR irrespective of gender. AR signaling in urothelial carcinoma has been linked to progression through multiple mechanisms, including activation of human epidermal growth factor receptor-2(EGFR or HER-2)signaling and epithelial to mesenchymal transition (EMT). Furthermore, AR is enriched in the luminal papillary mRNA subtype of urothelial carcinoma and also mediates resistance to cisplatin-based chemotherapy.Preclinical evidence suggests that AR inhibition can successfully inhibit urothelial carcinoma growth as monotherapy and is synergistic with cisplatin-based chemotherapy. We review the preclinical and clinical evidence supporting the putative role of AR signaling in urothelial carcinoma pathogenesis, progression and its role as a novel therapeutic target and future directions.
1. Introduction
Globally, urothelial carcinoma (UC) accounts for approximately 450 000 new cancer cases and 165 000 deaths every year with a significantly higher incidence in males compared to females [1,2]. Majority of patients are diagnosed with non-muscle invasive bladder cancer(NMIBC)for which, transurethral resection of bladder tumor (TURBT)with intravesical therapy with BCG, or chemotherapy agents like valrubicin, mitomycin or gemcitabine form the cornerstone of therapy [3]. Patients with localized muscle invasive bladder cancer (MIBC) are treated with multimodality therapy with neoadjuvant chemotherapy (in cisplatin eligible patients) followed by radical cystectomy or bladder sparing approaches incorporating maximal TURBT and concurrent chemotherapy and radiation or partial cystectomy in selected cases [4-7]. However,despite initial curative intent treatment, around 50% of patients with muscle invasive disease experience disease recurrence and develop incurable metastatic UC(mUC)[4].
For patients with mUC, platinum-based combination chemotherapy continues to be the first line of therapy in eligible patients with gemcitabine plus cisplatin (GC) and conventional or dose-dense methotrexate,vinblastine,doxorubicin and cisplatin (MVAC) or gemcitabine and carboplatin being the most commonly utilized regimens[8,9].After a long void of over 4 decades, the past few years have witnessed significant progress inthe treatment of mUC withthe advent of immune checkpoint inhibitors(CPIs)resulting in the Food and Drug Administration(FDA)approval of five CPIs,namely programmed cell death ligand-1 (PD-L1) inhibitors (avelumab,atezolizumab, and durvalumab) and anti-PD-1 antibodies(nivolumab and pembrolizumab)for mUC treatment[10-15].While all the CPIs are approved for patients with platinumrefractory mUC, only atezolizumab and pembrolizumab are approved for use as first-line therapy in cisplatin-ineligible patients with mUC with high-PD-L1 expressing tumors or those who are“platinum-ineligible”[16].
While CPIs have significantly changed the treatment paradigm in mUC, their efficacy remains modest with responses seen in only around 20% of patients. Treatment options are very limited for mUC patients who do not respond or progress on CPIs. Promising activity has been observed with a novel antibody drug conjugate, enfortumab vedotin in mUC patients refractory to prior platinumbased chemotherapy and CPIs and has received accelerated FDA approval [17]. The fibroblast growth factor receptor(FGFR) inhibitor erdafitinib, was also recently approved by the FDA for mUC patients with susceptible FGFR3 or FGFR2 genetic alterations and disease progression after prior platinum-containing chemotherapy[18].While this marks a major advancement as the first targeted therapy to get approved in mUC,its use is limited to only around 10%mUC patients harboring the susceptible genetic alterations. The five-year survival in mUC remains dismal and exploring rational therapeutic targets in UC remains an unmet need.In this review,we will provide an overview of the role of AR in bladder cancer progression and the preclinical and clinical implications of targeting AR in urothelial cancer.
