Gastric food retention at endoscopy is associated with severity of liver cirrhosis
2019-12-02DavidSnellShirleyCohenMekelburgRussellWegGauravGhoshAdamBuckholzAmitMehtaXiaoyueMaPaulChristosArunJesudian
David B Snell,Shirley Cohen-Mekelburg,Russell Weg,Gaurav Ghosh,Adam P Buckholz,Amit Mehta,Xiaoyue Ma,Paul J Christos,Arun B Jesudian
David B Snell,Division of Gastroenterology and Hepatology,New York University,New York,NY 10016,United States
Shirley Cohen-Mekelburg,Division of Gastroenterology and Hepatology,University of Michigan,Ann Arbor,MI 48109,United States
Russell Weg,Division of Gastroenterology and Hepatology,University of Rochester Medical Center,Rochester,NY 14642,United States
Gaurav Ghosh,Adam P Buckholz,Department of Medicine,NewYork-Presbyterian Hospital/Weill Cornell Medicine,New York,NY 10065,United States
Amit Mehta,Arun B Jesudian,Division of Gastroenterology&Hepatology,Weill Cornell Medicine,New York,NY 10021,United States
Xiaoyue Ma,Paul J Christos,Division of Biostatistics and Epidemiology,Department of Healthcare Policy and Research,Weill Cornell Medicine,New York,NY 10065,United States
Abstract
Key words:Child-Pugh;Cirrhosis;Endoscopy;Gastric emptying;Motility
INTRODUCTION
Many patients with cirrhosis report gastrointestinal(GI)symptoms such as abdominal bloating,pain,and belching[1-6].The prevalence of these symptoms has prompted investigation into abnormalities in GI function in cirrhosis.As suspected,cirrhotic patients have higher rates of gastrointestinal dysmotility,characterized by delayed gastric emptying and prolonged small bowel transit time,compared to those without cirrhosis[1,2,7-19].While severity of cirrhosis has been associated with worsened small bowel motility,the relationship between gastric emptying and severity of liver disease has not been well established.Although some studies have correlated markers of portal hypertension with delayed gastric emptying[7,9,14,20],those examining the size of esophageal varices[11],variceal pressure[16],and hepatic venous pressure gradient[21],have failed to demonstrate an association with impaired gastric motility.
The presence of retained gastric food on esophagogastroduodenoscopy(EGD)can be used as a surrogate for delayed gastric emptying with a reasonably high specificity[22].Furthermore,the risk of retained gastric food contents at EGD is higher among patients with severe emptying delays compared to mild or moderate delays[22].Using this method of evaluating for retained food at EGD,the prevalence of delayed gastric emptying is less than 1% in the general population[23].
Since patients with cirrhosis frequently require EGD for surveillance and treatment of esophageal varices,evaluation for retained gastric food contents at EGD could provide important clinical information in this population.Therefore,we conducted this study to characterize the frequency of retained gastric food contents at EGD in a cirrhotic population compared to a control population without liver disease and to elucidate factors predictive of retained food.
MATERIALS AND METHODS
We performed a retrospective case-control study of patients with cirrhosis who had an EGD for screening or surveillance of esophageal varices between 2000 and 2015.Cirrhotic patients who underwent EGD for an indication of screening or surveillance of varices were identified using the endoscopy electronic health record system,ProVation®,and the ICD-9-CM diagnosis codes 571.2,571.5,or 571.6.A subsequent chart review confirmed a diagnosis of cirrhosis based on physician assessment.Patients younger than 18 years,those with intra-luminal tumor or mechanical bowel obstruction,those with a prior diagnosis of gastroparesis or prior esophageal,gastric or thoracic surgery,and those who had an EGD indication which could confound gastric emptying(food impaction,foreign body,active gastrointestinal bleed,abdominal pain,nausea,vomiting,dyspepsia,bloating,weight loss,early satiety,or post-prandial fullness)were excluded.Retained gastric food was defined as any EGD with retained food documented in the procedure note for a unique patient.A control group who underwent EGD for an indication of anemia was identified using ProVation®and the ICD-9-CM Diagnosis Codes 280.*,281.*,or 285.9.Subsequent chart review excluded those with any known liver disease based on physician assessment.Anemia was chosen as the indication for EGD in the control group as it is unrelated to gastroparesis or its symptoms.
