Polymyxin B hemoperfusion as a feasible therapy after source control in abdominal septic shock
2019-12-31JinJooKimYoungJunParkKiYoonMoonJinHyeongParkYongKiJeongEunYoungKim
Jin Joo Kim, Young Jun Park, Ki Yoon Moon, Jin Hyeong Park, Yong Ki Jeong, Eun Young Kim
Jin Joo Kim, Eun Young Kim, Division of Trauma and Surgical Critical Care, Department of Surgery, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea,Seoul 137-701, South Korea
Young Jun Park, Ki Yoon Moon, Jin Hyeong Park, Yong Ki Jeong, Department of Surgery, Seoul St. Mary's Hospital, Seoul 137-701, South Korea
Abstract
BACKGROUND
Polymyxin B hemoperfusion (PMX-HP) has been used as a treatment for intraabdominal septic shock by absorbing and removing endotoxins of gram-negative bacilli.
AIM
To investigate the clinical efficacy of PMX-HP in patients with gram-negative septic shock who underwent abdominal surgery.
METHODS
From January 2012 to December 2018, patients who had septic shock secondary to peritonitis were enrolled. They were classified into PMX-HP treated and control groups based on postopreative intervention using PMX-HP. The clinical outcomes were compared using 1:1 propensity score matching methods to balance the overall distribution between the two groups.
RESULTS
After propensity score matching, 40 patients were analyzed (20 patients in the PMX group and 20 patients in the control group). The scores of total Sequential Organ Failure Assessment (SOFA) score, renal SOFA and coagulation SOFA were significantly improved in the PMX group but not in the control group. (from 11.2± 5.8 to 4.7 ± 3.5 in PMX group vs 10.0 ± 4.0 to 8.7 ± 7.3 in control group, P = 0.047 from 2.6 ± 1.0 to 0.7 ± 1.0 in PMX group vs 2.6 ± 1.5 to 2.8 ± 1.6 in control group, P= 0.000, from 1.6 ± 1.5 to 1.3 ± 1.3 in PMX group vs 1.2 ± 1.2 to 2.8 ± 1.8 in control group, P = 0.014, respectively). Further, the length of intensive care unit (ICU)stay was significantly shorter in PMX group. However, no statistically significant difference was found in ICU mortality (50% in PMX group vs 50% in control group).
CONCLUSION
PMX-HP is a feasible adjunct treatment for peritonitis in ICU patients with peritonitis for improved organ impairment and to stabilize hemodynamics. It would be helpful to enhance clinical outcomes especially in patients with complete elimination of the source of gram-negative bacilli infection by surgical procedure accompanied with conventional treatment of sepsis.
Key words: Intraabdominal septic shock; Panperitonitis; Polymyxin B hemoperfusion;Sepsis; Toraymyxin
INTRODUCTION
Intra-abdominal infection is one of the common causes of sepsis or septic shock and is associated with a high mortality rate of 19.5%[1,2]. Because of the inherent bacterial colonization in abdomen, gram-negative bacilli (GNB) are probably the major source of infection[3,4]. Lipopolisaccharide (LPS) is the core lipid portion of the endotoxin in gram-negative microorganisms, and has been considered as one of the important triggers of sepis or septic shock[5]. It induces a systemic inflammatory response syndrome resulting in the release of cytokines such as tumor necrosis factor-α (TNFα), interleukin-1β (IL-1β) and nitrous oxide, and also activates the coagulation and complement system of the host[1,6]. Moreover, LPS translocation into the blood stream when the intestinal mucosa is impaired in sepsis, results in multiorgan failure[3].
Polymyxin B (PMX) is an antibiotic, which binds to LPS of GNB and inactivates the endotoxin with increased affinity. Hemofiltration with PMX hemoperfusion (PMXHP, Toraymyxin, Toray Industries, Tokyo, Japan) immobilized to a polysterenederived fiber was developed in Japan in the 1990s, to selectively adsor and remove the endotoxin of GNB in the blood stream[5,7-9]. Since 2017, our institution have used the PMX-HP in selected patients who underwent surgery for the treatment of septic shock originated from abdominal peritonitis. However, there is still lack of a comparative study of the effectiveness of PMX-HP treatment after abdominal surgery, and PMXHP is not routinely used to manage post-operative patients with peritonitis.
Herein, we evaluated the clinical efficacy of PMX-HP treatmentviapropensity score matching in patients undergoing abdominal surgery due to peritonitis with gram-negative sepsis.
