Self-efficacy for managing hypertension and comorbid conditions
2019-12-23MiJungLeeSergioRomeroHuanGuangJiaCraigVelozoAnnGruberBaldiniLisaShulman
Mi Jung Lee,Sergio Romero,HuanGuang Jia,Craig A Velozo,Ann L Gruber-Baldini,Lisa M Shulman
Mi Jung Lee,Sergio Romero,Department of Occupational Therapy,University of Florida,Gainesville,FL 32610,United States
Mi Jung Lee,Sergio Romero,Huan-Guang Jia,NF/SG VHS,Center of Innovation on Disability and Rehabilitation Research-GNV,Gainesville,FL 32601,United States
Craig A Velozo,Division of Occupational Therapy,Medical University of South Carolina,Charleston,SC 29425,United States
Ann L Gruber-Baldini,Department of Epidemiology and Public Health,University of Maryland School of Medicine,Baltimore,MD 21201,United States
Lisa M Shulman,Department of Neurology,University of Maryland School of Medicine,Baltimore,MD 21201,United States
Abstract
Key words: Hypertension;Self-efficacy;Self-management;Chronic conditions
INTRODUCTION
Chronic conditions,such as hypertension,require consistent symptom management and treatment adherence.However,according to the Centers for Disease Control and Prevention,approximately 24% of adults with hypertension do not engage in self-care practices (i.e.,takes medications) to control their blood pressure.Farley et alreported that for each 10% increase in adherence to hypertension treatment,14000 adult lives could be saved annually in the United States.Adherence to self-managing treatment behaviors has been associated with age,gender,marital status,emotional well-being,knowledge of hypertension medication and management,and selfefficacy.Among these variables,self-efficacy has been a critical predictor or mediator of adherence to treatment behaviors for hypertension and other chronic conditions.
Self-efficacy is defined as an individual’s belief in performing a required course of actions to accomplish a given outcome.Self-efficacy is a consistent predictor of behavioral maintenance and was shown to improve with health educational programs.Studies show that self-efficacy is a determinant of participation in selfmanagement of hypertension.In addition,in a study of individuals with hypertension conducted by Schoenthaler et al,the negative influence of depression on medication adherence was mediated by self-efficacy,such that when self-efficacy was controlled,the relationship between depression and medication adherence became nonsignificant.Therefore,enhancing self-efficacy for managing hypertension is important to foster self-management of hypertension.
Hypertension is associated with many medical comorbidities (e.g.,cerebrovascular disease,cardiovascular diseases).Therefore,patients with hypertension often manage multiple comorbid conditions.Accordingly,when examining self-efficacy for managing hypertension,the overall aspect of self-efficacy for managing chronic conditions should be considered beyond hypertension management.The patient reported outcomes measurement information system self-efficacy for managing chronic conditions measures (PROMIS-SE) are the non-disease-specific and domainspecific self-efficacy measure for managing chronic conditions therefore might be most appropriate for capturing the multidimensional aspects of self-efficacy for managing chronic conditions in patients with hypertension who often need to manage multiple chronic conditions.PROMIS-SE includes a total of 137 items in five selfefficacy domains.These domains are self-efficacy for managing daily activities,emotions,medications and treatments,social interactions,and symptoms.
Thus,the purpose of this study is to investigate self-efficacy for managing chronic conditions in individuals with hypertension.The study aims are to compare domainand item-level self-efficacy for managing chronic conditions between patients with hypertension and patients with other chronic conditions;and identify structural relationships between self-efficacy for managing hypertension and comorbid conditions and other health-related outcomes.
MATERIALS AND METHODS
This retrospective study was a secondary analysis of data from the PROMIS-SE original validation study.The dataset includes patients from a clinical practice at the University of Maryland Neurology Care Center (patients with neurologic conditions) and individuals from a national online recruitment company,Op4G(patients with general chronic medical conditions) from April 2013 to April 2014.Data was collected from a total of 1087 patients with chronic conditions,with 837 patients comprising the neurology sample.For the online sample,250 subjects were randomly selected among approximately 250000 identified subjects with chronic conditions in the Op4G database.Participants were asked to respond to PROMIS-SE items based on all chronic conditions they experience.For the purpose of this study,participants were divided into two groups,hypertension and non-hypertension,based on selfreport.
