Sternal Hodgkin’s lymphoma: A case report and review of literature
2020-05-14
Yi-Yu Yin, Nan Zhao, Bin Yang, Hua Xin, Department of Thoracic Surgery, China-Japan Union Hospital of Jilin University, Changchun 130000, Jilin Province, China
Abstract
BACKGROUND
Sternal tumors are difficult to diagnose, and usually need to be differentiated from other diseases such as tuberculosis, osteosarcoma, intrathoracic thyroid and thymoma. The sternum is a rare site of Hodgkin’s lymphoma, which is often misdiagnosed as tuberculosis on routine histopathology.
CASE SUMMARY
We reported a 47-year-old female patient with chest pain in the upper sternum for 1 mo. Chest computed tomography found a mass in the upper sternum.Pathology and immunohistochemistry of the biopsy confirmed the diagnosis of typical Hodgkin’s lymphoma (mixed cellularity subtype). Patient was diagnosed with primary sternal Hodgkin’s lymphoma and administered 6 cycles of adriamycin, bleomycin, vinblastine, and dacarbazine chemotherapy. Patient had no tumor recurrence and progression at a follow-up visit 2 years later.
CONCLUSION
This study highlights the rarity of primary sternal Hodgkin’s lymphoma and the challenges of its diagnosis. A PubMed and Web of Science search revealed 10 reported cases of sternal involvement in Hodgkin’s lymphoma.
Key words: Sternum; Skeleton; Hodgkin’s Lymphoma; Chest pain; Case report
INTRODUCTION
Lymphomas, both Hodgkin lymphomas (HL) and non-HL, comprise approximately 5% to 6% of all malignancies, approximately half of all newly diagnosed hematological tumors[1,2]. HL is a type of lymphoma that originates from B lymphocytes and characteristically presents in a group of lymph nodes, most commonly in the cervical and supraclavicular lymph nodes (LN)[3]. Extranodal HL,especially in sternum, is extremely rare. This study highlights the rarity of primary sternal Hodgkin’s lymphoma and the challenges of its diagnosis.
CASE PRESENTATION
Chief complaints
Chest pain in the upper sternum for 1 mo in a 47-year-old woman.
History of present illness
The patient presented to our department with complaints of paroxysmal chest pain,radiating to the left side, and associated with fatigue, fever of 37.8 °C, and significant weight loss (6.5 kg over 3 mo), these symptoms gradually aggravated within 1 mo.Patient denied experiencing night sweats or other symptoms.
History of past illness
The patient had no history of other diseases.
Personal and family history
She had no history of cigarette smoking or alcohol use, and there were no similar cases in the family.
Physical examination upon admission
Physical examination after admission revealed the following: blood pressure of 110/70 mmHg, pulse of 80 beats/min and temperature of 37.5 °C. The general examination was unremarkable, and no palpable lymph nodules were found. Chest examination revealed a solid mass in the upper sternal segment. On palpation, the swelling was fixed, firm, and non-tender with smooth edges without redness and ulceration, and no obvious abnormality was found in other systemic examinations.
Laboratory examinations
Blood test results were as follows: Differential counts of neutrophils, 72.9%;lymphocytes, 19.8%; platelet counts, 257 × 109/L; lactate dehydrogenase level, 169.69 IU/L and human immunodeficiency virus was negative.
Imaging examinations
Chest contrast-enhanced computed tomography (CT) (Figure 1) showed a patellar low-density shadow in the upper sternum, surrounding a soft tissue mass measuring 3.9 cm × 2.8 cm with mild enhancement. The initial diagnosis was a mediastinal mass.We performed a technetium 99m-methyl diphosphonate (Tc99MDP) bone scintigraphy scan (Figure 2) to exclude other skeletal system tumors in the patient. The results revealed apparent fixation of the radiopharmaceuticals in the sternal manubrium and upper segment of the sternal body, and no involvement of other sites in the skeleton was found.