Demographic,clinical,laboratory,and endoscopic data were collected and managed using Research Electronic Data Capture tools hosted at Weill Cornell Medicine[24].Demographic information included age,sex,ethnicity,and body mass index.Clinical data included documented symptoms of delayed gastric emptying in the six months preceding EGD(i.e.,bloating,nausea/vomiting,early satiety/postprandial fullness,upper abdominal pain,or weight loss);current or past history of diabetes mellitus type 1,diabetes mellitus type 2,human immunodeficiency virus,neurological disorders(such as parkinsonism,multiple sclerosis,stroke,primary dysautonomias),infiltrative diseases(such as scleroderma or amyloidosis);causes of drug-induced gastroparesis(α-2 adrenergic agonists,tricyclic antidepressants,calcium channel blockers,dopamine agonists,muscarinic cholinergic receptor antagonists,octreotide,glucagon-like peptide-1 agonists,phenothiazines,cyclosporine,and any opioid);and use of prokinetic medications(metoclopramide,domperidone,erythromycin,or cisapride).Cirrhosis-specific details included model for end-stage liver disease score,Child-Pugh score,transient elastography results,liver biopsy results,hepatic venous pressure gradient,history of spontaneous bacterial peritonitis,history of hepatic encephalopathy(along with highest grade noted),history of esophageal varices(along with highest grade noted),history of ascites,history or development of hepatocellular carcinoma,and liver transplantation.Routine blood testing within 3 months of EGD was also obtained,including hemoglobin,platelets,sodium,blood urea nitrogen,creatinine,prothrombin time/international normalized ratio,total bilirubin,albumin,total protein,aspartate aminotransferase,alanine aminotransferase,alkaline phosphatase,hemoglobin A1C,thyroid stimulating hormone,and anti-nuclear antibodies.Endoscopic information included total number of endoscopies completed per patient over the study period,maximal point of EGD insertion,endoscopic findings,presence of pyloric stenosis or other evidence of gastric outlet obstruction,interventions performed,presence of solid gastric food contents,qualitative amount of retained gastric contents,visualization during EGD and whether lavage was required,and endoscopic findings on subsequent EGD within one year.
The primary outcome of the study was the frequency of retained gastric solid food contents,as documented in the procedural report by the endoscopist,in patients with cirrhosis undergoing EGD as compared to patients without liver disease undergoing EGD for anemia.Secondary outcomes included the relationship between retained gastric food contents with severity of cirrhosis by Child-Pugh score;and the association between retained gastric food contents with complications of decompensated cirrhosis as defined by presence of esophageal varices,ascites,or hepatic encephalopathy.
Categorical variables were described as frequencies(percentages)and continuous variables as(mean±SD).Characteristics of patients with and without retained food on EGD were compared using the Kruskall-Wallis test for non-parametric continuous variables andχ2or Fisher’s exact test for categorical variables,as appropriate.A multivariable logistic regression analysis was performed including co-variates statistically significant on univariable analysis.Statistical significance was defined by a two-tailedPvalue of less than 0.05.The statistical methods of this study were reviewed by biostatisticians in the Biostatistics,Epidemiology and Research Design Core within the Weill Cornell Clinical and Translational Science Center.Statistical analysis was performed using SAS statistical software version 9.4(SAS Institute Inc.,Cary,NC).
RESULTS
Between 2000 and 2015,364 patients with confirmed cirrhosis,who underwent a total of 1044 EGDs for the indication of variceal screening or surveillance,were identified.During the same period,519 control patients without liver disease,who underwent a total of 881 EGDs for the indication of anemia,were identified.Figure 1 shows the subject screening process and application of exclusion criteria.
