Resorption of upwardly displaced lumbar disk herniation after nonsurgical treatment:A case report
2020-04-09YiWangShiChuanLiaoGuoGangDaiLingJiang
Yi Wang,Shi-Chuan Liao,Guo-Gang Dai,Ling Jiang
Yi Wang,Shi-Chuan Liao,Guo-Gang Dai,Cervicodynia/Omalgia/Lumbago/Sciatica Department 2,Sichuan Provincial Orthopedics Hospital,Chengdu 610041,Sichuan Province,China
Ling Jiang,College Hospital,Sichuan Agricultural University-Chengdu Campus,Chengdu 611130,Sichuan Province,China
Abstract BACKGROUND The spontaneous resorption of lumbar disk herniations(LDHs)has been widely reported.However,the majority of these reports analyze the resorption of LDHs that were displaced backwards or downwards.There have been few reports on the spontaneous resorption of upwardly displaced L4/5 LDH that has caused femoral nerve symptoms.CASE SUMMARY A 55-year-old woman presented to our hospital with acute pain in her left leg.She had been suffering from recurrent lower back pain for approximately 1 year and began to feel pain accompanied with numbness at the anterior aspect of her left leg 7 d previously.On examination,a typical L4 nerve stimulation was noted.An upwardly displaced LDH at the L4/5 level was revealed by magnetic resonance imaging.The patient attained complete relief of her symptoms after 10 wk of nonsurgical treatment and the upwardly displaced herniation almost entirely disappeared.There was no recurrence during a follow-up of 2 years.CONCLUSION Clinicians should be aware that the nerves disturbed by LDHs vary according to the direction of the herniations and the probable resorption of upwardly displaced LDHs should be considered before making a decision on surgery.
Key Words:Lumbar disk herniation;Upward displacement;Resorption;Neurology;Rehabilitation;Case report
INTRODUCTION
Lumbar disc herniation(LDH)can be treated non-surgically or surgically[1,2].Resorption of LDH is one of the primary factors that contributes to relief following nonsurgical treatments;and thus has clinical significance in the nonsurgical treatment of LDH.The spontaneous resorption of LDHs has been widely reported[3-16].However,the majority of these reports analyze the resorption of LDHs that were displaced backwards or downwards in the form of sequestration,extrusion,protrusion,or bulging[17].The natural history of upwardly displaced LDHs has rarely been documented.In addition,upwardly migrated LDHs may exhibit a different pattern in disturbing nerve roots compared with LDHs displaced backwards or downwards.Therefore,we present this case study to demonstrate the femoral nerve symptoms that result from upwardly displaced L4/5 LDHs and provide an example of the spontaneous resorption of an upwardly displaced L4/5 LDH.
CASE PRESENTATION
Chief complaints
A 55-year-old woman presented to our hospital with acute pain in her left leg for 7 d.
History of present illness
The patient had been suffering from recurrent low back pain for approximately 1 year,and her pain was relieved spontaneously or after nonsurgical treatment.She began to feel pain accompanied by numbness at the anterior aspect of her left leg 7 d before presentation.
History of past illness
The patient underwent appendectomy for appendicitis 15 years ago.
Physical examination
Clinical examination revealed the following:a negative Lasegue’s sign and a positive femoral nerve stretch test of her left leg,hypoesthesia over the distribution of the left femoral nerve,and normal muscle strength and deep tendon reflexes of her legs with a bilateral negative Babinski’s sign.She perceived an electric shock-like sensation in her left leg prompted by lumbar spine extension.
Laboratory examinations
Routine blood,blood biochemistry,serum C-reactive protein level and erythrocyte sedimentation rate were normal.
Imaging examinations
An upwardly displaced LDH at the L4/5 level was revealed by magnetic resonance imaging(MRI)(Figure 1).
