An update on biomarkers of potential benefit with bevacizumab for breast cancer treatment: Do we make progress?
2019-09-10XuLiangHuipingLiFlorenceCoussyCelineCallensFlorenceLerebours
Xu Liang, Huiping Li, Florence Coussy, Celine Callens, Florence Lerebours
1Key Laboratory of Carcinogenesis and Translational Research (Ministry of Education/Beijing), Department of Breast Oncology, Peking University Cancer Hospital & Institute, Beijing 100142, China; 2Department of Medical Oncology, Institut Curie, PSL Research University, Paris 75005,France; 3Pharmacogenomic Unit, Department of Genetics, Curie Institute, PSL Research University, Paris 75005, France; 4Department of Medical Oncology, Institut Curie, René Huguenin Hospital, Saint-Cloud 92210, France
Abstract As the first monoclonal antibody against vascular endothelial growth factor (VEGF), bevacizumab (BEV) is a definitely controversial antiangiogenic therapy in breast cancer. The initial excitement over improvements in progression-free survival (PFS) with BEV was tempered by an absence of overall survival (OS) benefit and serious adverse effects. Missing targeted population urged us to identify the predictive biomarkers for BEV efficacy. In this review we focus on the research in breast cancer and provide recent investigations on clinical, radiological,molecular and gene profiling markers of BEV efficacy, including the new results from randomized phase III clinical trials evaluating the efficacy of BEV in combination with comprehensive biomarker analyses. Current evidences indicate some predictive values for genetic variants, molecular imaging, VEGF pathway factors or associated factors in peripheral blood and gene profiling. The current challenge is to validate those potential biomarkers and implement them into clinical practice.
Keywords: Bevacizumab; efficacy; biomarker; breast cancer
Introduction
The addition of bevacizumab (BEV) to chemotherapy for metastatic breast cancer (MBC) was first proposed a decade ago. Solid tumor strongly requires a new blood vessel formation to provide quick-proliferating tumor cells with an adequate supply in oxygen and nutrients, therefore,targeting angiogenesis agent theoretically should be useful in cancer treatment. After BEV, more than ten agents that target vascular endothelial growth factor (VEGF) or its receptor (VEGFR) have been approved for the treatment of various malignant tumors (1), unfortunately, BEV as a monoclonal antibody against VEGF has been failed to prove overall survival (OS) benefit of MBC (2). The interest of physicians to BEV was descending after USA Food and Drug Administration (FDA) withdrew the approval, and also because of many novel agents bringing breakthrough results in therapy of MBC. Whether there is still any room for BEV in MBC, whether a particular subgroup of patients will benefit from BEV more than the others, it is a question continuing to be asked. In CALGB 40503 trial, the addition of BEV to letrozole improved progression-free survival (PFS) from a median of 15.6 months with letrozole alone to 20.2 months in hormone receptor-positive MBC, but still with a markedly increasing toxicities, which required a research on markers (3).Meanwhile, TURANDOT trial interestingly represented that BEV plus capecitabine was associated with better OS than BEV plus paclitaxel in post-menopausal women with a body surface area less than 1.8 m2in an exploratory analysis(4). And more recently, in a phase II study at premenopausal women with human epidermal growth factor receptor 2 (HER2)-negative, local advanced breast cancer(LABC), Tampaki et al. indicated that neoadjuvant treatment with BEV, liposomal doxorubicin, cyclophosphamide and paclitaxel combination seemed to be an effective alternative choice with manageable safety profile(5). Thus, BEV still does have a substantial role in the management of MBC and LABC. To date, a biomarker that defines the subset of MBC patients most likely benefit from BEV has not been identified. For most physicians,there is no evidence suggesting that factors other than clinical reasons should influence patient selection for BEV,but those clinical standards are equivocal and indecisive,depending on various conditions (6). VEGF is a master regulator of angiogenesis, and should be expected to predict response to BEV (7). Several trials have assessed the predictive value of circulating VEGF-A levels in serum, but the results of different studies are not consistent, it seems that the efficacy of BEV might not be predicted simply by one factor. The aim of this present review is to update the recent studies of predictive biomarkers for BEV efficacy in breast cancer (BC).
Genetic variability
As the host factors may influence angiogenesis, it was hypothesized that genetic variability may lead to different responses to BEV. Polymorphisms in components of the VEGF pathway have been proposed to predict benefit from BEV. The clinical trials of BEV in BC with simultaneous translational research in genetic variants were limited(Table 1, Figure 1A). In MBC E2100 trial, carriers of the rs699947 and rs1570360 single-nucleotide polymorphisms(SNPs), which correlate with reduced expression of VEGFA, were significantly associated with improved OS in the BEV arm but not in the control arm (8). However, they were not confirmed in the latter AVADO trial as rs699947 showed a weak correlation with PFS in the placebo arm but not in BEV arm. In the BEV 7.5 mg/kg arm, there was an indication of potential treatment-by-genotype interaction(interaction P=0.018) for the rs699947 for PFS, and the rs1570360 SNP showed a weak correlation with PFS, but neither of them showed correlation in the BEV 15 mg/kg arm. The results of SNP-based analyses of the AVADO trial did not confirm the previously reported correlations between SNPs and efficacy in the E2100, AViTA, and AVOREN trials. Furthermore, none of the 26 SNPs involved in angiogenesis and tumorigenesis which was evaluated in AVADO trial correlated with BEV efficacy (9).