Table 1 shows the baseline characteristics of these two groups.Cirrhotic patients had a mean age of 56 years as compared to 66 years in non-cirrhotic patients.Patients with cirrhosis were predominantly male(63%)compared to those without known liver disease who were predominantly female(55%).The vast majority of patients in both groups reported at least one upper gastrointestinal symptom within the six months prior to EGD.No patients had evidence of pyloric stenosis or other causes of gastric outlet obstruction on endoscopy.Well-established predisposing factors to gastroparesis,such as diabetes mellitus and opioid use,were similarly present in the two groups.Laboratory values demonstrated expected differences between the cirrhotic group and the non-cirrhotic,anemic group.Overall,40(4.5%)patients had evidence of retained food on EGD.Cirrhotics were more likely to have retained food on EGD than non-cirrhotics(9.1%vs1.4%,adjusted OR=5.83;95%CI:2.32-14.7,P<0.001).
Table 2 demonstrates the results of univariate analysis of the relationship between patient characteristics and the presence or absence of gastric food retention.Age younger than 60 years was associated with retained food(12.6%vs5.2%,P=0.015).Diabetes mellitus types 1 and 2 showed a trend towards a significant association with retained food(P=0.066).Opioid use was associated with retained food on EGD(P=0.004).More severe thrombocytopenia,a marker of worse portal hypertension,was also associated with the presence of retained food(P=0.027).Although no complications of decompensated cirrhosis were shown to be significantly associated,the presence of esophageal varices did show a trend towards significance(P=0.084).On the other hand,severity of Child-Pugh class was associated with retained food on EGD(P=0.007).
On multivariate logistic regression analysis,in addition to the presence of cirrhosis(adjusted OR=5.83;95%CI:2.32-14.7,P<0.001),diabetes mellitus(types 1 and 2 combined)(OR=2.34;95%CI:1.08-5.06,P=0.031),opioid use(OR=3.08;95%CI:1.29-7.34,P=0.011),and Child-Pugh class C(OR=4.29;95%CI:1.43-12.9,P=0.01)were also associated with a higher likelihood of food retention on EGD(Table 3).
DISCUSSION
This study is the first to describe the frequency of retained gastric food contents visualized on EGD in a cirrhotic population.Our study reveals that cirrhotic patients are five times more likely to have retained food on EGD than controls.In addition,more decompensated cirrhosis was associated with a higher likelihood of gastric food contents at EGD.

Figure 1 Flow chart of patient inclusion for cases(A)and controls(B).1Wrong indication for EGD includes food impaction,foreign body,melena,hematochezia,hematemesis,abdominal pain,nausea,vomiting,dyspepsia,bloating,weight loss,early satiety or post-prandial fullness.EGD:Esophagogastroduodenoscopy.
Cirrhosis has been associated with increased nitric oxide(NO)production,gut hormonal alterations,and autonomic neuropathy that can impact gastrointestinal motility[3].Gut hormonal alterations related to insulin resistance,including hyperglycemia,hyperinsulinemia,and hypoghrelinemia can play a prominent role in the pathophysiology of delayed gastric emptying in patients with cirrhosis[17].Portal hypertension has also been implicated as a potential mechanism given decreased postprandial portal blood flow resulting in congestion of the gastric wall as well as impaired antral compliance and motility[3].Prolonged gastric emptying has been demonstrated in 24%-95% of patients with cirrhosis and upper gastrointestinal symptoms not attributable to other causes[1,2,4,5].These often vague upper GI symptoms have been shown to contribute significant morbidity in the cirrhotic population through malnutrition[4],small intestinal bacterial overgrowth[4],psychological distress[6],and reduced health related quality of life measures[6].
