Thoracic surgery by minimally invasion robotassisted in children: “experience and current status”
2020-07-30MarioNavarreteArellano
Mario Navarrete-Arellano
Pediatric Surgery, Hospital Central Militar, SEDENA, Mexico City 11200, Mexico.
Abstract
Keywords: Robotic surgery, thoracic surgery, thoracic robotic surgery, thoracoscopy, congenital malformations, children
INTRODUCTION
Minimally invasive techniques are applicable in more than 60% of abdominal and thoracic operations in children, according to evidence-based data and ethical principles can be used properly[1].The first publication on thoracoscopy in children dates from 1971 in Russia and, fundamentally its application at that time was diagnosed in thoracic diseases and neoplasms[2].From that date to the present, thoracoscopic surgery in children has been applied in a wide range of thoracic pathologies, with diagnostic and therapeutic procedures.
The global experience in thoracoscopic surgery in children is more than 30 years compared to robotassisted thoracic surgery (RATS), and, although the learning curve for thoracoscopy is longer compared to RATS, there are centers in the world where this curve has been overcome.The minimally invasive surgical (MIS) approach offers obvious advantages over the open technique to solve various thoracic pathologies[3].In 1981, Rodgers reported 80 thoracoscopic procedures in children, which were performed without mortality and with minimal morbidity, and the main technique was lung biopsy[4].
An important aspect in pediatric age is to prevent or avoid sequelae of surgery.Makitaet al.[5]conducted a comparative study to identify risk factors for thoracic and spinal deformities (scoliosis, pectus excavatum, chest asymmetry, and pectus carinatum) after lung resection during childhood, in patients undergoing thoracoscopic surgery versus thoracotomy.Their results are as follows: nine deformities (n= 49) were observed during follow-up in patients with thoracoscopy (18.3%), while patients with thoracotomy reported 19 deformities (n= 25) (76%), with aPvalue of 0.0000022.The authors concluded that minimally invasive thoracic surgery (MITS) reduced the risk of thoracic and spinal deformities after lung resection in children.
The most commonly performed technique in children with thoracoscopic surgery is lobectomy, but the learning curve is prolonged.An analysis of the learning curve in pediatric thoracoscopic lobectomy for congenital pulmonary malformations required a minimum of 50 cases of experience to obtain stable results with video-assisted thoracic surgery in pulmonary resections[6].This factor is one of the key obstacles for the thoracoscopic technique to be applied more widely in the world in the pediatric population.
With the learning curve overcome, meticulous thoracoscopic lobectomy is feasible in children, and it is effective in avoiding common postoperative (PO) complications, accelerating the recovery, and shortening the hospitalization time[7].
Clermidiet al.[8]published a study evaluating the feasibility of a fast-track protocol in thoracoscopic lung resection for congenital pulmonary airway malformations (CPAM) in children in 2017.Through the three periods, median PO hospital stay decreased (four, three, and two days, successively;P= 0.02).In the third period, four patients underwent day-case surgery.The authors concluded that the fast-track protocol for children undergoing uncomplicated thoracic surgery for CPAM seems feasible without extra morbidity, and selected patients undergoing thoracoscopic resection may benefit from the absence of pleural tube and can be operated on in day-case surgery.
In the adult population, Melfiet al.[9]published the first report on robotic surgery for thoracic diseases, with encouraging results in their preliminary experience.They believed that robotic procedures are technically feasible.Theirs was the first robotic lobectomy in Europe (February 2001, and published in 2002).
In the United States, the first pulmonary lobectomy performed with robotic assistance was reported in July 2003, in a 48-year-old woman with lung cancer[10].
The first publication on pulmonary lobectomy with robotic assistance, including pediatric cases, is from Parket al.[11], in 2006.They concluded that RATS lobectomy is feasible and safe, and the usefulness and advantages of robotic assistance for lobectomy require further refinement and study of the technique.
Toker[12]and his group started with a thoracic robotics program after an established experience of videoassisted thoracic surgery (VATS).The idea for a thoracic robotic program was based on the anatomical difficulties of some thoracoscopic lung resections and the superior capabilities of the robotic articulated instruments.