Inclusion criteria for the study sample were: (1) 18 years of age or older;(2)Community residence;and (3) Having at least one common chronic condition such as arthritis,depression,coronary artery disease,heart attack,stroke,and other conditions (Table 1).At the University of Maryland Neurology Care Center,participants were diagnosed with one of the following chronic neurologic conditions:epilepsy,multiple sclerosis,Parkinson’s disease,peripheral neuropathy,and stroke.For additional data collections methods and procedures,please see Hong et aland Gruber-Baldini et al.
This study was approved by the institutional review boards of the Medical University of South Carolina (#Pro00033397),the University of Florida (#261-2010),and the University of Maryland (#HP- 000432550).
PROMIS-SE
The PROMIS-SE measure comprise a total of 137 items from five domain item banks;daily activities (DA;35 items),emotions (EM;25 items),medications and treatments(MT;26 items),social interactions (SS;23 items),and symptoms (SX;28 items).The 5-point Likert scale for all items was: (1) Not at all confident;(2) A little confident;(3)Somewhat confident;(4) Quite confident;and (5) Very confident.Appendix provides all of the items in the PROMIS-SE.Participants’ PROMIS-SE domain scores were calculated separately for each domain using the graded response model from item response Theory.Patient scores are provided in T-scores (a mean of 50 with a standard deviation of 10) based on the distribution of the US clinical sample with chronic conditions.These T-scores are described as Tscores.Detailed information on PROMIS-SE’s psychometric data and its scoring system,is provided in our previous publications.
PROMIS global health measure
The PROMIS Global Health measure consists of ten items that are designed to assess global physical,mental,and social health of generic,rather than disease-specific populations.For this study,we used scores for the global physical v1.0 (Item Global 03: “In general,how would you rate your physical health?”,item Global 06: “To what extent are you able to carry out your everyday physical activities such as walking,climbing stairs,carrying groceries,or moving a chair?”,item Global 07: “How would you rate your pain on average?”,and item Global 08: “How would you rate your fatigue on average?”) and mental health v1.2a (Item Global 04: “In general,how would you rate your mental health,including your mood and your ability to think?”and item Global 05: “In general,how would you rate your satisfaction with yoursocial activities and relationships?”).A single item,“In general,would you say your quality of life is…” was used to assess general quality of life.The rating scale for this item was: Excellent,very good,good,fair or poor.

Table1 Patient-reported chronic conditions,n (%)
Statistical analysis
Participants were divided into two groups (hypertension and non-hypertension).These two groups’ self-efficacy for managing chronic conditions were compared at the domain- and item-levels.At the domain level,we compared the average Tscores across the five PROMIS-SE domains between the two groups.Higher Tscores represent higher self-efficacy levels for any given domain.At the item level,based on the two groups’ average ratings for all 137 items,items with a large difference between the two groups were identified.Multivariate analysis of variance(MANOVA) was conducted to test for statistical differences in self-efficacy for managing chronic conditions between individuals with hypertension and without hypertension.When MANOVA results were significantly different,univariate analysis of variance (ANOVA) was conducted for each domain to examine the main effect.We randomly selected 300 individuals for each group (n = 600 total) in order to prevent disproportionate numbers between the groups.
In addition,structural equation modeling was conducted to examine the relationships between self-efficacy and other health-related outcomes,such as global physical health,global mental health,and general quality of life for the hypertension group using PROMIS global health measure.Since previous studies have shown these five domains are correlated,we allowed the domains to be correlated in the model.Maximum likelihood estimation with robust standard errors (MLR) was used as the estimator to calculate coefficients.The three health-related outcomes were regressed on those five PROMIS-SE domains simultaneously using 80% of randomly selected data (full model,Figure 1).Then,we excluded the non-significant predictors and retested fitness of the model with the remaining 20% of our data (unused) and confirmed the structural model of self-efficacy on other health-related outcomes.In order to assess the fit,the following criteria were used: CFI and TLI (> 0.95 good,>0.90 acceptable),RMSEA (< 0.06 good,< 0.08 acceptable),and SRMR (< 0.05 good,<0.08 acceptable).Statistical programs R 3.5.0,R studio version 1.0.136 (R Core Team,Cary,Vienna,Austria),and various packages (dplyr,tidyr,splitstackshape,lavaan,and semPlot) were used for all computational processes.