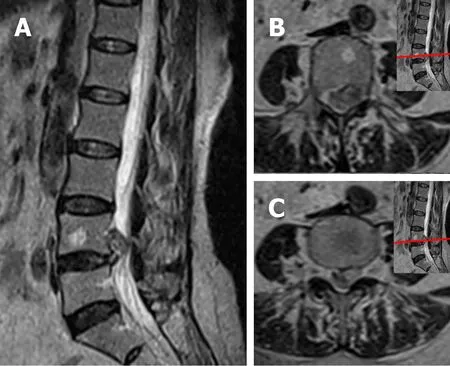
Figure 1 Magnetic resonance imaging obtained at the patient’s initial visit.A:Sagittal T2-weighted magnetic resonance imaging revealed an L4/5 lumbar disk herniation moved upward to above the L4/5 disc level,lying behind the L4 vertebral body;B and C:Axial T2-weighted magnetic resonance imaging revealed that the lumbar disk herniation compressed the L4 nerve root at the left posterolateral of the L4 vertebral body.
FINAL DIAGNOSIS
The patient was diagnosed with an upwardly displaced L4/5 LDH.
TREATMENT
The patient received nonsurgical treatment with Traditional Chinese Medicine for 4 wk,which included bed rest,acupuncture,massage,moxibustion and Chinese medicine fumigation.All of her symptoms were relieved except for moderate lumbago,and she was discharged from the hospital.She underwent a follow-up visit every 2 wk and performed home-based exercise therapy following the doctor's instructions for 6 wk.
OUTCOME AND FOLLOW-UP
She attained complete relief of her symptoms 10 wk after presentation.The upwardly displaced herniation mostly disappeared on the second MRI,which was performed 10 wk after her initial visit(Figure 2).There was no recurrence during a follow-up of 2 years,and only a small amount of herniated disc tissue was found on the third MRI,which was performed 2 years after the patient’s initial visit(Figure 3).
DISCUSSION
The resorption of LDHs after nonsurgical treatments has been widely reported since the first case in 1984.In these reports,the LDHs were characterized as decreasing or disappearing over time,and the nonsurgical treatments in these reports included bed rest,lumbar support,analgesics,oral steroids,non-steroidal anti-inflammatory drugs,epidural steroid injection,caudal epidural injections of local anesthetic,manipulation,hot back,ultrasound,electrotherapy,traction,exercises,Traditional Chinese Medicine and integrative Korean medicine[3-16].However,which of these treatments are essential for promoting resorption and the time when resorption takes place remains unclear.
The incidence of resorption varies in the existing reports depending on the different follow-up times.Lee reported the highest incidence of resorption of 96% with an average follow-up time of 341.38 ± 306.83 d[3].Two studies reported no resorption with follow-ups of 45 d[4]and 20 d[5],suggesting that resorption should not be expected to occur too soon after nonsurgical treatments.The relationship between the incidence of resorption and the time of follow-up was not consistent in these studies,and no secular trends in the incidence of resorption were identified in these studies(Table 1).
A meta-analysis reported the overall incidence of resorption of LDHs to be 66.66%(95%CI:55.12%-78.21%)[18],and randomized controlled trials have confirmed that resorption is a widespread phenomenon in patients with LDHs[7,12,19].The North American Spine Society has suggested that the probability of resorption should beconsidered during the management of LDH[20].Although it is well known that sequestrated and large LDHs are more likely to undergo resorption[21-23],it is still not possible to accurately predict resorption in individual cases;even the possibility of resorption cannot be predicted for individual cases.Thus,for many cases that present without cauda equina syndrome or progressive neurological deficits,there remains no consensus on whether to perform surgical treatments or nonsurgical treatments[1].However,we cannot ignore the physical decompression that occurs during resorption of LDH,and the probability of resorption should be considered before making a decision on surgery.

