Assessment of clinical dehydration using point of care ultrasound for pediatric patients in rural Panama
2019-11-24GenevieveMazzaCarinaMirelesRomoMarleneTorresAliDuffensAnnashaVyasKatherineMoranJoshuaLivingstonSavannahGonzalesShadiLahhamInnaShniterMaxwellThompsonJohnChristianFox
Genevieve Mazza, Carina Mireles Romo, Marlene Torres, Ali Duffens, Annasha Vyas, Katherine Moran, Joshua Livingston, Savannah Gonzales, Shadi Lahham, Inna Shniter, Maxwell Thompson, John Christian Fox
1 School of Medicine, University of California Irvine, Irvine, CA 92697, USA
2 Department of Emergency Medicine, University of California Irvine, Orange, CA 92868, USA
KEY WORDS: Ultrasound; Parasitic infection; Panama; Rural medicine; Dehydration; Medical education
INTRODUCTION
Dehydration and its associated symptoms are among the most common chief complaints for children in rural Panama. This is often caused by diarrheal illness secondary to parasitic infection, in the context of poor sanitation.[1,2]The World Health Organization recommends assessing dehydration in children based on four clinical features: general appearance, eyes (whether they appear sunken), history of thirst, and skin pinch to assess turgor.[3]However, these clinical signs may be subtle or nonspecific and thus have important limitations if used as independent predictors of dehydration. A more objective way to assess for dehydration using serum and urine analysis has been implicated.[4,5]However,in a resource-limited setting, laboratories that perform serum and urine analysis may not be easily accessible.Additionally, studies on dehydration have shown serum and urine analysis do not show sufficient sensitivity,specificity or reliability[3,4]and are typically only useful in children with moderate to severe hypovolemia.
Bedside ultrasonography is a noninvasive method that can serve as a more objective tool for assessing dehydration in both adults and children. Point-of-care ultrasound has the potential to reduce unnecessary use of resources such as IV fluids or hospital access, while identifying children who are severely dehydrated and need immediate medical attention.[6]Previous studies have shown that intravascular volume correlates to the ratio of the diameters of the inferior vena cava(IVC) to the aorta (Ao). This concept is predicated on the assumption that the IVC/Ao diameter ratio of symptomatic patients would be less than 0.8, a threshold established as a clinical marker of significant dehydration in studies involving American children.[4]
Previous studies have shown that medical students are capable of performing accurate focused point-ofcare ultrasound scans.[7-9]Thus, in resource-poor settings,healthcare workers with minimal training may be able to use ultrasound to identify and treat dehydration. To date, no clinical studies have evaluated dehydration using ultrasound in rural Panama. Additionally, while it was apparent that there are many healthcare disparities present in rural Panama, little is documented and researched about this population. The World Bank reports that mortality rates for Ngobe children under five years old are nearly twice the national Panamanian average.[10]Furthermore, poverty is highest among the Ngobe population, Panama’s largest ethnic indigenous group. Indigenous communities in Panama have greater gaps in all basic infrastructure services, including potable water, sanitation, and electricity.[11]The poor infrastructure contributes to the poor sanitation and ongoing transmission of parasitic infections. For these reasons, identification of an objective, portable and costeffective method of identifying dehydration is important.There are growing opportunities for the use of ultrasound in low-resource settings, especially given the declining costs of portable ultrasound machines and the profound lack of reported data regarding ultrasound as a low-cost imaging alternative in the developing world.[3]
The primary objective of our study is to determine if minimally-trained first year medical students can perform point-of-care ultrasound of the IVC and aorta on children in rural Panama to assess for dehydration. We hypothesize that IVC/Ao ratio will be lower in the dehydrated children as compared to the asymptomatic children.
METHODS
Study design
This was a prospective, observational study conducted in the Bocas del Toro region of rural Panama between June 2017 and July 2017. This research was conducted in collaboration with Floating Doctors, a non-profit organization with clinics in Bocas del Toro, Panama.Patients were enrolled via a convenience sample of pediatric patients presenting to the clinic. Prior to patient enrollment, the study was approved by the site Institutional Review Board. Consent was obtained from all pediatric patients and their guardians.