The main advantages of using a robotic device are: (1) the precision of the instrument and improved dexterity due to the use of “wristed” instruments; (2) three-dimensional imaging, with improved ability to locate blood vessels, nerves, and tissues; and (3) the surgeon's console, which reduces fatigue and allows for tremor-free manipulation[13].
The improvements with robotic assistance offer technical capabilities beyond the existing threshold limits of human performance for surgery within restricted work spaces in children; the camera is controlled by the primary surgeon; and articulated instruments allow dissection and precise anastomosis[14].The above are advantages for the surgeon, which benefit the patient.
RATS is gaining more acceptance for the adult population and recently large series have been reported on lobectomy[15,16]and excision of the mediastinal cyst[17].
The first robotic procedure in children was fundoplication, and was carried out by Meiningeret al.[18]in July 2000 and reported in 2001.
The safety of robotic-assisted surgery in children is reported to be similar to open procedures, and the outcomes are at least equivalent to standard laparoscopy[19].
Very few cases of RATS have been reported in children.The first publications of RATS in children were in the area of cardiovascular surgery[20,21].
Ballouheyet al.[22], in 2015, published on 11 patients treated with RATS at two pediatric surgery centers over a period of six years.Their conclusions were RATS for newborns and infants is still very challenging; these patients are not good candidates for this approach; and the most appropriate procedures are the removal of mediastinal cysts in children weighing more than 20 kg.
The objective of this article is to inform about our experience in MITS assisted by robot in children.In addition, a current analysis is carried out on this topic.
METHODS
Observational, prospective, and longitudinal studies were performed for pediatric patients with thoracic pathologic treated with RATS, from March 2015 to April 2019.The diagnosis was made with laboratory studies, X-rays, ultrasound, CT scan image, angiographic study, and histopathology, according to the patient.
The surgeries were performed by MITS assisted by robot.We used the “da Vinci surgical system Version Si” (Intuitive Surgical, Inc., Sunnyvale, CA.USA).
We use four or five trocars (three of four robotics and one laparoscopic).To collapse the hemithorax lung to operate, in patients younger than six years, we used CO2at 6 mmHg of pressure and flow of 1-4 liters per minute, while, in patients older than six years, selective intubation of the contralateral bronchus was used.
Registered variables included demographic data, diagnosis, surgical technique, total time, time of console surgery, bleeding, hemotransfusions, conversions, complications, PO stay, and follow-up.The data were entered into a spreadsheet in Microsoft Office Excel 2013.
Seven cases are part of the statistics of our published series of the first three years of robotic surgery[23].
Measures of central tendency were used.In relation to ethical considerations of the study, being of an observational nature, it was not necessary to obtain the informed consent for the patients to enter the study.The Research Ethics Committee of the Hospital evaluated and approved the study.To perform the medical and surgical procedures, we obtained the informed consent in writing from the parents or guardians.
We carried out a detailed non-systematic review of previous publications in PubMed on thoracic pathology treated with robotic surgery in the pediatric population, with the following four search strategies (at: https://www.ncbi.nlm.nih.gov/pubmed/): (1) robot-assisted thoracoscopic surgery + thoracic robotic surgery + children; (2) robot-assisted thoracoscopic surgery + children; (3) thoracoscopic robotic surgery + children; and (4) robotic surgery thoracic + children.
RESULTS
We treated 11 patients with thoracic pathology, six male and five female.The average age was 5.7 years (range 6 months to 15 years), the average weight was 21.34 kg (range: 5.93-60 kg), and the average height was 107 cm (range: 66-176 cm).The diagnoses were three congenital cystic adenomatoid malformation (CCAM) and an intralobar sequestration; three right diaphragmatic paralysis and a diaphragmatic eventration; and one case each of mediastinal teratoma, Ewing's tumor of the fourth left rib, and pulmonary tuberculosis.The surgeries performed were: four lobectomies (36.36%), four diaphragmatic plications (36.36%), two tumor resections (18.2%), and one pleural and lung biopsies (9.1%).
The following average values were found: console surgery time, 166.45 min (range: 25-314 min); bleeding, 42.27 mL (range: 0-150 mL); and PO stay, 3.6 days (range: 1-12 days).Conversions and PO complications were reported in one patient, and there were no intraoperative (IO) complications and mortality.Hemotransfusions were reported in one patient: a 10-month-old girl, weighing 5.93 kg and 66 cm tall, who entered the operating room with low hemoglobin, the diagnosis of CCAM, and underwent lower right lobectomy.She required 314 min of console surgery time, presented 40 mL of bleeding, and was hemotransfused in the immediate PO period.Her PO stay was three days.This is our smallest patient by weight and height.