2. Structure and function of AR
The AR is a nuclear transcription factor and a member of the steroid hormone receptor family of genes and consists of a deoxyribonucleic acid (DNA) binding domain, ligand binding domain(LBD)and an N-terminal domain(NTD)[19].In the absence of its ligand, the AR is located primarily in the cytoplasm bound to heat shock proteins (HSPs). Upon binding to its ligands such as dihydrotestosterone (DHT), it translocates to the nucleus and regulates the transcription of its target genes known as androgen response elements(AREs). Its role in oncogenesis is most widely recognized in prostate cancer where agents targeting AR signaling such as gonadotrophin releasing hormone (GnRH) agonist/antagonists and AR inhibitors such as enzalutamide, and more recently apalutamide and darolutamide continue to be the cornerstone of therapy [20-22]. Emerging evidence suggests that besides prostate cancer, AR may play a role in other cancers, like triple-negative breast cancer and bladder cancer.
3. Physiologic functions of AR in bladder
The prostate,membranous urethra and urinary bladder are derived from the endoderm of urogenital sinus. Although not considered to be an androgen responsive organ, AR expression in normal urothelium, submucosa and smooth muscle and neurons has been described in primate and human bladder [23-28]. The role of AR in normal development of bladder remains incompletely understood. In preclinical models, androgen deficiency was associated with a significant decrease in total and smooth muscle bladder mass, decreased autonomic nerve function,decreased bladder capacity, and testosterone supplementation was able to attenuate these effects [29-32]. These studies indicate that AR signaling plays a significant role in normal embryonic development and function of the urinary bladder.
4. Role of AR in UC
4.1. AR and gender variation in UC
Although traditionally not thought to be an androgen driven malignancy,UC has a strong male preponderance[2].While exposure to chemical carcinogens through cigarette smoking and occupational exposure has been implicated as the reason for the gender disparity, men continue to be at three to four times increased risk of developing bladder cancer than women even when accounting for lifestyle and environmental factors. Women usually present with more advanced disease at diagnosis and have worse outcomes[33-36]. Differences in AR signaling might be one possible explanation for this gender predilection. In mice models,Miyamoto et al. [37] demonstrated that the oncogenic effects of the known carcinogen N-butyl-N-(4-hydroxybutyl)nitrosamine (BBN) were dependent on AR signaling. In this study, the incidence of UC was higher in AR wild type male mice treated with BBN compared to female mice (92%vs.42%, respectively) while none of theARknockout mice developed cancer and suppression of AR signaling with castration orARknock down was able to decrease tumor cell growth in mice who did develop tumors[37].However,in contrast to these preclinical findings, comparative analyses and case control studies have not shown any association between AR expression and gender [38-40].
4.2. AR and progression of UC
Several preclinical studies have demonstrated an association between AR and development of UC. Wu et al. [41]investigated whether targeting the AR has a therapeutic effect in bladder cancer by using small interference RNA(siRNA) strategy to knock downARexpression in experimental modelsin vitroandin vivo. This study demonstrated thatARknockdown in AR positive T24 and 253-J cell lines using siRNA resulted in a significant decrease in cell proliferation, migration compared to control which was accompanied by decrease in expression of cyclin-D1, Bcl and metastasis related matrix metallopeptidase-9 [41].Providing further mechanistic insights into the tumorigenic effects of AR signaling, studies by Zheng et al. [42] and MacLaine et al.[43]investigated the cross talk between AR signaling and EGFR and ERBB2 pathways which are known drivers of tumor cell growth in UC [42,43]. In AR positive bladder cancer cell lines (UMUC3 and TCC-SUP), treatment with DHT mediated AR transactivation and cell proliferation which was partially mediated through the EGFR pathway[42].DHT increased mRNA and protein expression of ERBB-2 and EGFR and their downstream target genes while treatment with an anti-androgen significantly attenuated this effect [42]. In UMUC3 cells, silencing of AR expression by transfection with a retrovirus vector pMSCV/U6-AR-short hairpin RNA (shRNA) was associated with decrease in basal levels of ERBB2 and EGFR expression and a decrease in ability of DHT to induce their expression[42].In cystectomy specimens, AR expression was strongly associated with EGFR and ERBB2 expression; AR positivity was significantly associated with tumor progression and EGFR,pEGFR,ERBB2 and pERK showed a trend towards progression. This study confirmed that AR signaling pathway, via regulation of the EGFR/ERBB2 pathways, can lead to the progression of bladder cancer,further providing the rationale of androgen deprivation potential therapeutic approach [42]. AR expression has also been linked to epithelial to mesenchymal transition(EMT)in UC and activation of AR has been associated with increase in markers of EMT such as vimentin and N-cadherin through increase in Wnt/β-catenin signaling[44]. Importantly, data from The Cancer Genome Atlas(TCGA) bladder cancer study demonstrated that while somatic alterations in theARgene are rare,high expression of genes involved in AR signaling was observed in the luminal papillary mRNA subtype [45,46]. Specifically, luminal tumors showed decreased activity in the nodes of epidermis development and extracellular matrix, and increased activity in the node of steroid metabolism which was associated with higher expression of AR.This finding suggests that AR could be a rational therapeutic target in luminal subtypes of bladder cancer.