The randomized phase III GeparQuinto study reported that addition of BEV to neoadjuvant chemotherapy improved pathological complete response (pCR), in particular in triple-negative breast cancer (TNBC)subgroup (39.3% vs. 27.9%, P=0.003). In this trial, 125 SNPs of 15 genes from VEGF pathway were investigated in 729 BEV treated patients and 724 control patients. Five variants of VEGF-A (rs833058, rs699947, rs3025030,rs3025039) and VEGFR-1 (rs7995976) were found associated with an improved pCR in BEV treatment arm,especially in TNBC patients (10). Although none of them remained significant after adjustment for multiple testing,these gene variants were consistent with previous studies on BEV efficacy in BC: the VEGF-2578 AA genotype of rs699947 was associated with a better response to BEV in the present GeparQuinto study (OR=2.24; 95% CI:1.31-3.84). Furthermore, a meta-analysis of six randomized phase III trials reported for 195 SNPs in testing the addition of BEV to standard chemotherapy in colorectal,pancreatic, lung, renal, breast and gastric cancer, involving a total of 716 BEV treated patients and 686 patients receiving placebo. In this analysis, the variants of VEGF-A,VEGF-C, hypoxia inducible factor-2α (EPAS1), interleukin-8 (IL-8) receptor α (IL8RA), and von Hippel-Lindau tumor suppressor (VHL) genes were potential predictors of BEV treatment across tumor types. The same VEGF-A SNPs identified in GeparQuinto also showed significant association with PFS in this meta-analysis, in particular, AA carriers of rs833058 had prolonged PFS (15).
IL-8 was accepted for an angiogenesis mediator of a VEGF-independent angiogenic pathway. More evidences showed that IL-8 up-regulation is a mechanism of “escape”from VEGF-dependent angiogenic block (16). Correlation between the level of IL-8 and BEV resistance was confirmed in renal cancer, head and neck squamous cell carcinoma, and colorectal cancer (17-19). A retrospective study in MBC reported that a germline polymorphism in the IL-8 gene, which consists of a T to A substitution at position -251, was associated with treatment outcome of BEV combined chemotherapy (13). A similar association was reported in a phase II clinical trial on recurrent/-metastatic epithelial ovarian cancer patients (20).

Table 1 Studies assessing polymorphism biomarkers in relation to activity or efficacy of BEV
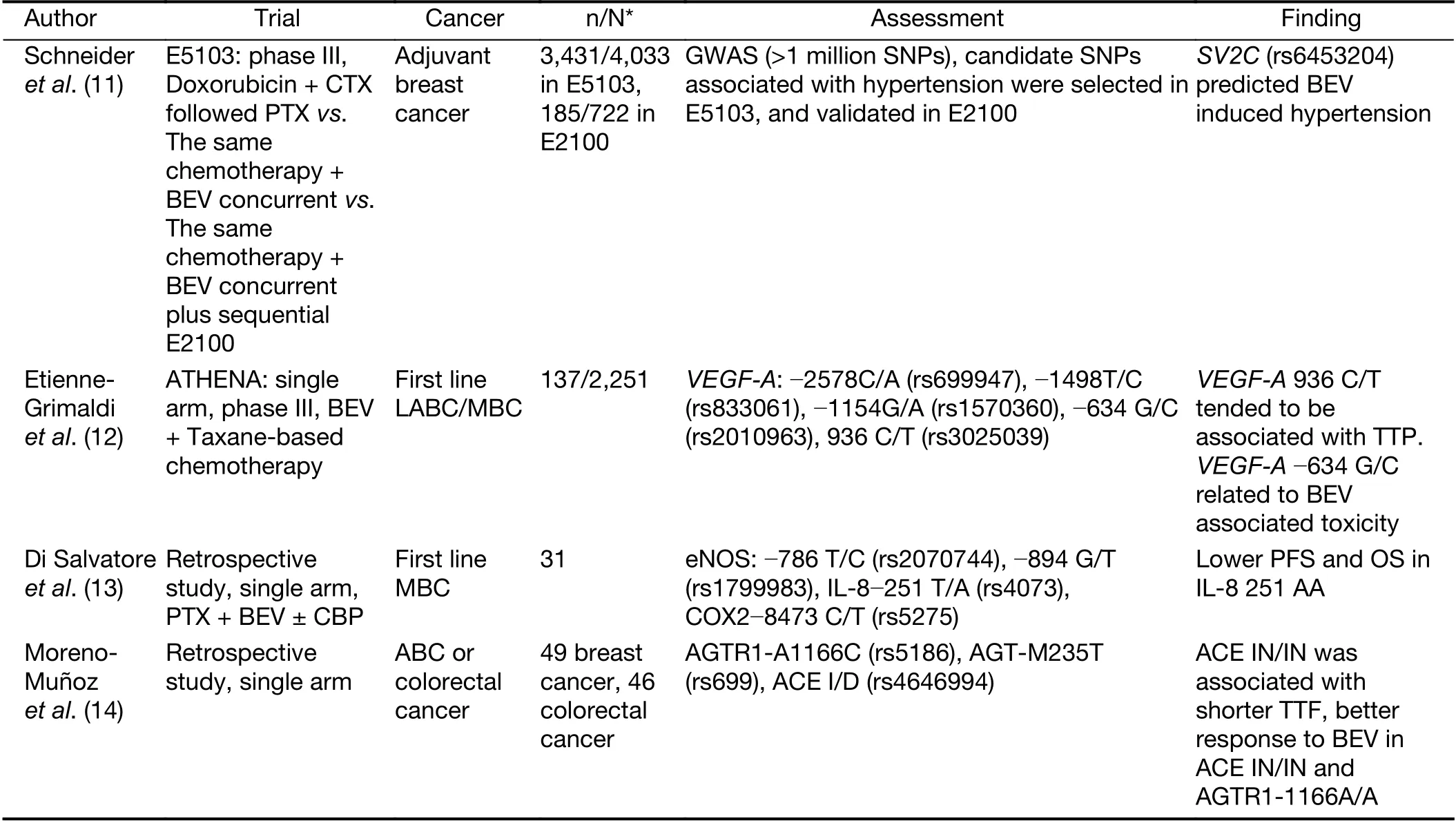
Table 1 (continued)
A study in MBC and colorectal cancer represents an analysis of renin-angiotensin system (RAS) genetic variants as predictive markers of BEV treatment outcome (14). The angiotensin-converting-enzyme (ACE) IN/IN genotype was associated with a higher rate of disease progression and shorter time to treatment failure. Meanwhile ACE IN/IN genotype showed lower level of circulating ACE, whereas higher circulating ACE levels were found to be associated with a better response to BEV treatment. Similarly,angiotensin II (AngII) receptor 1 (AGTR1) -1166 AA genotype was also associated with a higher rate of disease progression compared with the AC and CC