The patient with Ewing's tumor, from the left hemithorax, was a seven-year-old boy, weighing 21 kg and was 102 cm tall.The patient initially underwent an open incisional biopsy, through a 5-cm incision over the tumor area, obtaining the histopathological diagnosis of Ewing's tumor of the anterior arch of the fourth left rib, with pulmonary invasion.After the favorable evolution with the cancer medical treatment and that the tumor could be resectable, a second surgery was planned for block resection, as follows: (1) RATS performed a non-anatomical segmentectomy, using staplers, resection with a healthy pleura flap, and tumor with 4 cm of the fourth left rib (using a Gigli saw); (2) before dedocking, an open resection of the overlying soft tissues was performed, including the 5-cm-long scar, and then the closure of the chest wall; and (3) using RATS, a mesh was applied to stabilize the chest wall, concluding surgery.The surgical time of the console was 240 min and there was 60 mL of bleeding.The pleural tube was left, which was removed on the second day of PO.
The conversion was a lobectomy in a 10-month-old boy weighing 7.8 kg, with a diagnosis of right basal intralobar pulmonary sequestration due to technical difficulties.The PO complication was the prolonged drainage of serous fluid, in an eight-month-old girl weighing 8 kg, who underwent a diaphragmatic plication due to the diagnosis of diaphragmatic paralysis.The pleural drainage was removed on the eleventh day and was discharged daily; this complication is of grade I, according to the classification of Clavienet al.[24].The average follow-up was 24.7 months, ranging from 9 to 51 months.
We performed a detailed non-systematic review of previous publications in PubMed on the thoracic pathology treated with robotic surgery in the pediatric population.We obtained 4, 8, 30, and 50 publications, respectively, using the four search strategies, but only 15 publications were about our topic.Currently, the number of children with non-cardiovascular thoracic pathology treated with robotic surgery has barely reached 100 cases.
DISCUSSION
We present a series of 11 RATS.These data support that some robotic procedures are surgically feasible.Our study and others confirm the technical advantages of thoracic robotic surgery, such as precise dissection and suturing in very small spaces[20,22], in addition to its general advantages, such as stereoscopic and magnified vision, in 3D, scale movements, tremor filtration, and the surgeon's console for operating while sitting and with total ergonomics.In addition, the articulated instruments are superior to the rigid thoracoscopic instruments in the thoracic cavity, which itself is quite rigid[22].
During the same period of this study, we performed a total of 254 robotic procedures in pediatric patients, with eight conversions to open surgery.RATS corresponds to 4.3% of the total procedures in our experience.
The first publications of RATS in children were about cardiovascular techniques, such as patent ductus arteriosus (PDA) closure and vascular ring division[20,25].In the 2000 study by Le Bretet al.[20], 56 children underwent a surgical closure of a PDA, 28 patients with thoracoscopic technique and 28 with a robotassisted approach.They used the ZEUS robot surgical system (Computer Motion, Inc., Goleta, CA.USA), concluding that the robotically assisted closure of a PDA is comparable with closure by means of the thoracoscopic technique.However, robot-assisted approach required a longer operative time because of the increment in complexity.Previously, starting in 1991, these authors had performed 630 procedures of thoracoscopic closure of the PDA, and their first 28 surgeries with a robotic approach.Based on the above, robotic assistance offers advantages and with few procedures the results are similar to the thoracoscopic technique.
Currently, very few cases of RATS have been published.However, many studies have reported that robotassisted surgery is safe and feasible for pediatric patients.