RESULTS
Among 1087 participants,437 reported having hypertension (617: Non-hypertension and 33: Missing).The hypertension group (M = 57.8,SD = 12.5) were significantly older than the non-hypertension groups (M = 50.7,SD = 15.3);t (1036) = -7.8,P <0.001.Also,individuals with hypertension (M = 5.2,SD = 2.5) had significantly more comorbid conditions (5.2: Including hypertension and 4.2: excluding hypertension) as compared to individuals with no hypertension (M = 2.9,SD = 2.0) on average;t (1052)= -16.7,P < 0.001.The most common comorbid chronic conditions for individuals with hypertension were arthritis or rheumatism (202,46%),depression (160,37%),neuropathy (142,32%),anxiety (141,32%),and diabetes (138,32%),whereas depression (197,32%),anxiety (172,28%),migraines or severe headaches (163,26%),arthritis or rheumatism (160,26%),and epilepsy (128,21%) were most common for individuals without hypertension.As expected,risk factors associated with hypertension were more prominent in hypertension groups (i.e.,angina,coronary artery disease,myocardial infarction,stroke,heart failure).In addition,the two groups were statistically significantly different in education [χ(1,N = 1052) = 5.4,P <0.05] and in employment status [χ(1,N = 1054) = 7.1,P < 0.01].For detailed information on comorbid conditions and demographics of two groups,please see Tables 1 and 2.
Comparing hypertension and non-hypertension groups
Average Tscores for each domain of PROMIS-SE for hypertension and nonhypertension groups ranged from 49.2 to 50.4 and 49.6 to 51.1 (Table 3),respectively.As compared to the non-hypertension group,the hypertension group had lower average Tscores in DA (-1.9),MT (-0.4),and SX (-0.1) and higher average Tscores in EM (+0.7) and SS (+0.4).Accordingly,among the top fifteen PROMIS-SE items with the most substantial differences between the two groups (higher for the nonhypertension group),thirteen items belonged to DA.Item DA13 (exercise vigorously for 10 min) showed the largest difference (0.68) between the hypertension and nonhypertension groups.DA17 (climb one flight of stairs) had the second largest difference (0.32) and DA12 (exercise moderately for 10 min) came in third (0.31).On the other hand,the hypertension group’s average ratings were higher for all items in EM except for EM03 (relax body to reduce anxiety;0.05;Supplementary 1).
A one-way MANOVA identified a statistically significant difference in self-efficacy between hypertension and non-hypertension groups [Wilks’ λ = .973,F (5,594) =3.261,P < 0.001].According to the follow-up univariate ANOVAs for each domain of the PROMIS-SE,significant univariate main effects for the hypertension group were obtained for DA [F (1,598) = 5.63,P < 0.05],but not for all other domains;EM [F (1,598) = 1.17,P = 0.28],MT [F (1,598) = 0.24,P = 0.62],SS [F (1,598) = 0.13,P = 0.72],and SX [F (1,598) = 0.09,P = 0.76].
Structural relationship between self-efficacy and other health-related outcomes
Our full model explained 59.8%,60.6%,and 46.5% of the variance in general quality of life,global physical health,and global mental health sequentially.Four out of five PROMIS-SE domains significantly predicted global physical health (DA: P < 0.001,EM: P < 0.05,MT: P < 0.001,SS: P = 0.304,and SX: P < 0.001).For global mental health,three PROMIS-SE domains were significant predictors (DA: P < 0.001,EM: P < 0.001,MT: P = 0.128,SS: P < 0.01,and SX: P = 0.526).General quality of life was significantly predicted by both global physical health (P < 0.001) and global mental health (P <0.001),but none of the five PROMIS-SE domains significantly directly predicted general quality of life (DA: P = 0.818,EM: P = 0.388,MT: P = 0.342,SS: P = 0.224,and SX: P = 0.770).Following the results of the full model,the five PROMIS-SE domains as direct predictors of general quality of life,SS as a direct predictor of global physical health,and MT and SS as direct predictors of global mental health were removed in the revised model.The full model was “just” identified;CFI (1),TLI (1),RMSEA (0),and SRMR (0),respectively.