The factors associated with gastric retention in the study population include ageyounger than 60,diabetes mellitus,opioid use,thrombocytopenia,and higher Child-Pugh class.Opioid use and diabetes mellitus are well described risk factors for gastroparesis.The association of diabetes with delayed gastric emptying lends further support to the role of insulin resistance in the pathogenesis of gastroparesis in cirrhotic patients,as previously described in Kalaitzakiset al[17].Regarding the association of age and gastroparesis,it is unclear why gastric food retention was associated with younger age.Given that young age was associated with delayed gastric emptying on univariate analysis but not multivariate analysis,there are likely confounding factors at play.A novel finding is the fact that gastric retention is associated with decompensated cirrhosis as can be elucidated from the association with thrombocytopenia and higher Child-Pugh class.Additionally,there was a trend towards significance with the presence of esophageal varices that further supports an association between severity of cirrhosis,portal hypertension,and gastroparesis.Prior studies evaluating the association between severity of cirrhosis and gastroparesis have shown mixed results.The majority of studies have shown no association between severity of cirrhosis and gastroparesis[2,5,12,13,16,25].However,the correlation between severity of cirrhosis and delayed gastric emptying seen in this study is similar to two previous studies[1,14].Gumurduluet al[1]demonstrated that Child-Pugh class correlated with delayed gastric emptying,as measured by scintigraphy,and Miyajimaet al[14]concluded a similar association using measurements of autonomic function and portal blood flowviaMRI.Despite the different methodologies used in those studies and the present study,the similar conclusions lend further credence to the results of the current study.
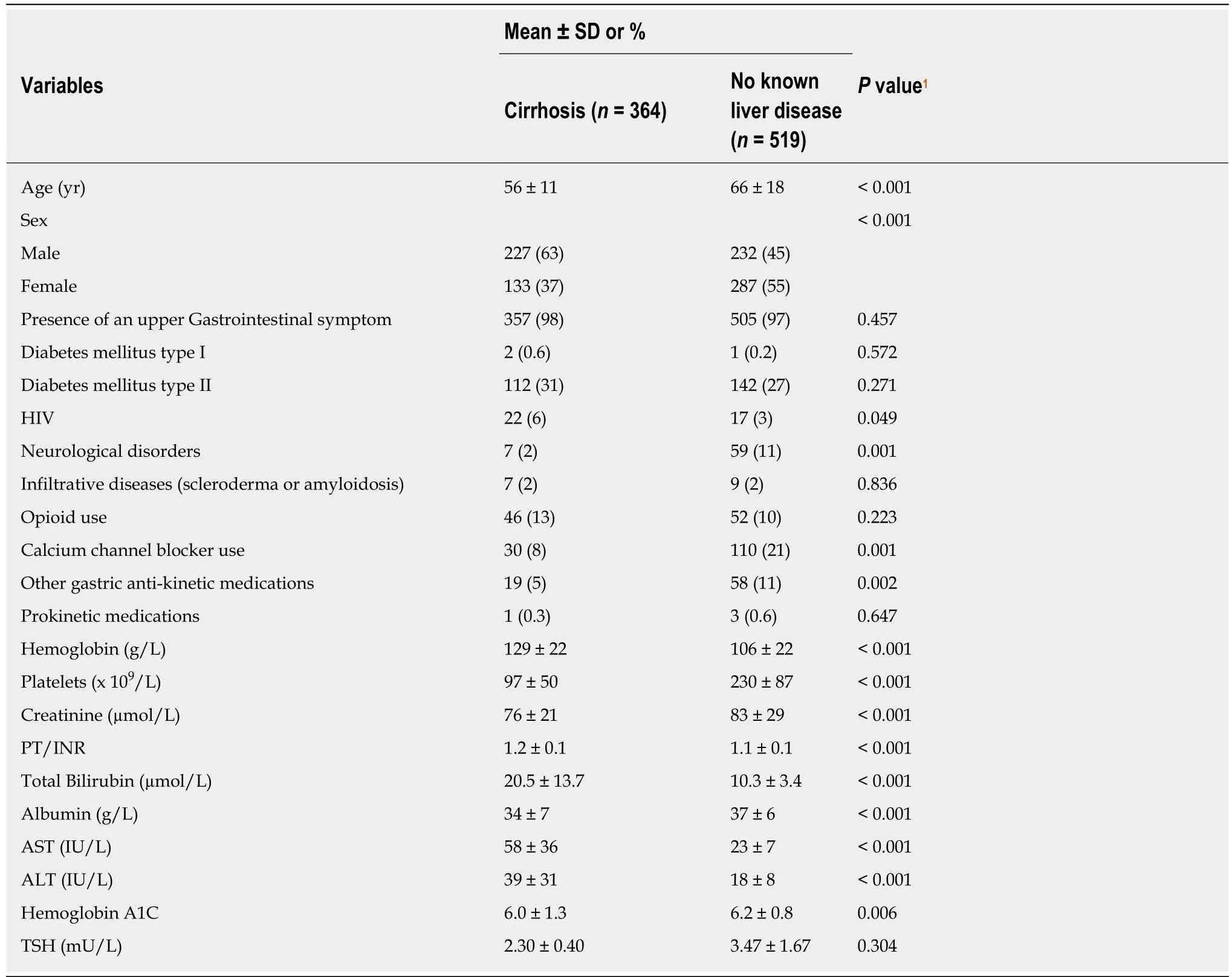
Table 1 Baseline characteristics of patients with cirrhosis and without known liver disease