MATERIALS AND METHODS
Study design and participants
This study was approved by the Institutional Review Board of our institution (No.IRB; KC18RESIO782). Patients who manifested septic shock secondary to peritonitis between January 2012 and December 2018 were enrolled. All the patients were diagnosed with abdominal septic shock due to suspected or established GNB infection, and they underwent surgical control of the source of infection.Subsequently, the patients received standard management based on Survival Sepsis Campaign (SSC) guidelines for sepsis[10,11]. The diagnosis of severe sepsis and septic shock was defined according to the SSC criteria[12]. Patients were treated according to SSC bundle with appropriate volume resuscitation, the culture prior to administration of antibiotics and usage of vasopressor. In addition, the culturing multiple sites including blood, sputum, drain or urine were performed during the intensive care unit (ICU) stay[6]. Gram-negative etiology of sepsis was strongly suspected according to the source of infection or based on microbiological tests[3]. All participants were classified into postoperative PMX-treated and untreated control group. Since 2016,patients at our institution have been treated with PMX-HP in the surgical intenstive care unit after source control following a diagnosis of intra-abdominal infection with septic shock. Based on the Early Use of Polymyxin B Hemoperfusion in Abdominal Septic Shock (EUPHAS) 1 trial, we adopted PMX-HP treatment based on our own guidelines. The indications for PMX-HP were same as follows: (1) Age over 18 years;(2) Clinical signs of sepsis or septic shock originating in the abdominal cavity with a Sequential Organ Failure Assessment (SOFA) score > 2; (3) Persistence or worsening of septic shock despite appropriate antibiotic treatments and effective source control;(4) Need for high dose of vasopressor within 12 h from diagnosis; and (5) Suspected or confirmed gram-negative infection traced to a recognized source of sepsis[1,8,13-15].PMX-HP was not used to treat cases with the following contraindications: (1) Age less than 18 years; (2) Incomplete source control due to poor condition of patients; (3)Pregnancy; (4) Previous history of hypersensitivity to PMX; (5) Uncontrolled hemorrhage within 24 h; (6) Severe thrombocytopenia (platelet count < 30000 ×109/L); (7) Severe leukocytopenia (leucocyte count < 500 µL/L); (8) Hematologic malignancy; or (9) Immunosuppressive therapy[6,15,16]. The control group was treated using standard intensive therapy according to guidelines recommended by SSC after surgical source control[10,11].
In this study, the source control was defined as any surgical procedure or intervention, which eliminates the focus of ongoing infection and also corrects the anatomical derangements involving intra-abdominal viscera in order to restore normal physiologic function[17]. According to Solomkinet al[18], the successful source control was defined as the case obtaines these findings after surgery or intervention;resolution of fever (oral temperature < 37.5 °C), improvement in leukocytosis [white blood cell (WBC) < 12000 µL/L], resolution of physical findings of tenderness and rigidity, restoration of enteric function and no further need for operative or other intervention[18]. However, the failure of source control was defined by a strong clinical suspicion of infection in the abdomen based on the color change of the drain, the result of imaging study such as computed tomography scan or clinical progression to septic condition despite operation or intervention. Patients manifesting any of these findings were excluded from the analysis; previously signed “do not resuscitate”orders, those with documented treatment limitations such as prohibition of further organ support or initiation of renal replacement therapy, as stated in the medical records.
Study protocol: Polymyxin B hemoperfusion group vs control group
The study protocol is summarized in Figure 1. In case of PMX group, the first PMXHP session was initiated within 12 h after surgical source control followed by a second PMX-HP session within 24 h after completion of the first session. A duallumen catheter (12Fr Arrow International, Reading, PA, United States) was inserted into the internal jugular vein or femoral vein guided by ultrasound. Subsequently,two sessions of PMX-HP were performed using toraymyxin cartridge (Toraymyxin,Toray industries, Tokyo, Japan) in the continuous renal replacement therapy (CRRT)machine. The blood flow rate varied between 80 to 120 mL/min, and Nafamostat mesylate (Futhan, Torii Pharmaceuticals, Tokyo, Japan) was used as anticoagulant for the circuit at a dose of 20-30 mg/h[3,19]. Based on the study of Kawazoeet al[20], each session was conducted for 6 h except in cases indicated for PMX-HP therapy discontinuation. To reduce the risk of postoperative bleeding, nafamostat was also used for patients with CRRT in the control group according to our institution's policy.