In this revised model,we tested the effect of self-efficacy on general quality of life with global physical health and mental health fully mediating (indirect effect only)this relationship with the unused sample (Figure 2).Our revised model demonstrated excellent fit to our data;CFI (0.997,> 0.95 good),TLI (0.990,> 0.95 good),RMSEA(0.044,< 0.06 good),and SRMR (0.015,< 0.05 good) respectively.The revised model explained 55.5 %,50.5 %,and 54.5 % of the variance in general quality of life,global physical health,and global mental health,consecutively.Global physical health and mental health significantly predicted general quality of life (P < 0.001).It was noted that two PROMIS-SE domains (DA: P < 0.001 and EM: P < 0.01) significantly predicted global physical health (DA: P < 0.001) and one domain (EM: P < 0.001)predicted global mental health.Figure 2 and Table 4 provide the structure of the revised model and its corresponding statistical results.

Figure1 The full model.
DISCUSSION
According to the World Health Organizations’ report on chronic condition care,patients with hypertension have poor self-management skills,including managing prescribed medications.The report recommends the study of hypertension selfmanagement skills to effectively control this life-long disease.Among factors contributing to managing hypertension,self-efficacy is a significant component in adherence to self-management activities.This study investigated self-efficacy domains for managing chronic conditions in individuals with hypertension and other comorbid conditions.Our results show that,compared to individuals with other chronic conditions,those with hypertension have significantly lower levels of selfefficacy for managing daily activities (DA),while their self-efficacy levels for managing emotions (EM),medications and treatment (MT),social interaction (SS) and symptoms (SX) were similar to our reference group of individuals with chronic conditions.Further,we found that self-efficacy is an indirect predictor of general quality of life in participants with hypertension and a direct predictor for their global physical and mental health.
Confidence in managing daily activities can be affected in individuals with decreased mobility and overall physical function.In our study,demographic differences between groups could account for the differences found in this domain.The hypertension group was on average seven-years-older and had approximately two more chronic conditions than the reference clinical sample.Aging is significantly associated with decreased physical abilities,abilities to perform daily tasks independently,and disability.Having more chronic conditions is likely to result in lower physical function.It has been estimated that approximately 25% of persons with chronic conditions have some physical limitations and that physical disability increases with increasing numbers of coexisting chronic conditions.Also,known risk factors for the development of hypertension,including obesity,physically inactivity,unhealthy diet,and alcohol/tobacco consumptionare associated with poor physical function and can potentially influence individuals’ beliefs in their capacity to perform daily tasks.
Other self-efficacy domains assessed by PROMIS-SE (managing emotions,medications and treatment,social interaction and symptoms) were equally affected across the hypertension and non-hypertension groups.In our previous paper,we did not find statistical differences among five chronic neurologic conditions in three PROMIS-SE domains;managing emotions,medications and treatment,and social interaction.These suggests individuals with chronic conditions have similar perceptions of their abilities to manage their conditions.Since our groups had different types and number of chronic conditions,we were not able to examine the unique impact of hypertension on self-efficacy for disease management.Furtherstudies are needed to see if differences exist that can potentially result in targeted interventions.

Table2 Demographics,n (%)
Our study indicates that self-efficacy for managing hypertension and comorbid conditions has an indirect effect on the general quality of life of these individuals.More than half of the variance in global physical and mental health is predicted by two domains of PROMIS-SE (managing daily activities and emotions) and one domain (managing emotions) sequentially,and global physical and mental health directly predict the general quality of life for patients with hypertension.This result supports that two domains of self-efficacy for managing chronic conditions (DA and EM) play a substantial role in the general quality of life of individuals with hypertension.Improving self-efficacy for managing chronic conditions has been recommended in patients with chronic pain for reducing disability,patients with epilepsy for improving general quality of life,patients with chronic kidney disease for encouraging self-care,and patients with spinal cord injury for reducing depressive conditions.The hypertension literature has focused on the role of selfefficacy for managing medication adherence.Based on our results,further studies are needed to isolate the specific role of self-efficacy for managing daily activities and emotions in this population in order to develop domain-specific interventions that maximize quality of life.