In addition to its role in UC progression,there is evidence that AR signaling might be important as a putative resistance mechanism to cisplatin,a commonly used chemotherapeutic agent in mUC. Kashiwagi et al. [47] demonstrated that cell lines expressing full length wild type AR(647V-AR and 5637-AR with exogenous AR, UMUC3 with endogenous AR) were significantly more resistant to the cytotoxic effects of cisplatin compared to AR negative cell lines.This difference in cisplatin sensitivity was attenuated in presence of an androgen depleted culture medium supplemented with charcoal-stripped fetal bovine serum (CS-FBS). Addition of synthetic androgen R1881 to AR positive cell lines significantly reduced the cytotoxic effect of cisplatin which was accompanied by increase in NF-κB, a known mediator of cisplatin resistance. Conversely, in cisplatin resistant cell lines,treatment with AR inhibitor hydroxyflutamide restored cisplatin sensitivity. Furthermore, among patients with MIBC,there was a trend toward higher AR expression among patients refractory to neoadjuvant cisplatin-based chemotherapy compared to those achieving a pathologic response[47]. Taken together, these studies highlight the role of AR signaling not only as a potential driver of urothelial carcinogenesis and progression,but also a potential mechanism of resistance to cisplatin,thus providing rationale to target AR in combination with cisplatin in UC, to enhance efficacy of cisplatin.
4.3. AR expression in UC and correlation with clinicopathologic features
Prevalence of AR expression by immunohistochemistry(IHC)has been reported in tumor tissue in 11%-55% of patients with UC. While some studies have reported increase in AR expression in tumor tissue compared to normal urothelial tissue [48], others have reported down regulation of AR expression in tumor tissue [26-28]. Findings of recent studies examining AR expression in UC are summarized in Table 1. In a meta-analysis of nine studies examining AR protein expression,AR expression was found to be similar in tumor tissue compared to normal urothelium (hazard ratio[HR]: 1.13;p=0.33) and muscle-invasive tumors compared to non-muscle invasive tumors (HR: 0.66;p=0.35) [49].Interestingly,AR expression was lower in high-grade tumors(compared to low grade tumors;HR:0.57;p<0.001)tumors.In contrast, Elzamy et al. [50] reported that AR expression was seen in 35%of patients with localized UC and associated with higher tumor grade and muscle invasion.