This study has several limitations.Given its retrospective non-interventional nature,no conclusions can be drawn regarding causality.Future studies shouldconsider prospectively recruiting patients to confirm these results,though time constraints might make prospective recruitment and longitudinal follow-up difficult.Since this is a single center study at an academic center,the results may also lack generalizability.Additionally,the presence of retained food on EGD is not the gold standard method for diagnosing gastroparesis;but,there exists strong evidence for correlation[22].
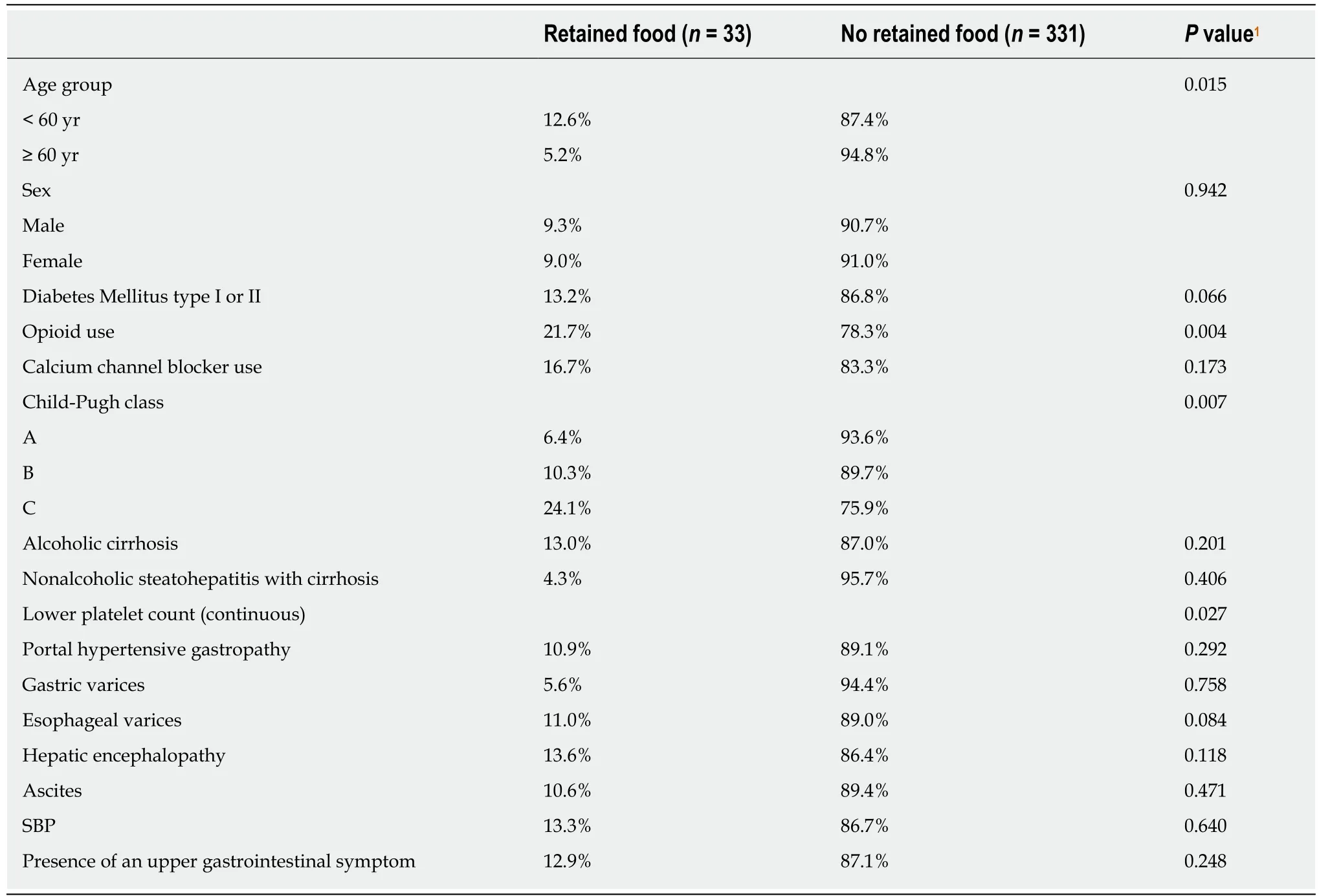
Table 2 Relationship between patient characteristics and retained food in cirrhotics
In conclusion,we demonstrate that cirrhotic subjects have a higher likelihood of delayed gastric emptying than non-cirrhotics,particularly in those with decompensation of their liver disease.Providers who care for cirrhotic patients should have a high index of suspicion for symptoms related to delayed gastric emptying,a condition which is vastly underrecognized in this patient group.Ultimately,a prospectively validated prediction tool would be useful for the detection of impaired gastric motility in cirrhotic patients.Future studies should evaluate the effect of delayed gastric emptying on patient reported outcomes,quality of life and health care utilization.
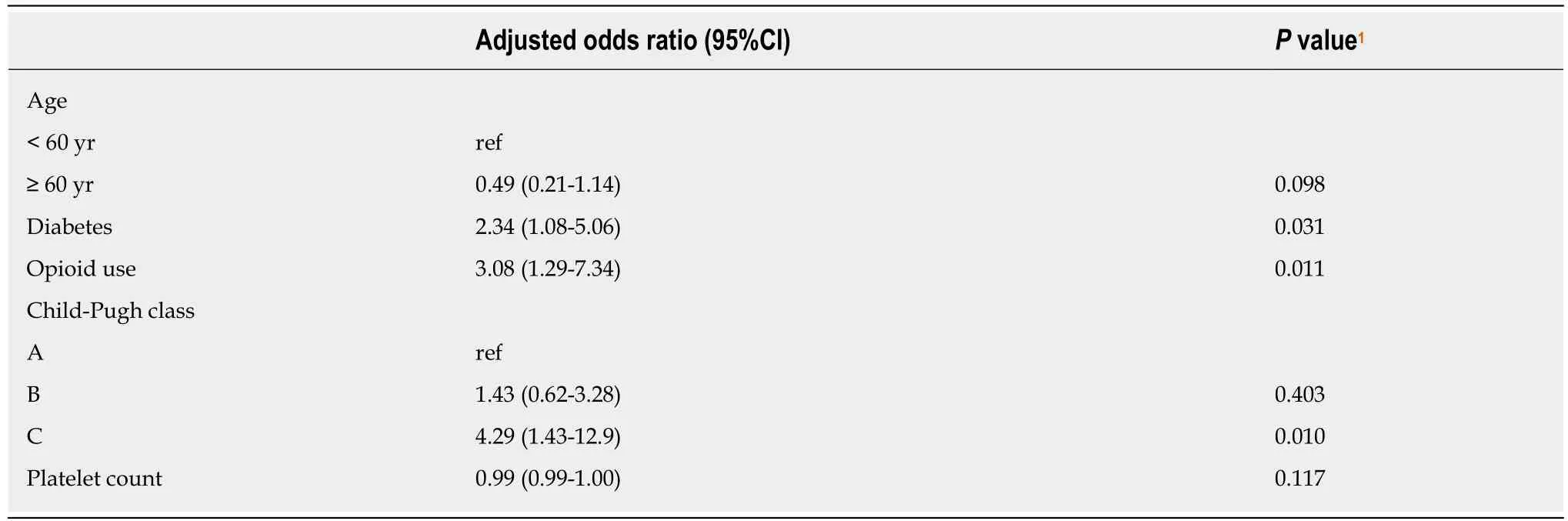
Table 3 Multivariate analysis for retained food in cirrhotic patients
ARTICLE HIGHLIGHTS
Research background
Many patients with cirrhosis report gastrointestinal(GI)symptoms such as abdominal bloating,pain,and belching.Cirrhosis has been associated with increased nitric oxide(NO)production,gut hormonal alterations,and autonomic neuropathy that can impact gastrointestinal motility.Portal hypertension has also been implicated as a potential mechanism given decreased postprandial portal blood flow resulting in congestion of the gastric wall as well as impaired antral compliance and motility.Prolonged gastric emptying has been demonstrated in 24%-95%of patients with