genotypes(24.4% vs. 2.7%, P<0.01). Hypertension was found associated with efficacy of BEV, and several studies interestingly reported that the AGTR1-1166 CC genotype is associated with increased predisposition to hypertension(21-23). This study indicates that a higher activity of the ACE-AngII-AGTR1 axis is associated with a better response to BEV, and probably explains part of reasons that secondary hypertension might predict better treatment result of BEV. A genetic variant in synaptic vesicle glycoprotein 2C (SV2C rs6453204) predicted clinically relevant BEV-induced hypertension in two independent randomized phase III clinic trials E-5103 and E-2100, and further evaluation of SV2C as a predictive marker for efficacy are ongoing in E5103 trial (11).
Imaging
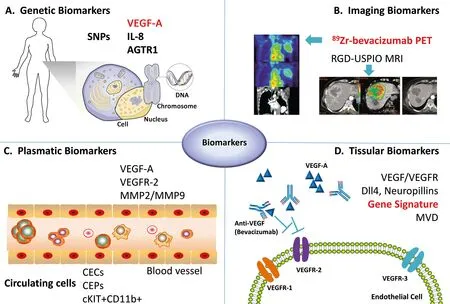
Figure 1 Overview of predictive biomarkers for bevacizumab efficacy in breast cancer. (A) Polymorphisms of several genes correlate with aberrant expression of critical proteins in angiogenic pathway; (B) Application of novel imaging methods allows in vivo tracing of bevacizumab perfusion in tumor tissues, and visualizing how they function on tumor; (C) Circulating angiogenic factors and endothelial cells promote neo-angiogenesis directly, and may serve as a noninvasive approach to assess angiogenic activities of tumors; (D)Combinations of multiple gene variables, tumor microvascular density or tumor characteristics profile the hallmark of breast cancer. SNP,single-nucleotide polymorphism; VEGF, vascular endothelial growth factor; IL-8, interleukin 8; AGTR1, angiotensin II receptor 1; RGDUSPIO, arginine-glycine-aspartic acid-labeled ultrasmall superparamagnetic iron oxide nanoparticles; VEGFR, vascular endothelial growth factor receptor; MMP, matrix metalloproteinases; CEC, circulating endothelial cell; CEP, circulating endothelial progenitor cell; Dll4,delta-like ligand 4; MVD, microvascular density.
Imaging methods to investigate BEV activity include dynamic contrast-enhanced magnetic resonance imaging(DCE-MRI) to assess perfusion (24,25) and positron emission tomography (PET) (26) to assess metabolic activity and hypoxia (Figure 1B). So far, the usefulness of PET as a predictor for BEV in BC was limited in small sample trials and animal model with BC xenografts (27-29).The predictive value of DCE-MRI for BEV had been shown years ago, but the results were inconsistent in different studies, and no followed data had shown whether this modality can be used to predict survival benefits with BEV (30-32). VEGF-A can be visualized noninvasively with PET imaging and using the tracer89Zr-labeled BEV.Gaykema and his colleagues investigated89Zr-BEV PET in primary BC patients (33). Tracer dosages of radio-labeled BEV can be used for tumor-specific, whole-body imaging of VEGF-A. Uptake of89Zr-BEV was visualized in 96.1%of the primary tumor lesions, and there was a relation with the level of VEGF-A in the tumor. This result provides proof that89Zr-BEV might be potentially valuable for prediction of the effect of VEGF-A — targeting therapeutics.