Table 1 Incidence of resorption of lumbar disk herniations reported at different follow-up times
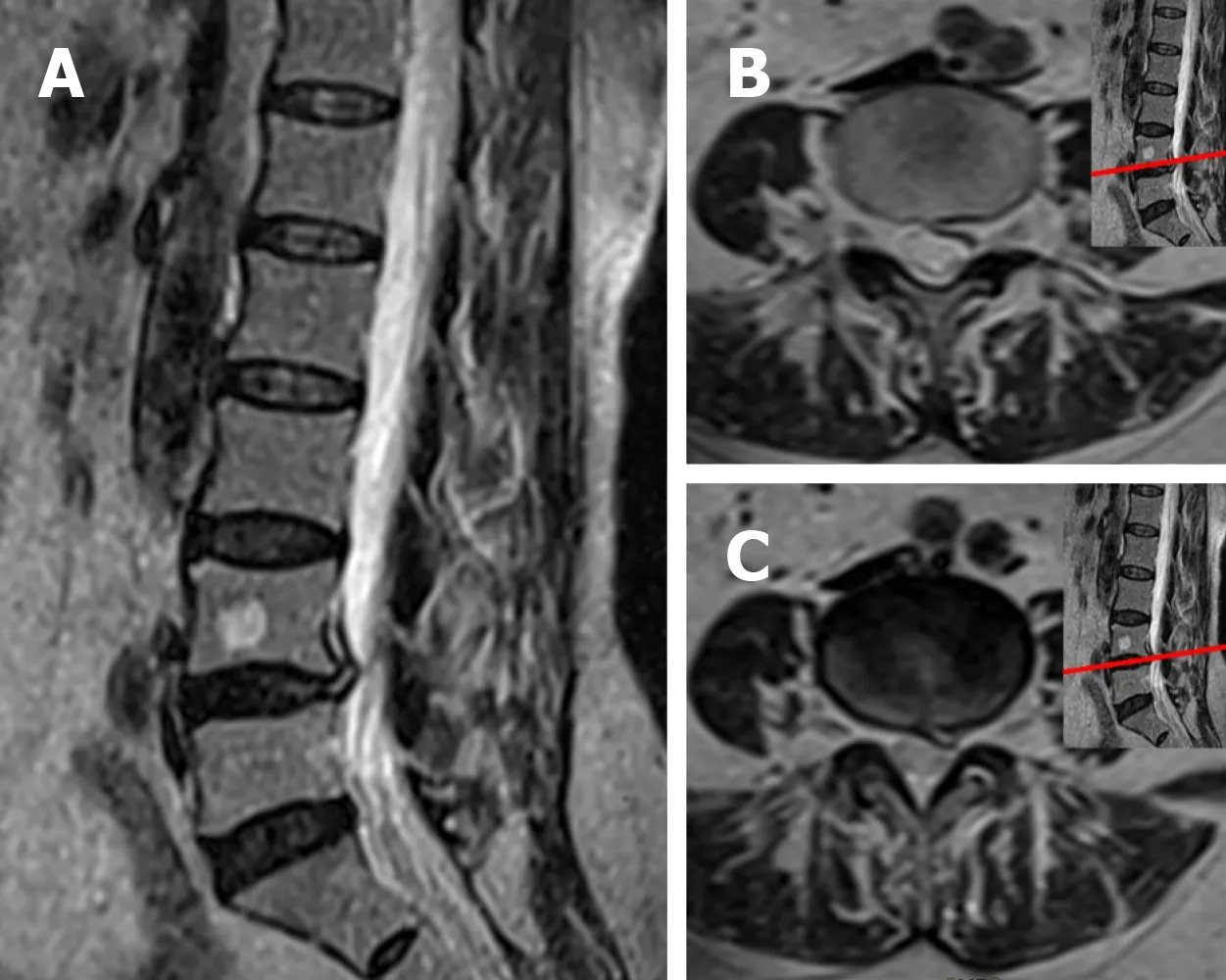
Figure 2 Magnetic resonance imaging obtained 10 wk after the patient’s initial visit.A:Sagittal T2-weighted magnetic resonance imaging revealed that most of the upwardly displaced disc material had disappeared;B and C:Axial T2-weighted magnetic resonance imaging revealed that a small amount of herniated disc material was visible at the left posterolateral of the L4 vertebral body and the L4/5 disc.