FINAL DIAGNOSIS
A histopathological biopsy (Figure 3) from the swelling revealed that most tissues were necrotic and contained inflammatory granulation, blood vessels, lymphocytes,plasma cells and a few large heterotypic cells (suspected to be Reed Sternberg cells).On immunohistochemistry (Figure 4): CD30 (+), Pax-5 (+), Ki67 (60%+), CD20 (-), and CD5 (-) were revealed, indicating a pattern typical of classical Hodgkin’s lymphoma(mixed cellularity, MC).

Figure 1 Chest contrast enhanced computed tomography scan. Patchy low-density shadows were seen in the upper sternum, and soft tissue mass formation was observed around the upper sternum, with a size of 3.9 cm × 2.8 cm and slight enhancement.
TREATMENT
To prevent disease progression and relieve symptoms, patient was administered 6 cycles of the ABVD regimen (Adriamycin 25 mg/m2, Bleomycin 10 mg/m2,Vinblastine 6 mg/m2, and Dacarbazine 375 mg/m2every 28 d). Patient’s symptoms improved significantly after the treatment, and chest CT examination (Figure 5)revealed a 90% reduction in the size of the mass lesion.
OUTCOME AND FOLLOW-UP
Patient has achieved complete remission after treatment and followed up for 2 years without recurrence of the tumor or clinically detectable lymph nodes enlargement.
DISCUSSION
HL is a type of lymphoma that originates in B lymphocytes, which characteristically presents in a group of lymph nodes (LN), most commonly in the cervical and supraclavicular LN. Four typical subtypes of HL are defined: Lymphocytic predominance, nodular sclerosis, MC, and lymphocytic depletion[3]. Extranodal HL is extremely rare and most commonly presents in the gastrointestinal tract, respiratory system, thyroid gland, skin, urogenital tract and central nervous system[4]. HL initially manifesting in the skeleton is rare because bone involvement is a peculiarity of advanced HL and occurs in about 10%-20% of cases at some stages of the disease course[5]. Although some cases of HL may initially appear with skeletal symptoms,other findings may eventually indicate the involvement of other areas, such as the mammary[6], the supraclavicular[7], the axillary[8], and the inguinal LNs[9]. Primary HL of the skeleton is extremely rare with an incidence of only 1%-4%.[7]Biswaset al[10]reported that the spine, pelvis, ribs, femur and clavicle are the most common sites of bone involvement in HL, while sternum involvement is distinctly uncommon.Primary bone lymphoma is defined as being limited to bone with or without an associated soft tissue component and no regional lymphadenopathy at diagnosis and during the 6-mo follow-up. Bone involvement is classified as stage IV HL, but primary solitary osseous HL is defined as stage IE according to the Ann Arbor staging[4].
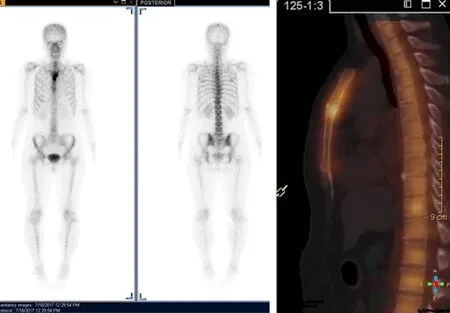
Figure 2 Bone scintigraphy scan with Tc99-MDP. Apparent fixation of the radiopharmaceuticals in the manubrium sternum and upper segment of the body of the sternum. No involvement of other sites of the skeleton was found.