Data collection and study endpoint

Figure 1 Design of the study protocol from the operation until second session of polymyxin B hemoperfusion.
For each patient, the data were prospectively collected from medical records and vital chart at baseline, at 48 h and at 72 h. In terms of hemodynamic status, it was assessed according to their mean arterial pressure (MAP), blood lactate concentration, and vasopressor load represented by the inotropic score [Inotropic score = (dopamine dose × 1) + (dobutamine dose × 1) + (adrenaline dose × 100) + (noradrenaline dose ×100) + (phenylephrine dose × 100)].
All doses were expressed as µg/kg/min. Because the vasopressor dose was titrated to maintain MAP of 65 mmHg, a dose-response relationship between MAP and vasopressor dose was expressed as the vasopressor dependency index (VDI) (VDI =Inotropic score/MAP).
On the aspect of PMX-HP, the duration, and the frequency and, the time to initiation of PMX-HP were recorded. The degree of organ dysfunction was expressed using the SOFA score[21]. Adverse events related to PMX-HP were defined by tachycardia (heart rate > 100 bpm) or heart rate increase greater than 10% at the beginning of PMX-HP, hypotension (MAP < 70 mmHg), and any type of hemorrhagic complication[3]. The primary endpoints were 28-d mortality and changes in hemodynamic parameters such as VDI and inotropic score within the first 3 d. The secondary endpoint was the 7-day mortality and the variation in the SOFA score within the first 3 d[4,16].
Statistical analysis
SPSS for Windows (version 21.0, SPSS Inc., Chicago, IL, United States) was used for statistical analysis. ThePvalue of less than 0.05 was considered statistically significant. Continuous variables were analyzed using Student'st-test and expressed as the mean standard deviation. Categorical variables were presented as proportions,and were analyzedvia χ2test or Fisher's exact test. The variations in SOFA score were analyzed using Wilcoxon rank sum test. We used propensity-score matching in order to minimize the lead-time bias and selection bias. Propensity-score matching was conducted to adjust for confounding of baseline characteristics and the severity of clinical conditions. To estimate the propensity score, a logistic regression analysis of clinical factors including age, sex, body weight, underlying malignancy, APACHE II score, pre-existing organ dysfunction, initial SOFA score, microorganism responsible for sepsis, and the initial values of lab including the count of WBC, platelet count,hemoglobin and the level of prothrombin time or international normalized ratio, was performed in patients who underwent PMX-HP treatment. In the propensity scorematched population, we compared the continuous variables using a pairedttest or the Wilcoxon rank test and categorical variables with the McNemar's or Bowker's test in the same group. Also one-way ANOVA was used to compare two groups. The Cstatistics were estimated to evaluate the goodness of fit. We used 1:1 matching and a caliper width equal to 0.01 of the standard deviation of the logit of the propensity score was used.
RESULTS
A total of 308 eligible patients including the PMX group (n= 20) and control group (n= 288) were finally enrolled, and 20 propensity-score-matched pairs were generated.Figure 2 demonstrates the study profile. Table 1 presents a comparative analysis of the baseline characteristics of the PMX and the control groups after propensity-score matching. Patient characteristics were adequately balanced between the two groups after propensity-score matching in terms of mean age, gender, underlying malignancy, pre-existing organ dysfunction, use of vasoactive agents and disease severity. Table 2 presents a comparative analysis of etiology and treatment for sepsis between the two groups. The leading primary infection site was lower gastrointestinal tract in both groups. (14 cases, 70.0% in PMX groupvs10 cases, 50% in control group,P= 0.166) Microbiological evidence of infection was confirmed in 28 (70.0%) patients,based on the bacterial cultures obtained before the operation or intervention. Multiple microorganisms were isolated in 12 (30.0%) patients. Gram-negative species were the predominant pathogen isolated in both groups (11 cases, 55.0% in PMX groupvs10 cases, 50% in control group,P= 0.752). The majority of patients (95.0%) received surgical treatment, and two patients underwent radiological intervention such as percutaneous trans-hepatic gallbladder drainage. There was no significant difference in the proportion of patients receiving CRRT or mechanical ventilation in both groups, and both groups had comparable clinical and laboratory parameters as described in Table 2.