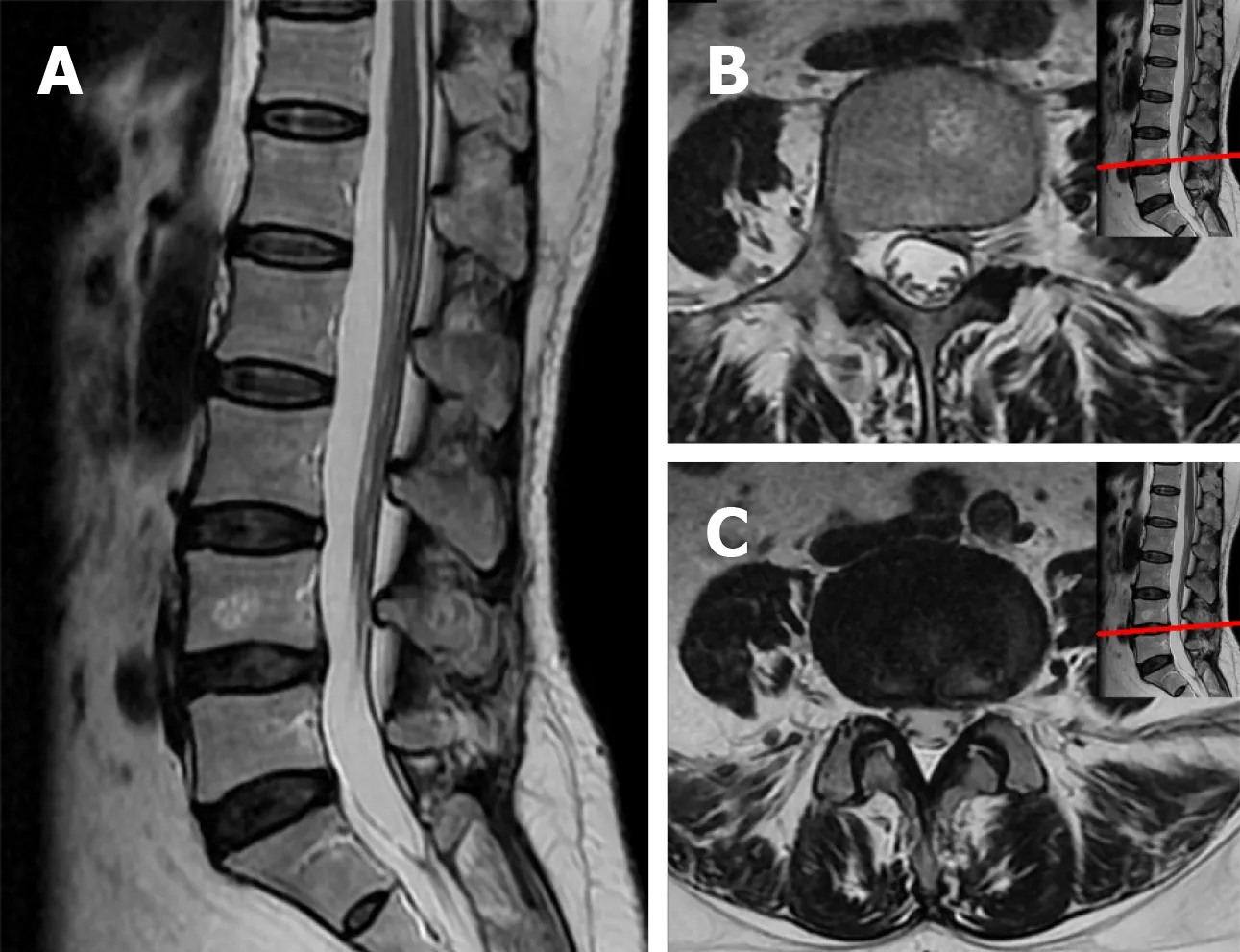
Figure 3 Magnetic resonance imaging obtained 2 years after the patient’s initial visit.A:Sagittal T2-weighted magnetic resonance imaging(MRI)revealed the upwardly displaced disc material had almost completely disappeared;B:Axial T2-weighted MRI revealed that a small amount of herniated disc material was visible at the left posterolateral of the L4 vertebral body;and C:Axial T2-weighted MRI revealed that the herniated disc material at the left posterolateral of the L4/5 disc had disappeared.