Studies investigating the prognostic significance of AR expression in UC have reported somewhat discordant results. Nam et al. [51] reported that AR expression was associated with decreased risk of recurrence in patients with NMIBC. In contrast, other study did not find a significant association between AR expression and outcomes [50]. Recently, Sikic et al. [53] reported their analysis of correlation between AR mRNA expression in their institutional cohort of UC patients (41 patients) and those included in the TCGA dataset (323 patients). While there was no correlation between AR expression and gender (p=0.23), females showed a significantly worse disease-free survival (p=0.03) and overall survival(p=0.02)when expressing AR mRNA above median level in contrast with men where this was not observed. They concluded that AR mRNA expression was an independent prognostic marker for disease-free survival in women(p=0.007). In addition, their analysis showed that AR mRNA expression was significantly higher in NMIBC than in muscle-invasive disease [51]. Yasui et al. [54] studied the correlation between NMIBC recurrence and tumor AR expression in Japanese patients. In this study specimens from 53 patients with NMIBC were retrospectively analyzed for AR expression and correlated with recurrence-free survival. Real-time quantitative PCR was used to quantify AR mRNA expression. While there was no significant difference in recurrence-free survival between the high AR mRNA-expressing group and the low AR group,multivariate analysis showed female gender (HR: 7.360,p=0.009),tumor size ≥3 cm(HR:23.697,p<0.001)and low AR mRNA expression (HR: 0.202,p=0.028) to be independent predictors of shorter recurrence-free survival [52].
It is possible that these discrepant results could be due to differences in the assays used to assess AR expression. In addition, it is possible that AR expression might change during the progression of bladder cancer[50] and AR protein expression or mRNA expression by itself may not accurately reflect AR signaling. Supporting this hypothesis, Bergerot et al. [55] utilized IHC to assess AR expression and quantitative polymerase chain reaction (qPCR) to develop an AR activity score reflecting expression of AR responsive genes. Among the 37 patients with MIBC included in