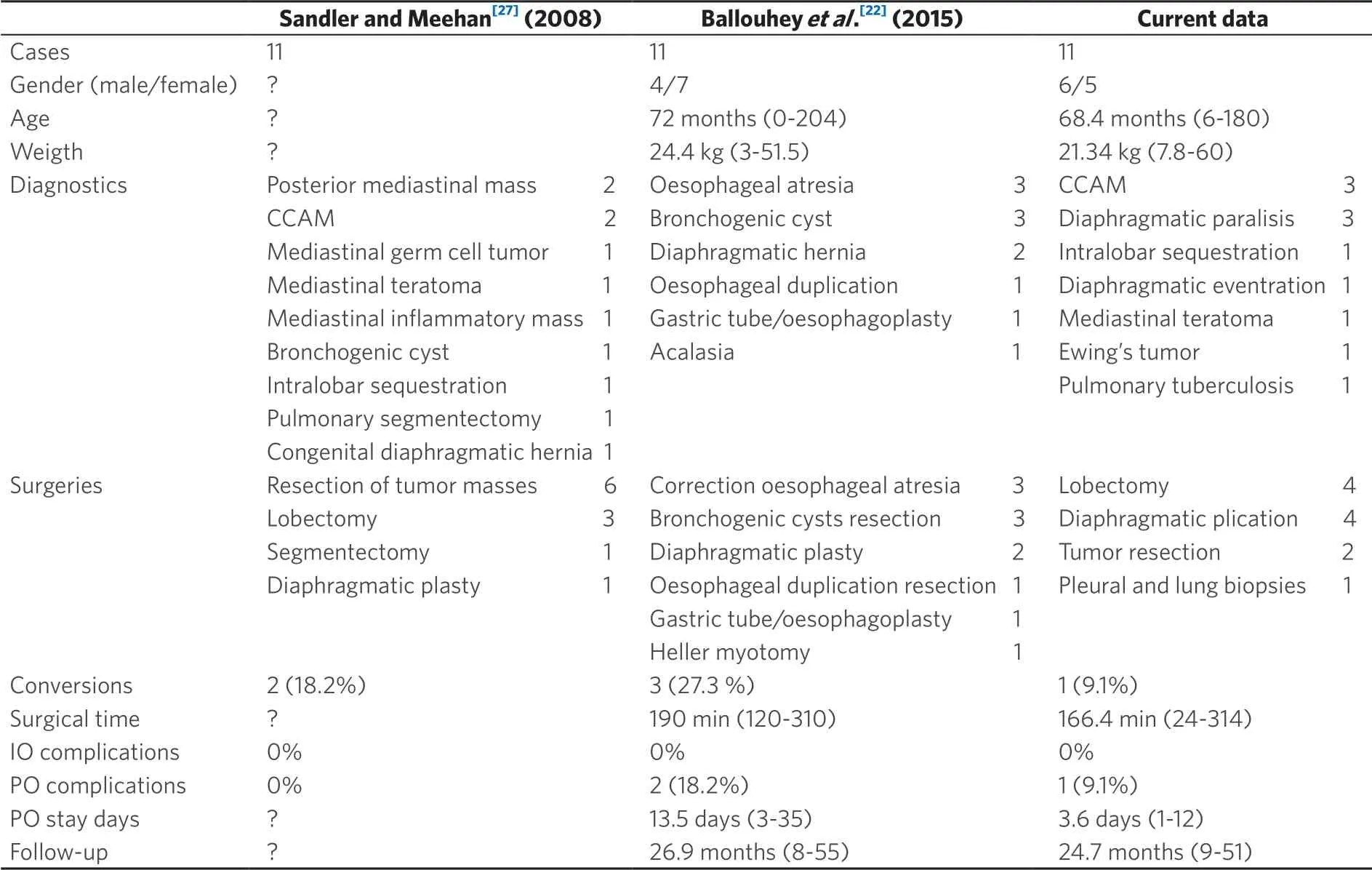
Table 1.Comparative series of cases of thoracic robotic surgery in children
RATS has previously been described as part of a series of general pediatric surgeries or a series of various thoracic pathologies[22,23,26,27], a series of pediatric cases of specific procedures such as thymectomy for myasthenia gravis[28,29], tracheopexy for treatment of severe tracheomalacia[30], or as pediatric case reports on esophageal leiomyoma and bronchogenic cyst[31-33].
We compared the results of two published series with ours[22,27].The three series are comparable, due to the diversity of thoracic pathologies and procedures and the number of cases of RATS in children.In our series, there was less conversion, less surgical time, less PO complications, and fewer days of PO stay.Conversion was more frequent in patients with lower weight, especially in newborns [Table 1].Most conversions in RATS are in children weighing less than 5 kg, and the extreme limit is 2.5 kg[22].