cirrhosis and upper gastrointestinal symptoms not attributable to other causes.These usual vague upper GI symptoms have been shown to contribute significant morbidity in the cirrhotic population through malnutrition,small intestinal bacterial overgrowth,psychological distress,and reduced health related quality of life measures.
Research motivation
The prevalence of GI symptoms has prompted investigation into abnormalities in GI function in cirrhosis.Cirrhotic patients have higher rates of gastrointestinal dysmotility,characterized by delayed gastric emptying and prolonged small bowel transit time,compared to those without cirrhosis.While severity of cirrhosis has been associated with worsened small bowel motility,the relationship between gastric emptying and severity of liver disease has not been well established.The mechanisms for gastrointestinal dysmotility in cirrhosis are also not fully understood.Although some studies have correlated markers of portal hypertension with delayed gastric emptying,those examining the size of esophageal varices,variceal pressure,and hepatic venous pressure gradient,have failed to demonstrate an association with impaired gastric motility.Examination of the risk factors for delayed gastric emptying in patients with cirrhosis could provide further insight into the underlying pathophysiology and could help identify patients who may benefit from therapeutic interventions aimed at improving gastric motility.
Research objectives
The presence of retained gastric food on esophagogastroduodenoscopy(EGD)can be used as a surrogate for delayed gastric emptying with a reasonably high specificity.Since patients with cirrhosis frequently require EGD for surveillance and treatment of esophageal varices,evaluation for retained gastric food contents at EGD could provide important clinical information in this population.Therefore,we conducted this study to characterize the frequency of retained gastric food contents at EGD in a cirrhotic population compared to a control population without liver disease and to elucidate