Recently, several studies of BC-bearing mice treated with BEV reported that new methods of magnetic iron oxide nanoparticles (IONP) MRI may be applicable for the in vivo monitoring of early antiangiogenic therapy effects (34-36). In a study by Kazmierczak et al., orthotopic human BC(MDA-MB-231) xenografts were imaged by αvβ3-integrintargeted, arginine-glycine-aspartic acid-labeled ultrasmall superparamagnetic iron oxide nanoparticles (RGDUSPIO) MRI before and after one-week therapy with BEV or placebo (34). Imaging results were validated by ex vivo multi-parametric immunohistochemistry (IHC). RGDUSPIO endothelial binding was significantly reduced after BEV, correspondingly, IHC revealed significantly lower αvβ3-integrin expression, microvascular density (MVD) and tumor cell proliferation, as well as significantly higher apoptosis in the therapy group. In contrast, morphologybased tumor response assessments did not show a significant intergroup difference in tumor volume.Although the observation is still limited in experimental BC, IONP-based MRI may be generating possible complementary molecular imaging biomarkers for BEV effect.
Diffuse optical spectroscopic imaging (DOSI) is a noninvasive imaging technology using near-infrared light to measure tissue hemoglobin concentration obtained from spectroscopic oxyhemoglobin (O2Hb) and deoxyhemoglobin (HHb) data, and directly visualizes vascularity and tissue oxygenation indicated from tHb (O2Hb+HHb)and stO2 (O2Hb/tHb), respectively (37,38). DOSI has been currently integrated into several clinical neoadjuvant studies that have explored hemodynamic biomarkers for predicting early treatment response (39,40). Ueda and his colleagues researched tumor oxygenation response after initiation of single-dose BEV followed by chemotherapy in seven BC patients. They found that tumor stO2 level could be a predictor of an additional benefit of BEV over that provided by paclitaxel and low tumor stO2 level predicted resistance to BEV (41).
From simply monitoring changes in vascular structure and function to tracing the drugs and visualizing how they function on tumor; the improvement of imaging methods will help us to know which one will be more effective as soon as the BEV was taken. Although all of these new methods to observe the response of antiangiogenic treatment are still in the experimental stage, they seem very promising to predict the short-time efficacy of BEV.
Circulating angiogenic factors of VEGF pathway
Many studies have measured circulating angiogenic factors to predict outcome of BC patients received BEV treatment(Table 2, Figure 1C). The choice of plasma levels of VEGFA (pVEGF-A) as a marker of benefit under BEV may seem straightforward, as it is the target for the drug, however,gauging its activity is a challenging issue. In AVADO trial,pVEGF-A and VEGFR-2 were proved to be potential predictive markers for BEV efficacy (9). In a recent metaanalysis including three BC trials of AVEREL, AVADO and BEATRICE, the pVEGF-A levels were assessed in 1,710 patients of total 3,751 patients enrolled in these trials. The patients with above median values of pVEGF-A had a 44% of improvement in disease control compared to with below median level (interaction P=0.02) (49). This meta-analysis polled the most patients with the assessment of pVEGF-A level, and positive results endorsed the hypothesis that pVEGF-A level could be a useful predictor to BEV therapy efficacy in BC. However, this study could not identify which specific length of pVEGF-A was measured. Another shortcoming was the lack of information of prognostic value of pVEGF-A, and it is probably relevant with predictive value. Optimal validation would require a prospective trial, randomizing or stratifying patients based on pVEGF-A levels to standard therapy BEV. A prospective stage III trial (MERiDiAN,GO25632) in HER2-negative MBC had been reported recently (42), 481 patients were stratified according to baseline pVEGF-A concentrations before randomization to weekly paclitaxel in combination with either BEV or placebo. The results of MERiDiAN do not support using baseline pVEGF-A to identify candidate benefitting most from BEV, the P value of interaction test is 0.4619. As the first trial prospectively evaluating pVEGF-A for a candidate biomarker of BEV efficacy, MERiDiAN trial represents major strengthes over all of retrospective biomarker analyses above. Collectively, this negative result may be the end to identify a single biomarker of pVEGF-A to predict BEV efficacy in MBC.