Patients between 3 and 5 kg with RATS are a great challenge and require experienced and capable surgeons.The fundamental technical limitation and disadvantage of RATS is in newborn patients and patients weighing less than 3 kg.
The dimensions of the robotic instruments (8 mm) require a minimum critical space to be manipulated, i.e., 5 mm.Their limitations are that they require more interior space in the cavity and have no energy.In the future, it will be necessary to implement a greater miniaturization of technology, preserving the functionality to treat children with lower weight.
The docking charts for robotic surgery suggested for surgical techniques in adults are not applicable for children.Therefore, sometimes, 3 cm of separation was required between each trocar when surgery was performed on infants, due to limited space in such small patients[23].
Cundyet al.[34]conducted a systematic search in the literature of reported cases of robotic surgery in children over a period of 11 years.They included 137 articles, with 2393 procedures in 1840 patients, and thoracic procedures accounted for 3.2% (77 surgeries and 12 different techniques).The conversion rate was 10% in RATS.The results show that the five most frequent RATS procedures are: lobectomy[18], thymectomy[14], benign mass excision[9], diaphragmatic plasties[8], and resection of malignant tumors[5].The other areas and procedures of robotic surgery that were part of this research were urological procedures (1434, 59.9%) and gastrointestinal procedures (882, 36.9%).Our small series of RATS cases coincides with the aforementioned data, in terms of thoracic pathology, surgical techniques, and conversion rate [Table 1].
Lobectomy is the most reported RATS, thus it is important discuss the surgical technique in children: (1) it is essential to have an excellent pediatric anesthesiologist, for the management of ventilation with a single lung, either by selective intubation (school-aged children and teenagers), or using 6 mmHg of pressure with CO2for pulmonary collapse; (2) for school-aged patients and adolescents, there should by an assistant surgeon who has the skills to handle and apply staplers, as it is the safest way to manage vascular structures, bronchial tubes, and interlobar lung tissue.
In most of our RATS procedures, from the open technique we jump to robotic surgery, due to the low frequency of presentation of these pathologies, and the thoracoscopic technique implies a longer learning curve.This also happened to Meehan and Sandler[27].Robotic assistance is ideal for complex hepatobiliary cases and thoracic surgery, particularly for solid mass resection[35,36].
Despite performing several different types of operations in the first months, we felt comfortable with the robot after approximately 15 cases.This experience is consistent with our colleagues in adult surgery[37].Reports suggest anywhere between 25 and 50 cases are required to learn a single new laparoscopic procedure[38].We believe that robotic surgery has a clear advantage over thoracoscopic surgery simply because the fulcrum effect is no longer a problem.
Robotic thoracoscopic surgery has been successfully applied to the removal of mediastinal masses or cysts, such as bronchogenic cyst, teratoma, esophageal duplication, esophageal leiomyoma, neurogenic tumor, and thymic pathology[39].
Radical thymectomy is the comprehensive treatment of myasthenia gravis.The feasibility and effectiveness of robotic thymectomy is evident in this cohort study[40].
In addition, performing the “early thymectomy” (performed within a year of diagnosis) resulted in higher remission rates compared to “late thymectomy”[41], including minimizing the adverse effects of immunosuppression in pediatric patients[42].
Other intra-thoracic pathologies that have been treated with RATS are tracheomalacia and resection of a right paraspinal mass[43,44].
Congenital diaphragm abnormalities, including eventration and Morgagni and Bochdalek diaphragmatic hernias, have been successfully repaired through the use of conventional MIS.However, some reports have shown a high recurrence rate for some defects, potentially due to the difficulty associated with rigid instruments.Robotic surgery is the alternative to close diaphragmatic hernias more efficiently[45].
Acquired anomalies, such as diaphragmatic paralysis, can also be resolved with RATS.The experience of other authors and ours confirms that robotic surgery is safe and effective for repairing diaphragm abnormalities in children[23,45].Slater and Meehan[45]preferred the thoracic approach for repairing Bochdalek congenital diaphragmatic hernia, but sometimes smaller babies, less than 2.5 kg, can improve with the abdominal approach, since articulated instruments require considerable length to maneuver.The authors operated by abdominal approach on a case of Morgagni congenital diaphragmatic hernia and another case of Bochdalek congenital diaphragmatic hernia.