this study, AR expression by IHC was noted in 54% of patients in tumor tissue with but did not correlate with AR activity score[50]. Given variable results from the trials cited above,systematic clinical studies are needed to investigate mRNA and protein expression levels simultaneously in UC to determine prognostic and predictive significant of AR in various stages of UC.
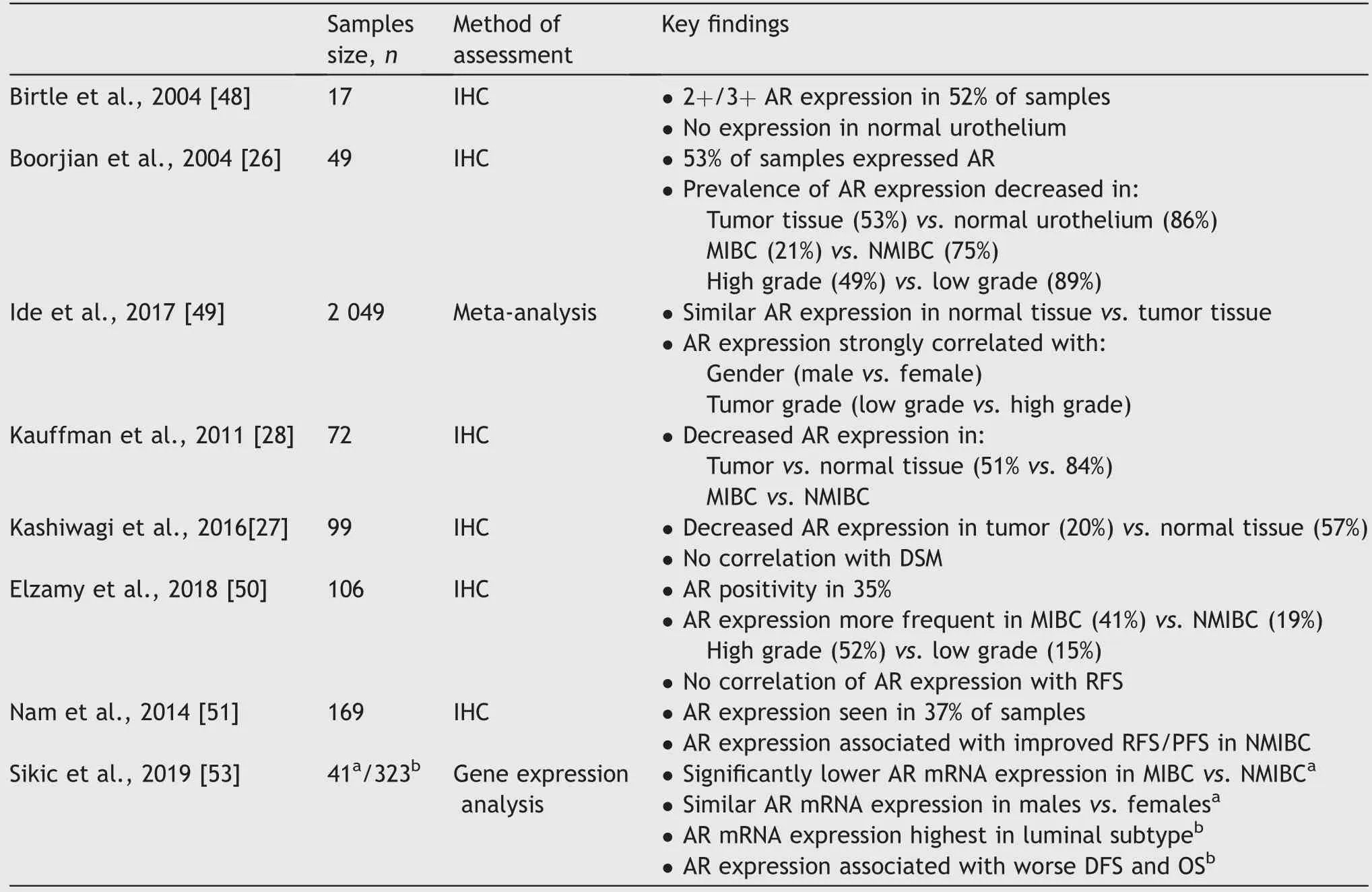
Table 1 Summary of prior studies investigating the prevalence and significance of AR expression in urothelial carcinoma.
5. Targeting AR in UC
The prevalence of AR expression in UC, its putative role in UC progression as well as availability of multiple novel AR directed therapies make it an attractive therapeutic target in the clinic.Several preclinical studies have evaluated the anti-tumor efficacy of androgen deprivation therapy or AR inhibitors[56,57].In SVHUC-AR cells exposed to carcinogen methylcholanthrene (MCA), enzalutamide, hydroxyflutamide and bicalutamide inhibited AR signaling mediated transcriptional activity and cell growthin vitroalong with downregulation of several oncogenes such as c-myc,cyclin D1, and cyclin E [58]. Similarly, in UMUC3 cells treatment with these AR antagonists decreased androgeninduced expression of AR, matrix metalloproteinase-2,and interleukin-6. However, in UMUC3 xenograft-bearing mice, only enzalutamide demonstrated a statistically significant suppression of tumor growth compared to control[59]. Preclinical evidence shows that AR mediates resistance to cisplatin-based chemotherapy and EMT. Tyagi et al. [60] further investigated the antitumor efficacy of combined treatment with enzalutamide and cisplatin in bladder cancer cell lines.Concurrent treatment with these agents synergistically inhibited tumor cell growth which was associated with increase in pro-apoptotic signaling and decrease in mesenchymal markers [56]. Similar results were reported by Huang et al. [61] in a study investigating the AR degrader ASC-J9 in miBCa cells. The authors demonstrated that combined treatment with ASC-J9 and cisplatin was associated with increase in the expression of the pro-apoptosisBAXgene and cell cycle inhibitorp21gene along with decrease in anti-apoptotic geneBCL-2and was able to suppress tumor growth better than cisplatin alone [57].
