Woven coronary artery: A case report
2020-04-08WeiWeiQiZhangLiMingGao
Wei Wei, Qi Zhang, Li-Ming Gao
Wei Wei, Li-Ming Gao, Department of Cardiovascular Medicine, East Hospital, Tongji University School of Medicine, Shanghai 200120, China
Qi Zhang, Department of Cardiovascular Medicine, Tongji University School of Medicine,Shanghai 200124, China
Abstract BACKGROUND Woven coronary artery is an extremely rare disease with unknown etiology. This condition is difficult to diagnosis by traditional methods.CASE SUMMARY A 67-year-old male presented to the cardiology department with a history of mild chest pain for 6 mo. Coronary computed-tomography angiography revealed a soft plaque with a 40% stenosis in the right coronary artery (RCA). A linear shadow was seen both on left circumflex (LCX) and RCA. Further coronary angiography showed an 80% regional stenosis in the area proximal of LCX and RCA, and it was divided into different channels with diffuse stenosis. Intravascular ultrasound (IVUS) and optical coherence tomography (OCT) were performed in RCA. These confirmed a woven coronary artery. No stent was implanted. He remained asymptomatic during the 5-year follow-up period.CONCLUSION Woven coronary artery can be distinguished from spontaneous dissection and revascularization of thrombosis. IVUS and OCT are useful in obtaining a definite diagnosis, which decreases chances of unnecessary intervention.
Key Words: Woven; Coronary artery; Optical coherence tomography; Dissection; Case report
INTRODUCTION
Woven coronary artery (WCA) is a sporadic coronary disease, which is considered a benign condition[1], and most patients are asymptomatic. However, in some patients with WCA, sudden myocardial infarction or thrombosis may develop[2-4]. In addition,there have been reports of “woven-like” changes caused by revascularization thrombosis or spiral dissection[5-7], which are hard to distinguish by angiography.Currently, no long-time follow-up analysis of this disease is available. The pathology and etiology of woven coronary artery are elusive.
CASE PRESENTATION
Chief complaints
A 67-year-old male presented to the cardiology department with a 6 mo history of mild chest pain.
History of present illness
The patient had received coronary computed-tomography angiography, revealing that the left main artery (LM) was normal, and the right coronary artery (RCA) had a soft plaque with a 40% stenosis. A linear shadow was seen both on the left circumflex(LCX) and RCA, which was considered a spontaneous dissection.
History of past illness
The patient had a 30-year history of smoking and had no history of hypertension and diabetes.
Physical examination
No positive sign was found in the physical examination.
Laboratory examinations
No abnormality was found in the laboratory examinations.
Imaging examinations
To clarify the lesions, a coronary angiography was performed. A 70% stenosis was found in the LM coronary artery, and a 30%-40% stenosis in the proximal left anterior descending. An 80% regional stenosis was found in the area proximal of LCX, which was divided into different channels with diffuse stenosis hard to describe. In addition,a diffuse and thin channel was seen in the whole RCA, with a 50% stenosis at the proximal part (Figure 1). The thrombosis in myocardial infarction (TIMI) grade was 3 in all the three vessels. Both intravascular ultrasound (IVUS) and optical coherence tomography (OCT) were performed in RCA (Figure 2). These were multiple twisted channels with intact intima, without any sign of thrombosis. All the channels were independent, shared the same tunica in the proximal segment, and merged into one lumen in the distal without abnormal flow.
FINAL DIAGNOSIS
These examinations revealed a WCA.