Regarding the clinical effects of PMX-HP, there was a significant improvement in the SOFA score at 72 h in patients included in the PMX-HP group compared with the control group (from 11.2 ± 5.8 to 4.7 ± 3.5 in PMX groupvs10.0 ± 4.0 to 8.7 ± 7.3 in control group,P= 0.047). Especially, the renal and coagulation SOFA scores were significantly improved in PMX group (from 2.6 ± 1.0 to 0.7 ± 1.0 in PMX groupvs2.6 ±1.5 to 2.8 ± 1.6 in control group,P =0.000, from 1.6 ± 1.5 to 1.3 ± 1.3 in PMX groupvs1.2 ± 1.2 to 2.8 ± 1.8 in control group,P= 0.014, respectively). Furthermore, the inotropic score and VDI were significantly decreased in PMX group (from 163.7 ±302.1 to 8.9 ± 19.1 of inotropic score in PMX groupvs90.8 ± 181.7 to 1.4 ± 4.2 in control group,P =0.006, and from 2.4 ± 3.4 to 0.1 ± 0.3 of VDI in PMX groupvs1.0 ± 2.0 to 0.0± 0.1 in control group,P= 0.001, respectively) (Table 3). The PMX group showed a greater reduction compared to the control group in terms of renal SOFA (mean delta SOFA score, -1.9vs0,P= 0.007) and coagulation SOFA (mean delta SOFA score, -0.36vs1.93,P= 0.013). However, the two groups were similar in term of total SOFA (mean delta SOFA score, -6.13vs-1.28,P= 0.121), cardiovascular SOFA (mean delta SOFA score, -2.12vs-1.43,P= 0.315) respiratory SOFA (mean delta SOFA score,-1.0vs-0.65,P= 0.613) (Figure 3). The length of ICU stay was significantly shorter in the PMX group than the control group (10.9 ± 3.9 d in PMX groupvs14.6 ± 6.4 d in control group,P =0.036). The ICU mortality rate was lower in the PMX group (n= 4, 20%)than in the control group (n= 8, 40%) without any statistically significant difference.Similarly, there was no significant difference between the two groups in the inhospital mortality and duration of mechanical ventilation (Table 4).
DISCUSSION
In the current study, PMX-HP treatment significantly improved the hemodynamic parameters such as inotropic score and VDI, and the degree of organ failure represented by the renal, coagulation or total SOFA score, and the length of ICU stay,for patients whose infection focus were successfully removed by surgical intervention.
In terms of hemodynamic aspects, the inotropic score and VDI decreased significantly in the PMX group consistent with previous studies that showed a significantly increment in arterial pressure and decreased need for vasopressor after PMX-HP treatment[4,14]. PMX is a lipopeptide antibiotics isolated fromBacillus polymyxa. It disrupts the outer membrane of GNB and binds to the lipid A portion of LPS selectively[19]. Circulating LPS activates the inflammatory reaction, complement or coagulation system of the hosts. Nakamuraet al[22,23]. reported that circulating monocyte and neutrophils were removed through the PMX cartridge, and PMX-HP reduced the levels of TNF-α, IL-6, IL-10, plasminogen activator inhibitor 1,metalloproteinase and anandamide. These mechanisms of PMX-HP improved tissue oxygenation and hemodynamic status, and contributed to the improvement of hemodynamics in patients with abdominal septic shock.
Moreover, PMX-HP treatment improved the cardiac functionviaelimination of myocardial depressant mediator such as anandamide of 2-arachidonoylglycerol.Therefore, it reduces the dosage of catecholamine drugs and enhances the hemodynamic outcome[24]. We propose that this mechanism decreases the adverse cardiovascular effects of high-dose catecholamines such as arrhythmia, decreased cardiac output, ischemic change of mesentery caused by potent vasoconstriction.Maynaret al[14]. reported that 28-d mortality rates were significantly decreased inpatients who reduced their norepinephrine dose by more than half within 24 h after PMX-HP. Our study also revealed a significant improvement in the inotropic score and VDI of the PMX group and suggested that PMX-HP treatment in reduced the levels of myocardial depressant mediator in cardiac function.
The role of PMX-HP in septic shock would also affect the pulmonary function by absorbing various inflammatory mediators including endotoxins and proinflammatory cytokines. The improvement in hypercytokinemia and inflammation prevented the damage to pulmonary endothelium consequently[1,25,26]. Pulmonary complications are common in septic shock, and rapidly increased due to fluid resuscitation or compromised respiratory function triggered by anesthesia after major surgery, and therefore PMX-HP might improve and protect pulmonary functions in patients after emergency abdominal surgery who has high risk of pulmonary complications such as acute respiratory distress syndrome[27]. However, we failed to detect a statistically significant improvement in pulmonary function probably due to its small sample size, and a further study with a large sample size should be needed.