The epidural space enlarges down the vertebral column[24].Thus,in the majority of cases,the LDH tends to protrude downward under the influence of gravity.Most of the existing studies reported resorption of backwardly or downwardly displaced LDHs,while upwardly displaced LDHs have been reported less.Mackiet al[25]reported a case of an upwardly migrated L4/5 LDH that was compressing the L5 nerve root and resorbed 5 mo after nonsurgical treatment.Another case presented the resorption of an upwardly migrated L4/5 LDH in a pregnant woman with sciatica[26].The upwardly displaced L4/5 LDHs of these two cases stimulated the L5 nerve root and resulted in sciatica.
There have been few reports on the spontaneous resorption of upwardly displaced L4/5 LDH that has caused femoral nerve symptoms.In most cases,LDH compresses the nerve root corresponding to the lower vertebral level;accordingly,L4/5 LDH disturbs the L5 nerve root,which originates at the L4/5 disc level and goes downward to the L5/S1 intervertebral foramen,subsequently causing sciatica.In rare cases,the L4/5 disc moves upward along the spinal canal to above the L4/5 disc level,and the herniated disc material is still connected to the L4/5 disc;the herniation may disturb the L5 nerve root at the starting point at the L4/5 disc level or disturb the L4 nerve root,which originates at the L4 vertebral level and leaves the spinal canal above the L4/5 disc plane,or disturb both.In the present case,the herniated L4/5 disc moved upwards to the L4 vertebral level above the starting point of the L5 nerve root,similar to a prolapsed L3/4 disc,leading to compression of the L4 nerve root,which originates at the L4 vertebral level and results in femoral nerve symptoms.The upwardly displaced L4/5 LDH of this patient almost completely disappeared and was accompanied by complete relief of the femoral nerve symptoms 10 wk following nonsurgical treatment with Traditional Chinese Medicine.
Upwardly displaced LDHs are not very common.To our knowledge,this is the first report of the spontaneous resorption of upwardly displaced L4/5 LDH that has caused femoral nerve symptoms.This case also demonstrated that the nerves disturbed vary according to the direction of the herniation.Resorption of the upwardly displaced LDH in this case corresponds with existing reports on the resorption of LDHs.
CONCLUSION
The nonsurgical treatment of this patient was successful.Clinicians should be aware that the nerves disturbed by LDHs vary according to the direction of the herniation,and the probable resorption of upwardly displaced LDHs should be considered before making a decision on surgery.Future research should explore the relationship between resorption and time as well as methods for predicting resorption.
杂志排行

World Journal of Clinical Cases的其它文章
- Role of monoclonal antibody drugs in the treatment of COVID-19
- Review of simulation model for education of point-of-care ultrasound using easy-to-make tools
- Liver injury in COVID-19:A minireview
- Transanal minimally invasive surgery vs endoscopic mucosal resection for rectal benign tumors and rectal carcinoids:A retrospective analysis
- Impact of mTOR gene polymorphisms and gene-tea interaction on susceptibility to tuberculosis
- Establishment and validation of a nomogram to predict the risk of ovarian metastasis in gastric cancer:Based on a large cohort