As with any retrospective analysis,this study relied on existing data,not collected to address our research questions.Critical variables such as length and severity of each chronic condition that could influence our study result were not included in our study.Further,we relied on a single item to represent general quality of life.Though the literature supports single item scales to assess quality of life,we acknowledge important limitations when assessing such a complex construct with a single item.Many aspects of quality of life including life trajectories,goals,expectations,disease dependency,and culture need to be considered since they influence individuals’perception of their quality of life.These are difficult to capture with a single item.Other studies have found self-efficacy to be a direct predictor of health-related quality of life.Our study indicates an indirect relationship between self-efficacy domains and the broader perception of quality of life.Further investigation is needed to elucidate the relationship between self-efficacy domains and health-related quality of life in individuals with hypertension.
While we attempted to minimize group selection bias,we found significant differences in age,number of chronic conditions,and other demographic variables that could influence our results.Future studies are needed to investigate the uniqueimpact of hypertension on the perceived ability of individuals to manage the condition.
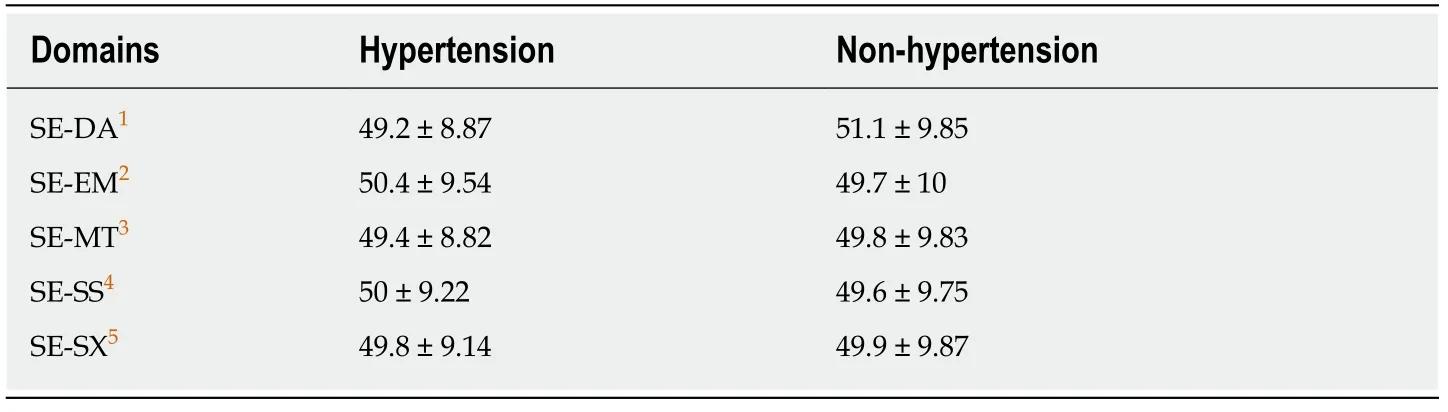
Table3 Average Tclin scores in patient reported outcomes measurement information system self-efficacy for managing chronic conditions measures domains (mean ± SD)
In conclusion,individuals with hypertension report deficits in self-efficacy to manage their condition and other comorbidities.This was particularly true for selfefficacy in managing daily activities.In this hypertension group,self-efficacy functioned as an indirect factor,mediated by global physical and mental health,to predict general quality of life.