In addition, one of the most common complications of septic shock is acute kidney injury (AKI) and it occurs in more than 20% of patients with sepsis that is related to higher mortality rate[28]. Ebiharaet al[29]suggested that PMX-HP restored the angiopoietin-1 levels and diminished the levels of angiopoietin-2 in septic AKI,thereby preventing the apoptosis of renal tubular cells resulting in a protective effect against AKI[19]. Our results demonstrated a dramatic decrease in renal SOFA score,and considering the high mortality of septic AKI, authors expect that the removal of endotoxin or cytokines might protect the renal function in abdominal septic shock.Our study also showed a significant reduction in the length of ICU stay and SOFA score at 72 h indicating improvement in overall organ function. PMX-HP therapy may have improved the prognosis in the early phases of intraabdominal septic shock and promoted organ preservation, ultimately.
Despite these interesting results of the PMX-HP, our study has some limitations inherent to its retrospective design and small sample size. Since it covers a period of more than six years, the evolution of intensive care may have affected the survival.However, a single intensivist performed the treatment according to the standard protocol, and no major changes in SSC guidelines have occurred. In addition, we could not exclude the impact of renal replacement therapy such as CRRT for clinical outcomes. For next study, we will fully consider this limitation and we will perform additional subgroup analysis on modified SOFA scores to completely exclude the impact of renal replacement therapy such as CRRT for clinical outcomes. In fact, in order to overcome these limitations, we performed a propensity score matching tocorrect for disease severity and baseline characteristics. Moreover, we believe that the bias might be minimized because the PMX-HP treatment was indicated to only patients with abdominal sepsis who underwent source control for the infectious foci.Additionally, the detection of further statistically significant differences in parameters such as 28-d mortality or ICU mortality was precluded due to the small sample size. A prospective multicenter randomized trial with a large sample size is needed in the near future to confirm our study results.