factors predictive of retained food.Specifically,we examined the relationship between retained gastric food contents with severity of cirrhosis by Child-Pugh score;and the association between retained gastric food contents with complications of decompensated cirrhosis as defined by the presence of esophageal varices,ascites,or hepatic encephalopathy.
Research methods
We performed a retrospective case-control study of patients with cirrhosis who had an EGD for screening or surveillance of esophageal varices between 2000 and 2015 at an academic medical center.Patients younger than 18 years,those with intra-luminal tumor or mechanical bowel obstruction,those with a prior diagnosis of gastroparesis or prior esophageal,gastric or thoracic surgery,and those who had an EGD indication which could confound gastric emptying(food impaction,foreign body,active gastrointestinal bleed,abdominal pain,nausea,vomiting,dyspepsia,bloating,weight loss,early satiety,or post-prandial fullness)were excluded.A control group who underwent EGD for an indication of anemia was identified as anemia is unrelated to gastroparesis or its symptoms.Three hundred sixty-four patients with confirmed cirrhosis,who underwent a total of 1044 EGDs for the indication of esophageal variceal screening or surveillance,were identified.During the same period,519 control patients without liver disease,who underwent a total of 881 EGDs for the indication of anemia,were identified.The presence of retained food on EGD was used as a surrogate for delayed gastric emptying.The relative frequency of delayed gastric emptying among cirrhotics was compared to non-cirrhotics.Characteristics of patients with and without retained food on EGD were compared using the Kruskall-Wallis test for non-parametric continuous variables andχ2or Fisher’s exact test for categorical variables,as appropriate.A multivariable logistic regression analysis was performed including co-variates statistically significant on univariable analysis.Statistical significance was defined by a two-tailedPvalue of less than 0.05.