A phase II trial BEVERLY-2 reported that high serum levels of matrix metalloproteinases (MMP) 2 and MMP9 were associated with better survival in HER2-positive inflammatory breast cancer (IBC) patients treated with BEV- and trastuzumab-based neoadjuvant chemotherapy(43). MMP2 and MMP9 belong to the MMP family, which implicates in proteolysis of extra-cellular matrices,regulation of cell adhesion and migration, processing of growth factors and cytokines, and liberation of angiogenic factors (50). MMP2 and MMP9 have been reported to be involved in angiogenesis with different vascularization process, and the predictive value has been observed in recurrent high-grade glioma (51-55). In accordance with results of glioma, baseline MMP2 and MMP9 serum levels were associated with disease-free survival (DFS) and OS in the HER2-positive IBC patient population of the BEVERLY-2 trial: high baseline MMP2 and low baseline MMP9 were correlated to better DFS and OS and remained significant for improved DFS in multivariate analyses (43). Although BEVERLY-2 trial lacked a control group in a randomized design for investigate the predictive value of MMP2 and MMP9, the similar results observed in glioma and HER2-positive IBC reinforce the interest of these biomarkers as candidates for prediction of BEV activity.
Circulating cell biomarkers
Tumor angiogenesis driven by VEGF-A depends at least partly on the mobilization of circulating endothelial progenitor cells (CEPs), which integrate into growing tumors and contribute to the formation of a functional
vascular bed. Increased concentrations of CEPs may reflect active tumor angiogenesis. A few studies investigated whether circulating endothelial cells (CECs) and CEPs could serve as predictive markers for antiangiogenic therapies, and these findings were contradictive (48,56-58).However, a pilot study of MBC patients with first-line chemotherapy of paclitaxel combined with or without BEV demonstrated that the circulating KIT+/CD11b+ cell subpopulation decreased significantly under therapy with paclitaxel and BEV compared to paclitaxel only. This effect is specific, as three additional subpopulations of CD11b+cells (VEGFR1+, JAM1+, TIE2+) were not affected. BEV combining treatment also significantly decreased the levels of IL-10 mRNA in CD11b+ cell and IL-10 protein in plasma, which is a well-known immune suppressive M2 cytokine produced during cancer progression (59). Thus,BEV might provide therapeutic benefits by reversing M2-associated state of immunosuppression in addition to its anti-angiogenic effects, and this was consistent with VEGF pathway which also plays an important immunological role in breast cancer (2). It has been shown in vitro that mesenchymal stem cell-secreted IL-6 and VEGF may act as paracrine factors to sustain BC cell migration (60).These results suggested circulating KIT+/CD11b+ cells and IL-10 levels as candidate biomarkers of BEV activity in MBC, and that we may look into the immunological biomarkers for patients selecting BEV treatment as BEV may regulate the immune environment of cancer patients.Larger studies are needed to test this hypothesis.
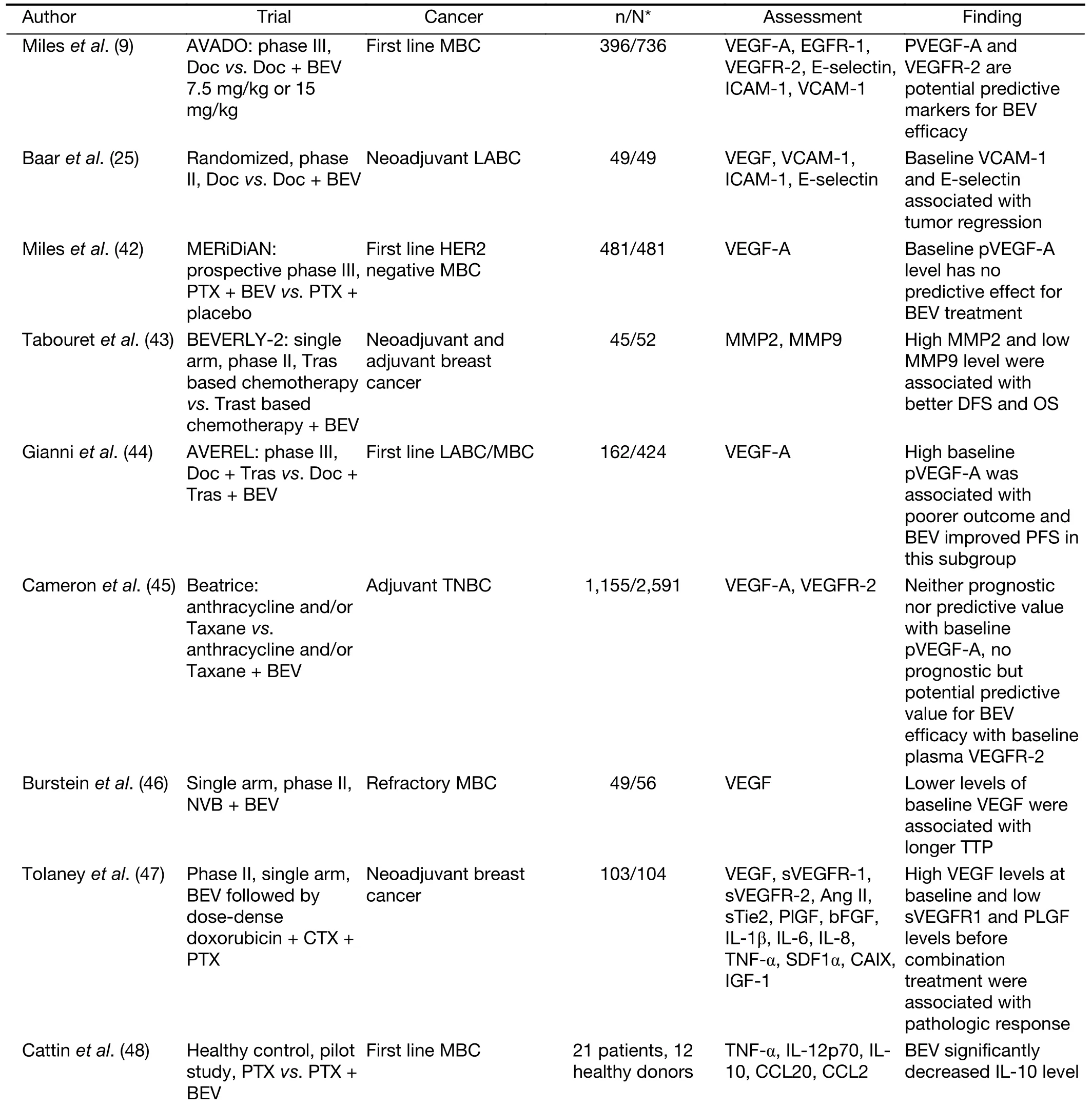
Table 2 Studies assessing serological biomarkers in relation to activity or efficacy of BEV
Angiogenic gene expression in situ
Numerous studies of gene expression in the VEGF pathway by tumor cells, inflammatory cells, endothelium,or tumor-associated stroma, tried to define the best biomarkers of response to BEV (Table 3, Figure 1D). A retrospective subset analyses on the AVF2119g phase III trial evaluated the expression of VEGF pathway components in available primary cancer tissue as predictors of benefit from BEV in MBC (61). This study suggested that expression of delta-like ligand 4 (Dll4), VEGF-C and neuropilin-1 (NRP1) showed trends toward improvement in PFS associated with the addition of BEV. Although the observations are not statistically significant after correction of multiple testing, correlation of low NRP1 expression and BEV effect was consistent with the early observing in gastric and colorectal cancer, which made NRP1 one of the most promising markers identified thus far. Besides translational research in phase III clinic trials, AGTR1 overexpression has been found associated with greater treatment response of BEV in several phase II studies(62,63).