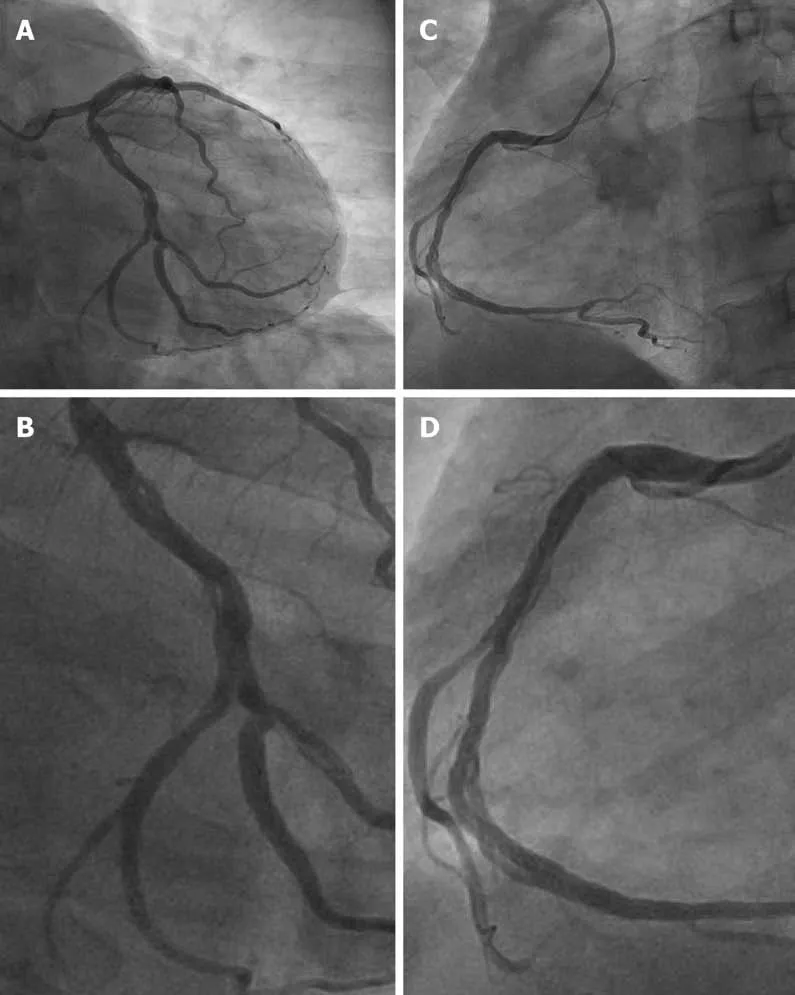
Figure 1 Image of the coronary angiography. A and B: The “woven” change in left circumflex; C and D: The “woven” change in right coronary artery.
TREATMENT
The tests suggested a benign condition that did not require further intervention. The patient was administered a single antiplatelet agent and statin before discharge from the hospital.
OUTCOME AND FOLLOW-UP
He was healthy and asymptomatic at the 12-mo follow-up and remained asymptomatic during the 5-year follow-up period. He continued with a single antiplatelet agent and statin for 5 years.
DISCUSSION
In 1988, Dr. Sane reported the first case of “8” sign in the right coronary artery angiography[7]. The vascular malformation looked woven, so the condition was named"woven coronary artery". Characteristically, the epicardial coronary artery is divided into multiple thin channels at the proximal segment and converged together in the distal segment, with a TIMI III distal blood flow. It was considered a benign coronary condition and a congenital anatomical anomaly. In some cases, WCA may cause acute coronary syndrome or sudden death when concomitant with atherosclerosis.
The etiology of WCA has remained unknown, but some researchers believe that it may arise from spontaneous coronary artery dissection[5]. However, it does not cause abnormal blood flow or nutrient supply or intramural hematoma. Other researchers have considered it a congenital vascular dysplasia. Previously, angiogenesis and arteriogenesis have been linked to the development of WCA. Other factors, such as slow flow, inflammation, and growth factors, are associated with the occurrence of WCA. Animal experiments confirmed that growth factors may promote the growth of coronary collateral vessels. It is also speculated that intrauterine inflammation might cause unbalanced development of the coronary artery, thereby leading to WCA.