Regardless of the fact that thoracoscopic surgery in newborns is demanding for the surgeon and the patient, surgeons with large experience in MIS, with advanced skills, and with learning curve overcome, can perform complex procedures with efficacy and safety, such as thoracoscopic repair of esophageal atresia with tracheoesophageal fistula[46], and even repair of long-gap esophageal atresia[47].
In our series of 11 RATS cases, five patients weighed between 5.93 and 10.6 kg, three had diaphragmatic plication, and two lobectomy.The case of conversion to thoracotomy was a 7.8 kg patient with pulmonary sequestration, being our first robotic lobectomy.The reason for the conversion was the difficulty in maneuvering the articulated instruments.Then, in the second lobectomy, the smallest patient in our series of cases (5.93 kg), we made a totally cephalic (longitudinal) docking and placed the trocars only penetrating the thickness of the thoracic wall, with which we obtained a better space inside the thoracic cavity and we could perform a comfortable and safe lobectomy [Figure 1].The three cases of diaphragmatic plication were performed without problems with RATS.
The application of MIS for the treatment of malignant solid tumors in children is very controversial.From 1966 to February 2011, the authors were unable to identify randomized controlled trials or controlled clinical trials that evaluated MIS in the treatment of intra-thoracic or intra-abdominal solid neoplasms in children; therefore, no definitive conclusions could be drawn about the results of MIS in these patients.Based on the available evidence at that time, the authors could not give recommendations for the use of MIS in the treatment of solid malignancies in children[48].
Following the publication of the above conclusions, several case series of intra-thoracic solid tumors treated with VATS in children have been published.
The efficacy and safety of resection of mediastinal tumors in children were compared, using thoracotomy in 10 cases and VATS in 21 cases.The approach was indicated as non-randomized, and the analysis of the results was retrospective.The VATS group required significantly fewer blood transfusions, shorter duration of thoracic drainage, and shorter hospital stay, thus suggesting VATS is less invasive[49].
Another series was of 17 children with thoracic neurogenic tumors, with an average weight of 11.9 kg (range: 9.3-27.4 kg).The series consisted of ten children with neuroblastoma, four with ganglioneuroma, and three with ganglioneuroblastoma.Complete thoracoscopic resection was performed in all cases.There were no deaths and no recurrence was observed during the follow-up period of 8.9-28.6 months.VATS resection of mediastinal neurogenic tumors in children offers good results.The main advantages of this approach are it avoids thoracotomy complications and improves surgical accuracy by having a better view of the anatomy[50].
Irtanet al.[51]published a series of 39 patients undergoing MIS due to neuroblastic tumors, using thoracoscopy in 20 patients, retroperitoneoscopy in 1 patient, and laparoscopy in 18 patients.The average diameter was 35 mm for thoracic tumors (range 7-85 mm).Resection was incomplete in six thoracic tumors and one adrenal tumor.Conversion was necessary in three cases of thoracic tumors.PO complications occurred in five patients.The overall survival rate was 98%.The authors concluded that, in carefully selected cases, MIS allows the safe and efficient resection of neuroblastic tumors in children.