DNA methylation is one of the known mechanisms of epigenetic regulation and its involvement is associated with the development of drug resistance (67,68). A certain methylation pattern in angiogenesis related genes could influence the response to an antiangiogenic therapy.Therefore, by using genome-wide methylation profiling, a recent study reported a nine genes methylation signature(PKNOX2, POLK, UNC119, SNRPN, TMBIM6, MLH1, and GNAS) may predict BEV efficacy in MBC (69). Due to numerous genes involved in angiogenesis process, a single biomarker seems unlikely to predict benefit from BEV.Recently, a spanish study analyzed a set of 168 genes related to angiogenesis, epithelial to mesenchymal transition (EMT) and inflammation on 60 patients treated with BEV and weekly paclitaxel (64). This study combined multiple clinical characteristics and gene variables into two models using the least absolute shrinkage and selection operator (LASSO) (70,71), for variable selection: one model with gene expression only (G-model), and the other included both gene expression and clinical variables (GCmodel). Finally the GC-model consisting of 13 genes (REL,FN1, NOTCH3, DDIT4, IL8, ADRBK1, FABP5, PLAU,HMBS, PTK2B, THBS1, SLC39A6, and TCF3) and five clinical variables (DFS, estrogen receptor, metastatic sites,prior anthracyclines and taxanes, and prior chemotherapy treatment for metastatic disease) obtained better accuracy with longer follow-up than G model or model of clinical variable only. Combination of gene profile and clinic characteristics might be a very reasonable predictor for BEV treatment as it will decrease maximum bias of single factor. Either the nine gene methylation signature or this GC-model should be evaluated in larger independent series in order to develop a routine clinical test to predict the benefit of BEV in MBC patients.
Neoadjuvant scenarios provide an opportunity of brief exposure to specific drugs for development of biomarkers.In a neoadjuvant trial of chemotherapy with addition of BEV, whole-transcriptome mRNA was performed in 132 HER2-negative untreated BC patients. After gene expression profiling and analysis of differential gene expression, the authors found highly expression of immune-related genes responding to antiangiogenic therapy, and to be a strong predictor to BEV, especially in luminal B subtype (72). Another retrospective study of
untreated BC patients from two phase II trials of neoadjuvant chemotherapy with carboplatin, nab-paclitaxel combined with BEV or trastuzumab reported that the transforming growth factor beta (TGF-β) signature was specifically predictive to BEV efficacy (65). Finally, the authors derived a 61-gene classifier by using this brief exposure with single run-in dose either nab-paclitaxel, BEV or trastuzumab, and serial biopsies from baseline and post brief exposure. They showed that a single dose of BEV resulted in down-regulation of a well-characterized TGF-β activity signature in every single breast tumor that achieved pCR (P≤0.004), and this predictive capacity is specific to BEV brief exposure as it is not able to predict response to nab-paclitaxel or trastuzumab. The research of associated mechanism suggested that there is a strong correlation between a reduction in tumor hypoxia and decrease in TGF-β pathway activity in tumors that respond to BEV. It has been reported that hypoxia leads to increased secretion of TGF-β ligand from mesenchymal stem cells in the stroma and has been shown to increase TGF-β activity in tumor cells, leading to EMT and drug resistance (73).Therefore, this result supported the effect of BEV on hypoxia leads to changes in TGF-β ligand secretion from the tumor stroma, leading to changes in TGF-β signaling in tumors. TGF-β signature may provide an early functional readout of pCR to preoperative BEV therapy in HER2-negative BC, thus the results require validation in prospective trials of anti-angiogenic therapies.