Study setting and population
The study was conducted in the Bocas del Toro region of Panama in clinics run by Floating Doctors.These clinics provide medical care for the rural indigenous population living in the Bocas del Toro region of Panama. Over four weeks, American trained first year medical students travelled to six different primary care clinics to enroll eligible patients. All of the subjects enrolled in the study spanned the ages of 11 months to 13 years of age. Our subjects were divided into two groups: the study group consisted of 24 children presenting to clinic with complaints of diarrhea and/or vomiting with concerns for a parasitic infection, which put them at increased risk for dehydration. The control group consisted of 35 children from the local village who were present in the clinic but were asymptomatic.
Study protocol
Medical volunteers were present in each clinic during regular clinic hours. The subjects were chosen from a convenience sample of both symptomatic and asymptomatic children that were present at the clinic.When an eligible child was identified by the volunteers,research associates were notified. The patient and guardian were then approached by the research team and explained the purpose of the study. Enrollment in the study was voluntary and did not affect the patient’s care.A study information sheet, translated into Spanish, was presented to the subject’s guardian and was discussed with the guardian prior to obtaining consent. Once consented, the subject underwent ultrasound by the medical students.
Prior to enrolling subjects, a total of eight American allopathic medical students were recruited for the study.All eight medical students had completed their first year of medical education. This included completion of the following courses: human physiology, human anatomy, cardiac anatomy and ultrasound education.The ultrasound training for the group consisted of 3 hours of pre-session podcast online lectures followed by three hours of supervised hands-on training with live standardized patients. Students were approved to begin enrolling patients after successful completion of a competency practical exam by the site ultrasound director. The ultrasound director was a board-certified emergency medicine physician who completed a oneyear point of care ultrasound fellowship.
Ultrasounds were performed using Mindray M7(Shenzhen Mindray Bio-Medical Electronics Co., Ltd.,Shenzhen, China) portable ultrasound machines. Each machine was equipped with a single phased array probe.During enrollment, subjects were placed in a supine position. The phased array transducer was placed over the anterior abdomen in the transverse plane beginning inferior to the xiphoid process. The indicator was directed towards the patient’s right side. In this view, the IVC and abdominal aorta were visible in cross section(Figure 1). Transducer was moved distally and the maximal anterior to posterior diameters of the IVC and aorta were measured using calipers placed on the outer walls during systole for the aorta and during expiration for the IVC (Figure 1).
Data collection

Figure 1. Ultrasonographic measurements of the IVC/Ao ratio in the transverse view.
Eight medical students enrolled a total of 59 patients from 6 different clinic locations. The patients’ages ranged from 11 months to 13 years of age. Of these 59 patients, 24 were patients clinically diagnosed as having dehydration, while the remaining 35 were asymptomatic and presumed to have normal hydration status. For patients with dehydration, the most common diagnosis was parasitic infection. Other presenting diagnoses include scabies, fever, cellulitis, and upper respiratory infection. Basic demographic data was collected from each enrolled patient (Table 1). The IVC and Ao diameters (cm) were measured and an Ao/IVC ratio was calculated for each patient. This information was entered a Microsoft Excel spreadsheet for analysis.Video clips and on-screen measurements were recorded and retrospectively reviewed by the ultrasound director for adequacy.
RESULTS
An independent-samples two-tailedt-test was conducted to compare IVC/Ao ratios between the dehydrated and normal patients. Subjects diagnosed with dehydration had insignificantly higher IVC/Ao ratios (M=0.872SD=0.185)than the asymptomatic subjects deemed to have normal hydration status ([M]=0.785SD=0.185,t[57]=2.00,P=0.081) (Figure 2, Table 2). This suggests that there is no real difference between the two groups.
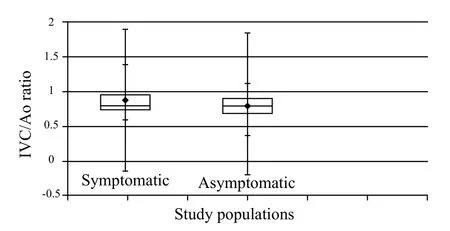
Figure 2. Box plot of Ao/IVC ratio for symptomatic and asymptomatic children's = individual mean with 95% CI.