Sternal tumors confer certain difficulties in clinical diagnosis, and usually need to be differentiated from other diseases such as tuberculosis, eosinophilic granuloma,osteosarcoma, intrathoracic thyroid and thymoma. Therefore, patients often delay treatment or even die because of misdiagnosis. Hence, in such patients with sternal pain, HL should be cautiously considered, although HL involving the sternum is very rare. In our case, the patient was admitted to the hospital with complaints of chest pain for 1 mo, in view of the patients’ age, symptoms, physical signs and imaging examination results, a mediastinal mass was considered as the primary diagnosis. For further diagnosis and treatment and to prevent misdiagnosis, the patient underwent a tissue biopsy and was finally diagnosed with sternal HL (MC) based on the pathological results. Following 6 cycles of chemotherapy, the patient achieved complete remission. Although CT, magnetic resonance imaging and positron emission tomography can be used for the diagnosis of chest wall or sternal tumors, careful clinical and comprehensive diagnostic workup is still needed in the treatment of such cases, which can improve the diagnosis rate, and avoid ultimate death due to misdiagnosis.
We conducted a search of PubMed and Web of Science using the key words“Hodgkin’s, sternum” for papers published from 2000 to 2019 and summarized 11 articles in Table 1. Nine patients had involvements in the LNs, 3 had involvements at other skeletal sites, and 2 patients had isolated and primary sternal involvement. Men had a higher prevalence than women (6, 54.55%) and the mean age was 29 years(ranged from 7-82, R software 3.5.1 was used). Histological results were available in 7 articles, NS was the most common subtype, which accounted for 71.43%, and MC accounted for 28.57%. Five cases (45.45%) were initially misdiagnosed (most commonly with