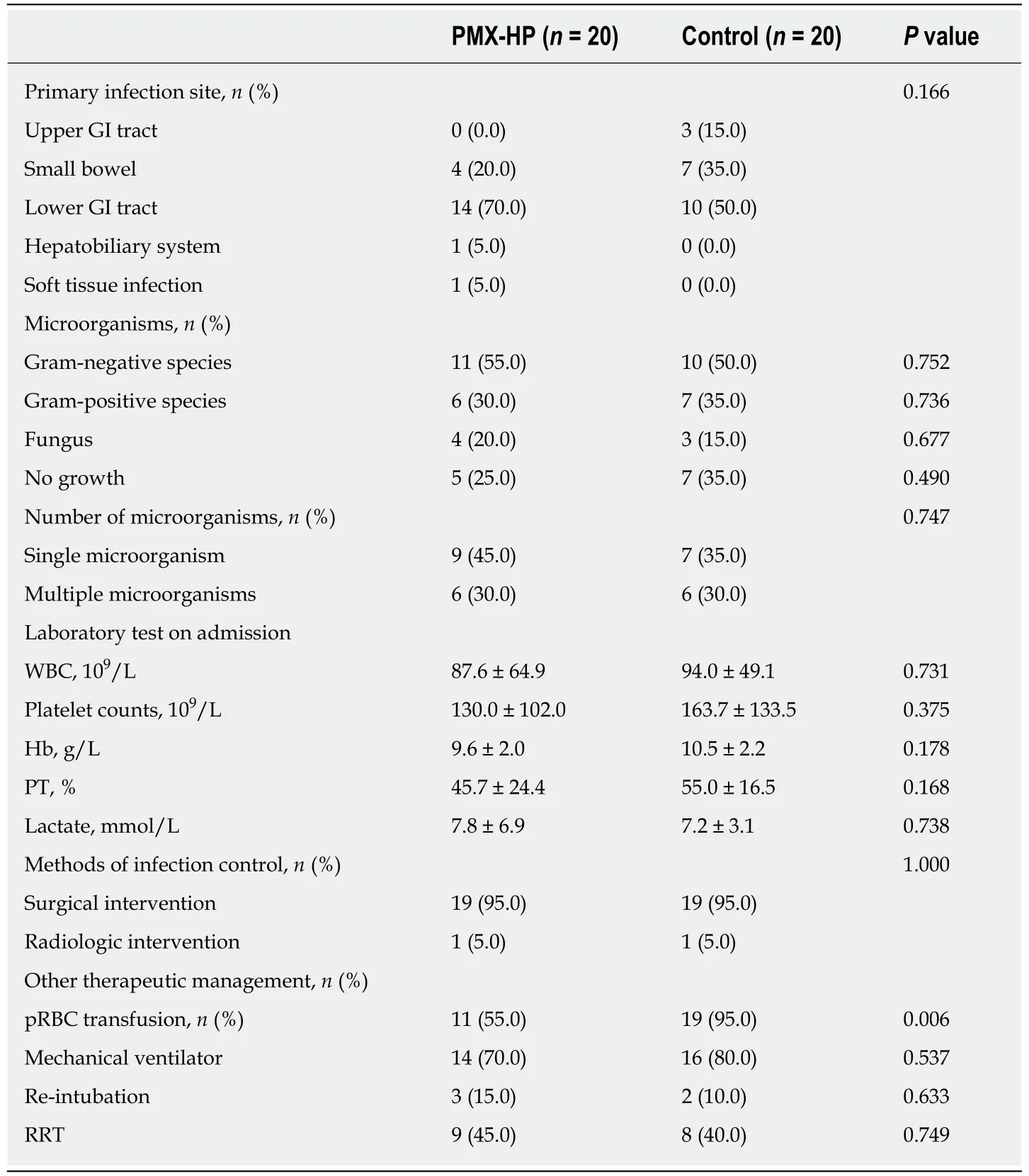
Table 2 Characteristics of patients, laboratory findings, and treatment of sepsis in propensitymatched groups
Actually, there have been studies to identify the effect of PMX-HP in various randomized controlled trials in the meantime. In the EUPHAS I trial of 2009[4], PMXHP significantly reduced the 28-d mortality and improved SOFA score in patients with septic shock associated with gram-negative infeciton. In the EUPHAS 2 trial of 2014, there was a significant decrease in SOFA score in patients with only abdominal sepsis[13]. We agree that PMX-HP is more effective in patients with abdominal sepsis following surgical elimination of infection foci. In case of other gram-negative infections, such as infection of the lower respiratory tract, the control of infectious source should be accomplishedviausing antibiotics, and this limitation might be implicated in a resistance to antibiotics or drug toxicity. On the other hand, in patients with abdominal sepsis, PMX-HP may be used after complete elimination of infection focusviasurgical control, resulting in clearance of the residual circulating endotoxin more effectively compared with other sites of infection[7]. We expect that this study,which involved only patients with abdominal sepsis controlled surgically, would be useful in establishing treatment guidelines for PMX-HP intervention.

Figure 2 Outline of patient selection and propensity score matching.
In conclusion, PMX-HP would be a feasible treatment modality in ICU patients with peritonitis to restore organ function and improve hemodynamics. It is expected to facilitate clinical outcomes especially in patients with complete elimination of the source of GNB infectionviasurgical procedures. A further prospective study with large samples is needed to establish the precise guidelines for PMX-HP therapy.