Table 2. Descriptive statistics for symptomatic vs. asymptomatic patients
DISCUSSION
Previous studies have found that ultrasound can be useful in assessing dehydration using the IVC/Ao ratio,with an IVC/Ao ratio less than 0.8 being the threshold established as a clinical marker of severe dehydration in American children.[12]A recent prospective, observational study by Kwon et al[13]evaluated dehydration in children using ultrasound by measuring the aorta/IVC cross sectional area (Ao/IVCA) and the aorta/IVC maximal diameter index (Ao/IVCD). They compared the Ao/IVCA to both the Ao/IVCD and the clinical dehydration scale (CDS). They found that when comparing the two parameters to the clinical dehydration scale, only the aorta/IVCA had a statistically significant correlation with the CDS. The researchers suggest that perhaps the Ao/IVCA is a better diagnostic index for assessing dehydration than the Ao/IVCD, which was the method employed in our study.[10]This holds promise that perhaps ultrasound may still be a diagnostic tool in assessing dehydration in children but may need a modification to the current protocol for how the images are analyzed.
Additionally, Modi et al[6]found a significant correlation of aorta/IVC ratio predicting dehydration,but they determined that the aorta/IVC ratio could not discriminate between levels of dehydration.They concluded that ultrasound is not a strong enough screening tool to be used solely by providers to determine management of children with diarrhea but suggested alternative ultrasound measurements like bladder ultrasound and carotid flow time to determine dehydration.
Our study results did not support previous literature showing that the IVC/Ao ratio is lower in children with dehydration.[12]It is possible that due to the chronic dehydration, inadequate access to safe drinking water,and higher rates of parasitic infection, the Ngobe population has developed a physiologic mechanism for compensating for their chronically low volume state that makes detecting dehydration using ultrasound more challenging. However, we must also consider that our study was not adequately powered to detect a true effect in either direction. A post-hoc power analysis revealed a power of only 42.7%. We were unable to estimate sample size a priori as there was a lack of prevalence data for patient presenting to the clinic with symptoms suggestive of dehydration. To date, no previous clinical studies have evaluated dehydration using ultrasound in rural Panama.Our current project may serve as a pilot study to guide researchers in determination of sample size to be able to appropriately power future studies.
Limitations
There are several limitations for this study. We were unable to calculate an estimated sample size in advance to appropriately power the study as we did not have access to prevalence data. With a post-hoc analysis we found that the sample of 59 subjects was not enough to power the study to be able to detect a difference between groups. Next, the findings of patients enrolled at these clinics may not be generalizable to compare with children in prior studies. Given rates of chronic dehydration, asymptomatic patients may have presented with abnormal IVC/Ao ratio despite being asymptomatic.Due to the lack of available resources, laboratory testing was not performed to assess for dehydration and only clinical exam was used to identify patients for dehydration. As such, there was no gold standard used for comparison. Next, inter-rater reliability was not evaluated and variation in measurements between different ultrasonographers could have contributed to different outcomes.
CONCLUSION
Dehydration in children is one of the largest health problems in developing countries, with parasitic infections being the most common cause of morbidity and mortality.[14]In these resource-limited settings,ultrasonography has the potential to serve as a more objective tool in assessing dehydration in children.While there is conflicting evidence regarding exactly which ultrasound parameters used to assess dehydration,ultrasound remains promising as a tool to evaluate dehydration in resource-limited settings. Further investigation with larger scale studies is needed to identify the appropriate ultrasound parameters to evaluate dehydration in rural Panama.
ACKNOWLEDGMENTS
Floating Doctors, UC Irvine Health Department of Emergency Medicine, UC Irvine School of Medicine.
Funding:None.
Ethical approval:The study was approved by the site Institutional Review Board..
Conflicts of interest:Dr. J Christian Fox receives stock options from Sonosim for consulting. However, no Sonosim products were used in this research project.
Contributors:All authors made an individual contribution to the writing of the article including: conception and design, acquisition of data or analysis and interpretation of data; drafting the article or revising it critically for important intellectual content; final approval of the version published.
杂志排行

World journal of emergency medicine的其它文章
- Information for Readers
- World Journal of Emergency Medicine
- Venous thromboembolism in the emergency department: A survey of current best practice awareness in physicians and nurses in China
- The use of outcome feedback by emergency medicine physicians: Results of a physician survey
- Rapid sequence induction (RSI) in trauma patients:Insights from healthcare providers
- Comparison between intravenous morphine versus fentanyl in acute pain relief in drug abusers with acute limb traumatic injury