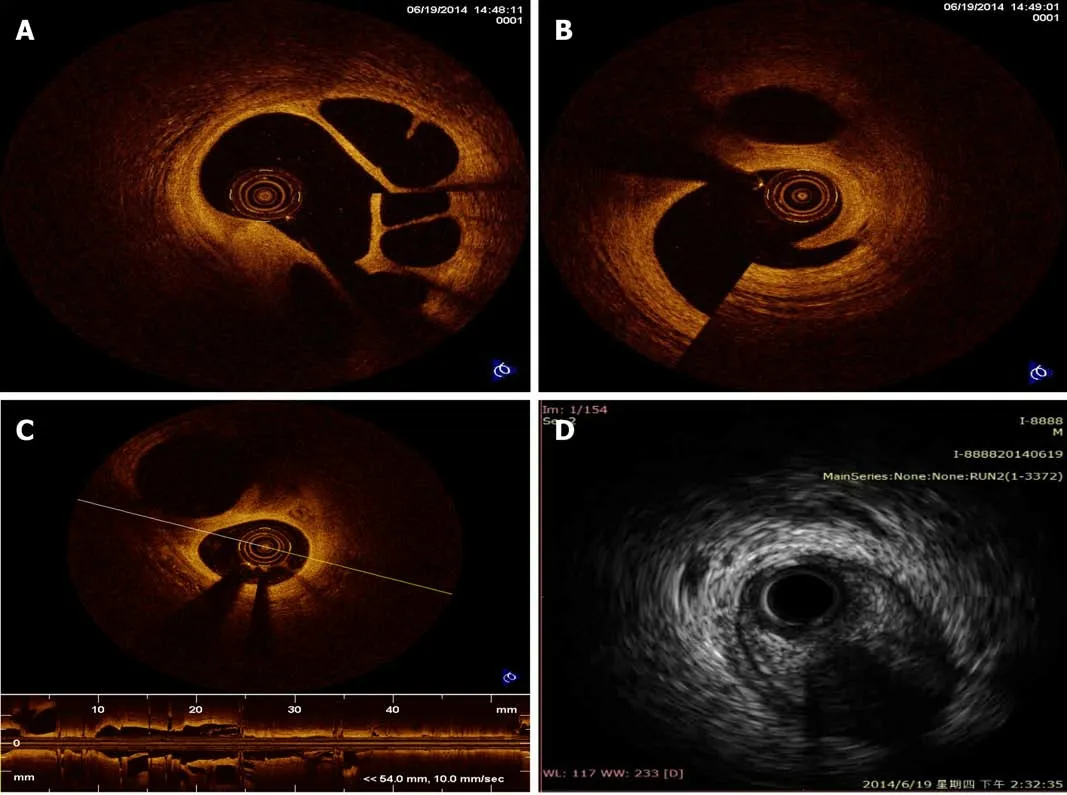
Figure 2 Optical coherence tomography and intravascular ultrasound images in right coronary artery. A-C: Multiple twisted channels without traces of thrombosis or dissection flaps are shown by optical coherence tomography in right coronary artery; D: Intravascular ultrasound shows multiple cavities filled with blood speckling in right coronary artery.
A previous report stated that WCA can be diagnosed by coronary angiography.WCA most frequently involves the right coronary artery (54.5%), the left anterior descending artery (13.6%), and the left circumflex artery (9.1%), in that order[8]. Both left and right coronary arteries were involved in the current case. The average length of segments involved in WCA was 2.2 cm (range of 1.0-5.0). The WCA could be distinguished from spontaneous dissection and revascularization of thrombosis with or without intervention. These two conditions may show a similar pattern on angiography but have different prognosis following respective treatments. Thus,coronary angiography alone is not sufficient to make a definitive diagnosis. An intervascular image (such as IVUS and OCT) should be obtained to delineate the lumen and wall for a definite diagnosis. Here, OCT revealed multiple spiral tunnels separated by fibrous tissue in the local lumen[9]. In WCA, each tunnel contains a relatively complete three-layer vascular structure, which distinguishes WCA from thrombosis revascularization. The diagnostic features of IVUS were similar to those of OCT.
CONCLUSION
WCA is often considered a benign variant because of its normal blood flow. The lumen diameters of the true WCA between different tunnels are narrowed. If misdiagnosed as thrombus recanalization, a large coronary stent may be used, leading to vascular rupture. Therefore, clinical follow-up is recommended for WCA if there is no flow restriction. IVUS and OCT can be used to make a definite diagnosis and reduce unnecessary intervention. If stenosis or thrombosis are seen, coronary artery bypass grafting combined with medications may be safer than stent implantation based on intravascular imaging. It is unknown whether antiplatelet and statin drugs are effective in this case.
Although WCA appears to be benign without any major adverse cardiovascular events, more data and in-depth research are needed to understand this sporadic disease.
杂志排行
World Journal of Clinical Cases的其它文章
- Relationship between non-alcoholic fatty liver disease and coronary heart disease
- Remission of hepatotoxicity in chronic pulmonary aspergillosis patients after lowering trough concentration of voriconazole
- Endoscopic submucosal dissection as alternative to surgery for complicated gastric heterotopic pancreas
- Observation of the effects of three methods for reducing perineal swelling in children with developmental hip dislocation
- Predictive value of serum cystatin C for risk of mortality in severe and critically ill patients with COVID-19
- Sleep quality of patients with postoperative glioma at home