Despite preclinical data providing rationale for targeting AR alone and with cisplatin in UC, there is paucity of clinical data regarding efficacy of AR inhibitors in UC. A phase 2 trial of enzalutamide in bladder cancer chemoprevention in NMIBC was attempted but terminated early due to low accrual (NCT02605863). Our group conducted a phase 1/1b trial investigating the safety and efficacy of enzalutamide in combination with cisplatin and gemcitabine in patients with mUC (NCT02300610) [62].Treatment naı¨ve patients with advanced UC were enrolled using a 3+3 dose escalation design to evaluate two dose levels of enzalutamide (80 mg daily and 160 mg daily) in combination with six cycles of standard doses of cisplatin and gemcitabine. A total of 10 patients were enrolled which included six enrolled in the dose escalation phase and four treated in the dose expansion part of the study.No dose limiting toxicities were noted and the maximum tolerated dose of enzalutamide was 160 mg daily. The combination demonstrated encouraging efficacy with complete response in one female patient with strongly positive AR expression, and partial response and stable disease in four and two patients respectively. Despite the limitation of being a small study, we demonstrated for the first time that enzalutamide can be safely combined with cisplatin and gemcitabine in mUC and the combination has promising efficacy, which needs to be tested in larger trials.
6. Conclusions and future directions
While significant progress has been made in therapy advances in mUC with advent of CPIs,only a minority of patients benefit and patient outcomes remain poor. UC is a heterogeneous disease and there is a scope to develop effective targeted therapies alone, or in combination with other therapies like chemotherapy, targeted therapies and immunotherapy. AR signaling plays a significant role in UC oncogenesis, progression and mediating resistance to cisplatin-based chemotherapy, providing a rationale to target AR in mUC. Use of AR inhibitors is a rational therapeutic strategy to prevent AR mediated UC growth and potentially prevent resistance to cisplatin-based chemotherapy.We have demonstrated the safety of this combination approach of enzalutamide, cisplatin and gemcitabine;this needs to be further tested in larger randomized trials to investigate the efficacy of this combination. Emerging evidence also suggests that AR signaling could exert an immunosuppressive effect in the tumor microenvironment by decreasing interferon response and increase in immunosuppressive regulatory T cells. Furthermore, enzalutamide has been shown to have immunomodulatory potential, first described in prostate cancer mouse models,rendering them more sensitive to immune-mediated therapies[63].Ongoing studies in metastatic prostate cancer are combining enzalutamide and pembrolizumab(NCT02312557,NCT02861573).This approach of targeting AR with novel AR inhibitors like enzalutamide and CPIs can result in potential synergy. In conclusion, targeting AR in UC is a rational and promising approach based on available preclinical and clinical data and future trials with AR directed therapies alone, or in combination with other therapies are urgently needed to improve outcomes in mUC.
Author contributions
Study concept and design: Shilpa Gupta.
Data acquisition: Abhishek Tripathi.
Data analysis: Abhishek Tripathi, Shilpa Gupta.
Drafting of manuscript: Abhishek Tripathi.
Critical revision of the manuscript: Shilpa Gupta.
Conflicts of interest
Dr. Abhishek Tripathi has received honorarium for advisory role from Foundation Medicine, and Pfizer, and has received research funding to institution from EMD Serono,Bayer,Clovis Oncology,Aravive Inc.,WindMIL therapeutics,and Corvus Pharmaceuticals.
Shilpa Gupta has received research funding to institution from BMS, Astellas, Seattle Genetics.
杂志排行

Asian Journal of Urology的其它文章
- Androgen receptor: Functional roles and facets of regulation in urology
- Mesenteric metastases from mature teratoma of the testis: A case report
- Intractable hematuria due to giant prostatic hyperplasia effectively treated with prostatic artery embolization
- Sheathless and fluoroscopy-free retrograde intrarenal surgery: An attractive way of renal stone management in high-volume stone centers
- Efficacy and safety of degarelix in patients with prostate cancer:Results from a phase III study in China
- Survival after radical cystectomy for bladder cancer: Multicenter comparison between minimally invasive and open approaches