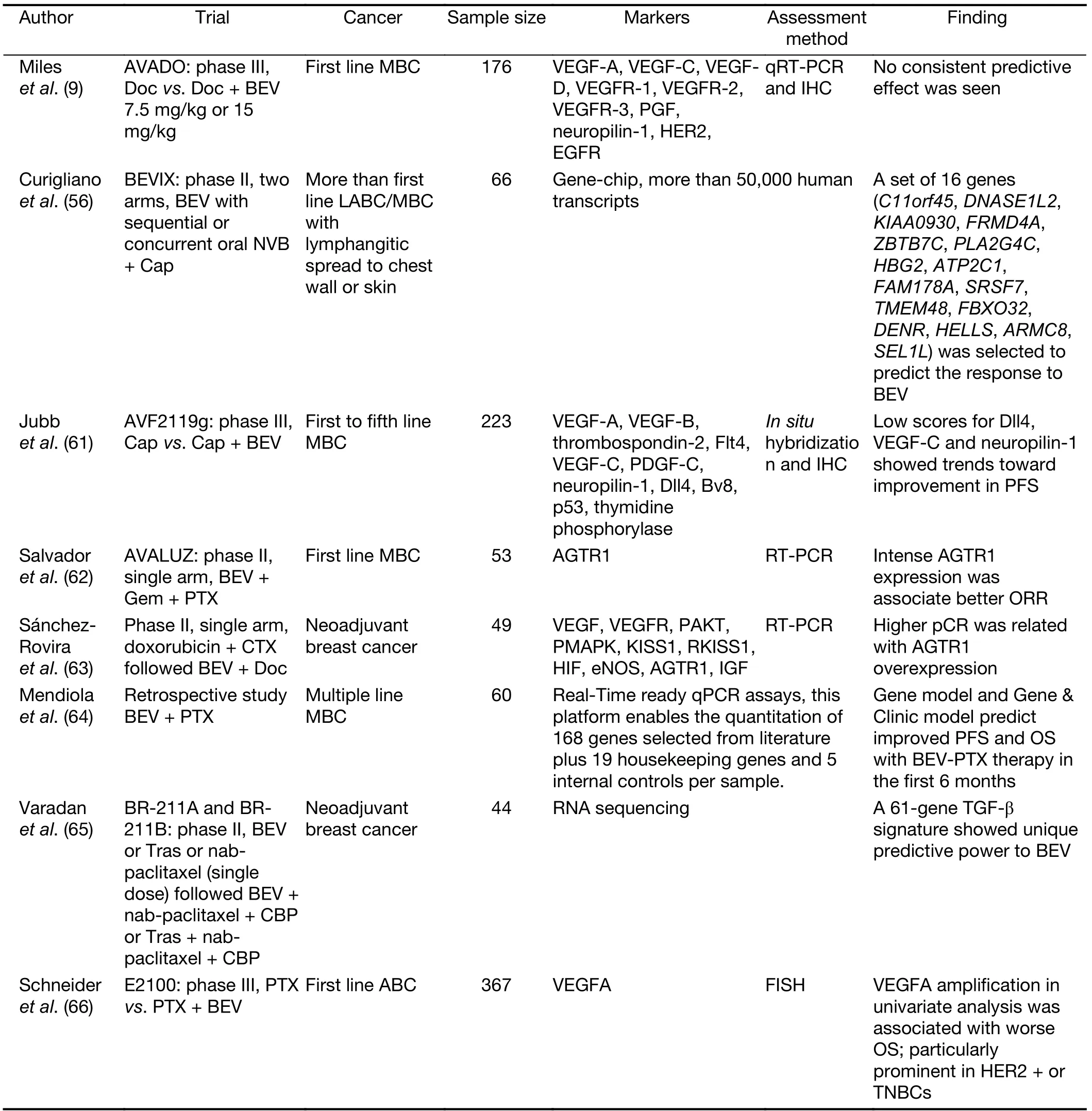
Table 3 Genetic markers evaluated as predictive biomarkers for BEV treatment
MVD
MVD is used to assess the neovascularization in tumors.High MVD or MVD surrogates commonly suggest poor prognosis of tumor, correlate with progression and metastasis, and predict clinical outcome (74,75). A large study of more than 800 BC patients showed that high MVD was significantly associated with DFS and OS (76).Some studies tried to evaluate the predictive effect of MVD to BEV. No correlations have been found between baseline MVD and response to BEV in most studies with the exception of one phase II trial in 20 BC patients (77,78).Recently, a phase II study of neoadjuvant BEV (single dose)followed by combination of BEV and chemotherapy in HER2-negative BC has found pretreatment MVD as a potential predictive biomarker of response to BEV in BC(47). This trial showed a higher rate of pCR in TNBC than in hormone receptor-positive (HR) BC that results from greater baseline MVD in TNBC compared to HRBC. The further research in this study proved that BEV reduces vessels only when sufficient numbers of vessels are initially present. Therefore, when they pooled high MVD HRBC and TNBC patients together, they found the relation between tumor regression and the change of pericytecovered MVD (a surrogate marker of vessel normalization)is in the same pattern. Hence, in TNBC and high-MVD HRBC patients with improved pCR, BEV induced vascular remodeling, which led to a higher density of normalized vessels. In addition, the assessment of circulating biomarkers in this study found that changes of soluble VEGFR-1 plasma level (a resistance biomarker associated with pericyte coverage) were inversely associated with tumor regression (79). BEV treatment seems less effective in BC than in other tumors. This study suggested the difference of baseline MVD across BC subsets may explain the various responses to BEV.