Research results
Overall,40(4.5%)patients had evidence of retained food on EGD.Cirrhotics were more likely to have retained food on EGD than non-cirrhotics(9.1%vs1.4%,OR=5.83;95%CI:2.32-14.7,P<0.001).Characteristics associated with retained food on univariable analysis included age less than 60 years(12.6%vs5.2%,P=0.015),opioid use(P=0.004),Child-Pugh class C(24.1% Child-Pugh class Cvs6.4% Child-Pugh class A,P=0.007),and lower platelet count(P=0.027).Diabetes mellitus showed a trend towards a significant association with retained food(P=0.066).Although no complications of decompensated cirrhosis were shown to be significantly associated,the presence of esophageal varices did show a trend towards significance(P=0.084).On multivariate logistic regression analysis,in addition to the presence of cirrhosis,diabetes mellitus(types 1 and 2 combined)(OR=2.34;95%CI:1.08-5.06,P=0.031),opioid use(OR=3.08;95%CI:1.29-7.34,P=0.011),and Child-Pugh class C(OR=4.29;95%CI:1.43-12.9,P=0.01)were also associated with a higher likelihood of food retention on EGD.
Research conclusions
This study is the first to describe the frequency of retained gastric food contents visualized on EGD in a cirrhotic population.Our study reveals that cirrhotic patients are five times more likely to have retained food on EGD than controls.In addition,more decompensated cirrhosis was associated with a higher likelihood of gastric food contents at EGD.The factors associated with gastric retention in the study population include age younger than 60,diabetes mellitus,opioid use,thrombocytopenia,and higher Child-Pugh class.Opioid use and diabetes mellitus are well described risk factors for gastroparesis.A novel finding is the fact that gastric retention is associated with decompensated cirrhosis as can be elucidated from the association with thrombocytopenia and higher Child-Pugh class.Additionally,there was a trend towards significance with the presence of esophageal varices that further supports an association between severity of cirrhosis,portal hypertension,and gastroparesis.Prior studies evaluating the association between severity of cirrhosis and gastroparesis have shown mixed results.However,the correlation between severity of cirrhosis and delayed gastric emptying seen in this study is similar to two previous studies.Gumurduluet aldemonstrated that Child-Pugh class correlated with delayed gastric emptying,as measured by scintigraphy,and Miyajimaet alconcluded a similar association using measurements of autonomic function and portal blood flowviaMRI.Despite the different methodologies used in those studies and the present study,the similar conclusions lend further credence to the results of the current study.Clinicians should have a higher index of suspicion for upper GI symptoms related to dysmotility in those with more decompensated cirrhosis,so that these patients can undergo timely diagnosis and treatment.
Research perspectives
We demonstrate that cirrhotic subjects have a higher likelihood of delayed gastric emptying than non-cirrhotics,particularly in those with decompensation of their liver disease.Future studies should consider prospectively recruiting patients in multiple centers to confirm these results,though time constraints might make prospective recruitment and longitudinal follow-up difficult.Additionally,since the presence of retained food on EGD is not the gold standard method for diagnosing gastroparesis,prospective studies could utilize gastric scintigraphy,which remains the gold standard for diagnosis.Providers who care for cirrhotic patients should have a high index of suspicion for symptoms related to delayed gastric emptying,a condition which is vastly underrecognized in this patient group.Ultimately,a prospectively validated prediction tool would be useful for the detection of impaired gastric motility in cirrhotic patients.Future studies should evaluate the effect of delayed gastric emptying on patient reported outcomes,quality of life and health care utilization.
ACKNOWLEDGEMENTS
The authors gratefully acknowledge the Clinical and Translational Science Center at Weill Cornell Medicine for their support in research design and biostatistical analysis.