tuberculosis). Chemoradiotherapy was the most common treatment(5, 45.45%), followed by chemotherapy (4, 36.36%) and one patient was treated by stem cell transplantation. Based on the review, about half of the patients were misdiagnosed initially, and only 2 patients were diagnosed with primary sternal HL,but they both experienced relapses; thus, our case is the first reported case diagnosed at initial presentation with a primary lesion.
CONCLUSION
This study highlights the rarity of primary sternal Hodgkin’s lymphoma and the challenges of its diagnosis. Because of the rarity of such tumors, we report this case to raise awareness of this disease.
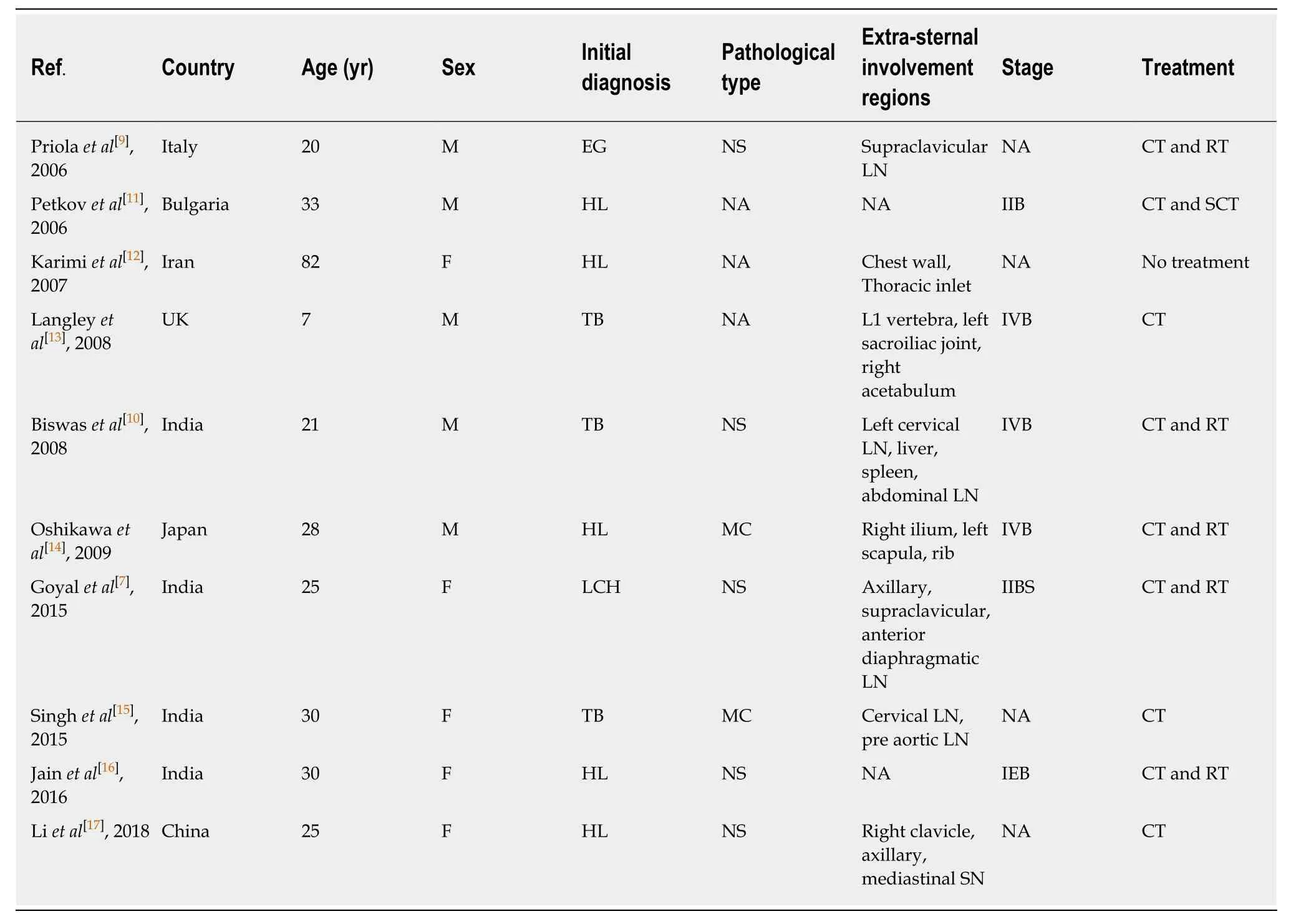
Table 1 Literature review of sternal Hodgkin’s lymphomas
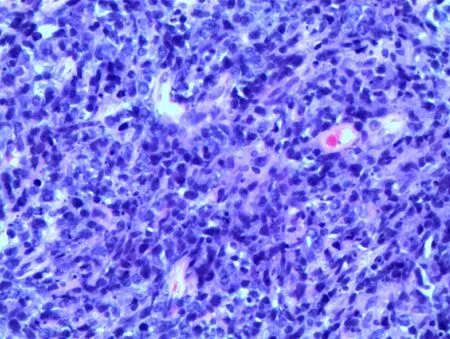
Figure 3 Hematoxylin and eosin staining (original magnification 200 ×). Lymphocytes, plasma cells and a few large heteromorphic cells (Suspected Reed Sternberg cells).
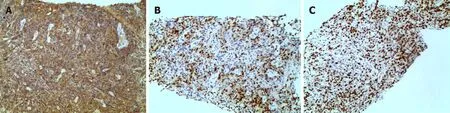
Figure 4 Immunohistochemical staining (original magnification 100 ×). A: CD 30(+); B: PAX-5(+); C: Ki-67(60%+).

Figure 5 Chest computed tomography shows that the mass around the upper sternum was reduced obviously.
杂志排行

World Journal of Clinical Cases的其它文章
- Comprehensive review into the challenges of gastrointestinal tumors in the Gulf and Levant countries
- Can cyclin-dependent kinase 4/6 inhibitors convert inoperable breast cancer relapse to operability? A case report
- Ruptured splenic peliosis in a patient with no comorbidity: A case report
- Successful kidney transplantation from an expanded criteria donor with long-term extracorporeal membrane oxygenation treatment: A case report
- Boarding issue in a commercial flight for patients with cavitary pulmonary tuberculosis: A case report
- Cytomegalovirus ileo-pancolitis presenting as toxic megacolon in an immunocompetent patient: A case report