Conclusions
BC is a complex heterogeneous disease with a relatively prolonged course, and BEV was tested in metastatic,adjuvant, neoadjuvant BC. As the recent TURANDOT,and MERiDian trial suggest, BEV combined therapy is still a reasonable option in MBC management. The real challenge will be how best to use BEV in whole comprehensive management strategy for this disease, since more and more innovative drugs with new mechanism are introduced for MBC treatment. So far, all the clinical data seem that there is a trend that extended tumors, metastatic or locally advanced, are likely to benefit from BEV therapy in combination with cytotoxic drugs, assuming that a high level of tumor neo-angiogenesis, like in neoadjuvant and metastatic treatment, or in triple negative tumors, but not in adjuvant therapy, is the best target. It is difficult to understand why the improvement has seen in PFS or pCR with BEV not translated to an improvement in OS in the metastatic setting, or in DFS in the adjuvant setting, which seems a failure of patient selection rather than a general failure for the anti-VEGF hypothesis. All these confusing results underscore the urgent need to identify mechanistic biomarkers of response to BEV therapy.
The optimum biomarkers will predict OS, have high negative predictive value, demonstrate biological relevance to VEGF inhibition, and permit continuous assessment to identify evolving resistance. Biomarkers that meet these standards are essential if BEV remains a standard agent in the treatment of BC, in the face of competition from drugs that improve OS. So far, investigation in BEV predictors has not been for lack of trying. Trials examining anti-VEGF therapy in BC have been probed at both genomic and proteomic levels, and potential gene signature, SNPs,and protein candidates for assigning patients have been put forth. MERiDian trial as the first and only one prospective trial using such biology-driven approaches to validate putative biomarkers has failed to prove that baseline pVEGF is a predictor to BEV efficacy. But given the complexity of underlying angiogenic mechanisms, it seems unrealistic to expect a single biomarker to predict the benefit from anti-angiogenic therapy. Current researches on predictive biomarkers of BEV focus on two different possibilities. One possibility is tried to select the potential benefit population by the pretreated data, like polymorphisms in VEGF-pathway, high pretreated MVD level in BC, or gene signature of different combination.With the development of comprehensive genomic profiling, the combined biomarkers like gene signature, is always a hopeful and reasonable predictor. The other possibility is multiple assessments of the biomarker before and after BEV treatment, the early change of these biomarkers might predict the future efficacy of BEV.Molecular imaging like labeled BEV PET probably offers a visualized noninvasive way to foresee the efficacy, especially to predict the short-term response such as pCR, and they need more evidence to prove the predictive value to longterm response. The use of BEV in BC has hit the ceiling,one way to break through the ceiling is to identify predictive biomarkers. The present review showed that some inspiring results have been achieved, however, it is difficult to know how much closer we are to personalizing its use. We hope that clinical studies will be undertaken with the prospective use of these new interesting finding in this review for patient selection that will validate their predict value, and allow us to target the appropriate patients for BEV therapy.
Acknowledgements
None.
Footnote
Conflicts of Interest: The authors have no conflicts of interest to declare.
杂志排行
Chinese Journal of Cancer Research的其它文章
- Chinese guidelines for diagnosis and treatment of melanoma 2018 (English version)
- Association of cancer prevention awareness with esophageal cancer screening participation rates: Results from a populationbased cancer screening program in rural China
- FAT1, a direct transcriptional target of E2F1, suppresses cell proliferation, migration and invasion in esophageal squamous cell carcinoma
- Clinical significance of MET gene amplification in metastatic or locally advanced gastric cancer treated with first-line fluoropyrimidine and platinum combination chemotherapy
- A 18FDG PET/CT-based volume parameter is a predictor of overall survival in patients with local advanced gastric cancer
- Radiomics-based predictive risk score: A scoring system for preoperatively predicting risk of lymph node metastasis in patients with resectable non-small cell lung cancer