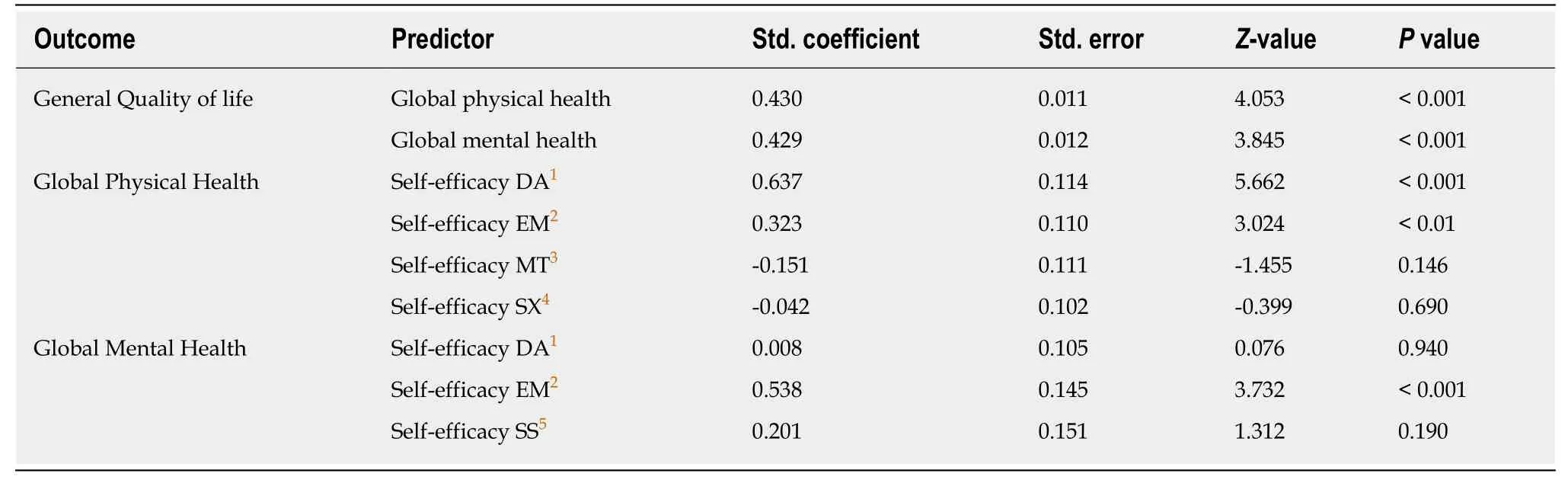
Table4 Parameters of the revised model

Figure2 The revised model.
ARTICLE HIGHLIGHTS
Research background
Consistent symptom management and treatment adherence are necessary for managing chronic conditions.Self-efficacy has been an influential predictor and mediator of adherence to treatment behaviors for patients with chronic conditions,such as hypertension.Patients with hypertension often manage multiple comorbid conditions since hypertension is often associated with numerous other medical conditions (e.g.,cerebrovascular disease,cardiovascular diseases).However,self-efficacy for managing hypertension and comorbid conditions has not been thoroughly examined.
Research motivation
Effectively improving self-efficacy for managing hypertension and comorbid conditions is critical for self-management of hypertension.Investigating self-efficacy for managing hypertension and comorbid conditions and its relationships to other health-related outcomes will allow clinicians and researchers to design therapeutic interventions tailored to patients with hypertension.Further,differences in self-efficacy domains and items may help develop targeted interventions to improve self-efficacy in this patient population.
Research objectives
Objectives of this study are to examine self-efficacy for managing chronic conditions in patients with hypertension and compare it to patients with other chronic conditions.We identified the structural model explaining the relationship of self-efficacy for managing hypertension with other health-related outcomes at the domain level.
Research methods
A total of 1087 individuals with chronic conditions were selected in this study.Individuals with chronic conditions were grouped into hypertension and non-hypertension group.Differences in self-efficacy for managing chronic conditions between the two groups were examined at domainand item-level using five domains of patient-reported outcomes measurement information system self-efficacy for managing chronic conditions measures (PROMIS-SE).Also,the associations between five domains of PROMIS-SE and other health-related outcomes such as global physical health,global mental health,and general quality of life were investigated using structural equation modeling for the hypertension group.
Research results
A total of 437 reported having hypertension (617: non-hypertension and 33: missing).Statistical differences in self-efficacy for managing chronic conditions between hypertension and nonhypertension groups were identified in the self-efficacy for managing daily activities domain.Also,for hypertension patients,self-efficacy for managing daily activities and emotions were significant predictors of global physical health.For global mental health,only one domain,selfefficacy for managing emotions was a significant predictor.Overall,both global physical and mental health statistically significantly predicted hypertension patients’ general quality of life.
Research conclusions
The hypertension group had lower self-efficacy for managing daily activities as compared to the non-hypertension group.For individuals with hypertension,self-efficacy for managing daily activities and emotions were indirect predictors for their general quality of life,mediated by global physical and mental health.
Research perspectives
Future studies are encouraged to examine specific roles of these two domains of self-efficacy for managing hypertension and comorbid conditions on global physical and mental health,and general quality of life in order to provide domain specific interventions that effectively enhance those outcomes.