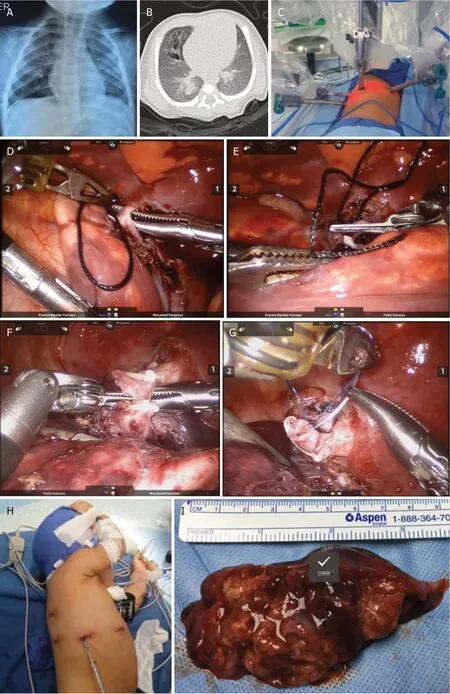
Figure 1.Robotics lobectomy technique in an infant patient.Female patient, 10 months old and 5.93 kg in weight.A, B: chest X-ray and CT scan image showing the right lower lobe affected by CCAM; C: location of the two 8-mm robot instrument trocars, an 8.5-mm trocar for camera lens, and an auxiliary 5-mm trocar in the right hemithorax and cephalic docking; D, E: IO images, dissection, ligation, and cutting of the pulmonary vein of the affected lobe; F, G: IO images, management of the lobular bronchus with hemoclip and suture; H: the complete lobectomy and pleural tube emerge through the wound to the trocar of the camera lens; I: the surgical piece was removed through the trocar wound of the camera lens.CCAM: congenital cystic adenomatoid malformation; IO: Intraoperative
Publications on the treatment of malignant tumors in children by RATS are only from isolated cases.Meehan and Sandler[36]reported a case of mediastinal germ cell tumor, a ganglioneuroma, a ganglioneuroblastoma, a teratoma, and an inflammatory mass of unclear etiology.They concluded the robotic surgery is safe and effective for resecting solid mediastinal tumors.The application of RATS in malignant solid tumors in children in selected cases is an option, but oncological surgical principles should be applied.
Due to the low frequency of thoracic surgery in children, it was difficult to include a control or comparative group in our study, this being its main weakness.
According to the detailed non-systematic review of previous publications in PubMed on noncardiovascular thoracic pathology treated with robotic surgery in the pediatric population worldwide, currently, the number of children treated with this technology barely has reached 100 cases, and all related references with the theme are included[11,22,26-34,36,39,44,45].
In conclusion, This pediatric series of RATS reports a small number of patients according to the low percentage of thoracic surgery in this population.The most frequent surgical techniques performed by RATS in children are: lobectomy, resection of benign masses and mediastinal cysts, thymectomy, plication, and closure of diaphragmatic defects.RATS in newborns and infants is a very difficult technique when they weigh between 3 and 5 kg, and patients under 3 kg are not candidates for this approach at present.Based on currently available evidence, it is not possible to suggest recommendations for the use of MIS for the treatment of intra-thoracic malignant tumors in children, including the robotic surgery.Currently, few children with malignant tumors treated with RATS have been reported.Its application in selected cases is an option, but oncological surgical principles should be applied.Our results are encouraging in RATS, although our experience is limited to a few cases.Robotic surgery for the treatment of thoracic pathology is feasible and safe, and has advantages.To date, few pediatric surgeons worldwide have applied RATS in children.
DECLARATIONS
Acknowledgments
I thank the Pediatricians and Pediatric Surgeons of the Department of Pediatrics of the Hospital Militar de Especialidades de la Mujer y Neonatología of Mexico City, as well as, to the resident physicians of the specialty of Pediatric Surgery, for their collaboration in referring patients for treatment with robotic surgery, also all those who collaborated in the surgical teams.
Authors' contributions
The author contributed solely to the article.
Availability of data and materials
The author cannot share the data according to the policy of the hospital institution, for reasons of confidentiality.
Financial support and sponsorship
None.
Conflicts of interest
The author declares to be Proctor of the da Vinci Surgical System and sometimes receives salary for advice to Surgeons in their first robotic procedures, from the marketing company in my country, as part of the support in the training of surgeons by this company.However, in relation to the treatment of patients and the execution of this manuscript, no economic financing was received from commercial companies.
Ethical approval and consent to participate
In relation to ethical considerations of the study, being of an observational nature, it was not necessary to obtain the informed consent for the patients to enter the study.The Research Ethics Committee of the Hospital evaluated and approved the study.In order to perform the medical-surgical procedures, we obtained the informed consent in writing from the parents or guardians.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2020.
杂志排行

Mini-invasive Surgery的其它文章
- Retraction: Diagnostic value of erythrocyte sedimentation rate levels as a predictor of stapleline leakage in bariatric surgery
- Robotic lobectomy costs and quality of life
- Robotic vs. traditional stapler use in robotic portal anatomic lung resection
- Subxiphoid uniportal video assisted thoracoscopic lobectomy in a pediatric patient
- Pain management following robotic thoracic surgery
- Utility of a lighted stent to avoid male urethral injury in transanal rectal surgery