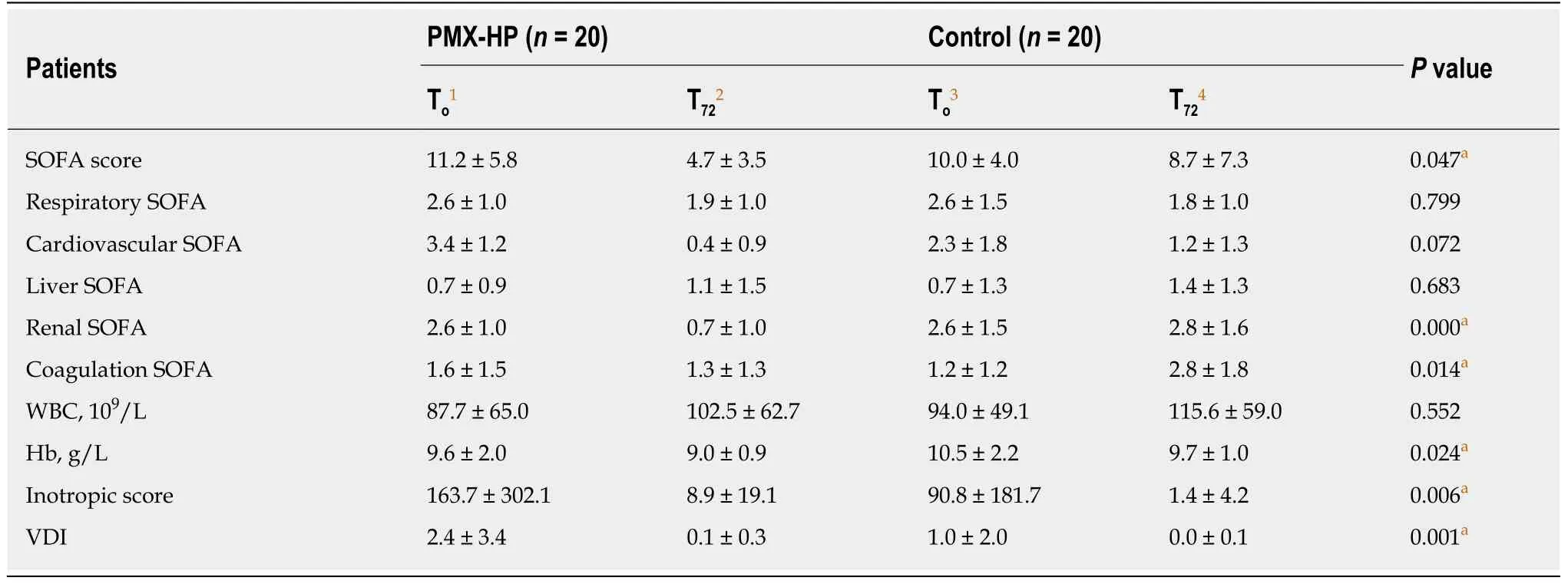
Table 3 Comparative analysis of variables changes between baseline and 72 h after treatment

Table 4 Mortality, length of Intensive care unit stay and ventilator free days in polymyxin B hemoperfusion and control groups

Figure 3 Comparison of the Sequential Organ Failure Assessment score at 72 h between polymyxin B hemoperfusion and control groups.
ARTICLE HIGHLIGHTS
Research background
Polymyxin B hemoperfusion (PMX-HP) has been used as a treatment for intra-abdominal septic shock by absorbing and removing endotoxins of gram-negative bacilli.
Research motivation
Intra-abdominal infection is one of the common causes of septic shock and is associated with a high mortality rate despite the treatment under survival sepsis guidelines. Previous studies demonstrate the favorable results of extracorporeal removal of endotoxin.
Research objectives
The objectives of this study is to investigate the clinical efficacy of PMX-HP in patients with gram-negative septic shock who underwent abdominal surgery.
Research methodes
From January 2012 to December 2018, patients who had septic shock secondary to peritonitis were enrolled. They were classified into PMX-HP treated and control groups based on postopreative intervention using PMX-HP. The clinical outcomes were compared using 1:1 propensity score matching methods to balance the overall distribution between the two groups.
Research results
After propensity score matching, 40 patients were analyzed (20 patients in the PMX group and 20 patients in the control group). The scores of total Sequential Organ Failure Assessment(SOFA) score, renal SOFA and coagulation SOFA were significantly improved in the PMX group but not in the control group. (from 11.2 ± 5.8 to 4.7 ± 3.5 in PMX groupvs10.0 ± 4.0 to 8.7 ± 7.3 in control group,P= 0.047 from 2.6 ± 1.0 to 0.7 ± 1.0 in PMX groupvs2.6 ± 1.5 to 2.8 ± 1.6 in control group,P =0.000, from 1.6 ± 1.5 to 1.3 ± 1.3 in PMX groupvs1.2 ± 1.2 to 2.8 ± 1.8 in control group,P= 0.014, respectively). Further, the length of intensive care unit (ICU) stay was significantly shorter in PMX group. However, no statistically significant difference was found in ICU mortality.
Research conclusions
PMX-HP is a feasible adjunct treatment for peritonitis in ICU patients with peritonitis for improved organ impairment and to stabilize hemodynamics. It would be helpful to enhance clinical outcomes especially in patients with complete elimination of the source of gram-negative bacilli infection by surgical procedure accompanied with conventional treatment of sepsis.
Research perspectives
Our study is limited by its retrospective nature and small sample size. Also, since it covers a period of more than six years, the evolution of intensive care may have affected the survival.Further studies especially prospective multicenter randomized trial with a large sample size should be conducted to confirm our study results.
