Endoscopic management of massive rectal bleeding from a Dieulafoy's lesion: Case report
2019-08-21MarioRenePinedaDePazMassielMadelinRosarioMorelJoseGuadalupeLopezFuentesLuisArielWallerGonzalezRodrigoSotoSolis
Mario Rene Pineda-De Paz,Massiel Madelin Rosario-Morel,Jose Guadalupe Lopez-Fuentes,Luis Ariel Waller-Gonzalez,Rodrigo Soto-Solis
Abstract
Key words: Dieulafoy's Lesion;Endoscopic hemostasis;Massive rectal bleeding;Case report
INTRODUCTION
Dieulafoy's lesions (DLs) represent less than 5% of all causes of gastrointestinal bleeding.These lesions were initially described as gastric aneurysms by Gallard in 1884,but it was in 1898 when George Dieulafoy,a French surgeon,identified them in three patients as the cause of gastrointestinal bleeding[1].More than 90% of the lesions are located at the upper gastrointestinal tract and only 2% are found at the rectum[2].Unlike the proximal lesions,rectal DLs (RDL) usually present hematochezia and/or fresh bleeding.The literature reveals only few case reports of RDL.We report the case of profuse lower gastrointestinal hemorrhage due to a RDL,as well as the proper literature review.
CASE PRESENTATION
Chief complaint
A 44-year-old female patient hospitalized in our institution due to a vascular access infection.
History of present illness
The patient presented profuse rectal bleeding that progressed to hypovolemic shock in four hours.
Past medical history
Her medical comorbidities included chronic kidney disease on replacement therapy and secondary hypertension.Patient denied any toxic habits.
Her surgical history included two cesarean sections,appendectomy,and livingdonor kidney transplant followed by acute rejection.Family history was negative for any gastrointestinal disease.
Physical examination
On presentation her vital signs were temperature of 36 °C,pulse of 120 bpm,respiratory rate of 20 rpm,blood pressure of 80/50 mmHg,and oxygen saturation of 92%.On general physical examination she looked pale and dehydrated.Abdominal examination revealed non-distended,soft,non-tender abdomen with normal bowel sounds.Rectal examination revealed bright blood with clots.The cardiovascular,pulmonary and neurological examination was unremarkable.
Laboratory examinations
Complete blood count analysis revealed hemoglobin of 6.7 g/dL,normal platelet count (193000/mm3),partial thromboplastin time of 42 s (RV 25-33),prothrombin time of 20 s (RV 11-15),and international normalized ratio 1.86.
Imaging examinations
Urgent colonoscopy findings were active bleeding from small bulgy vessel with minimal surrounding erosion and no ulcerative lesions (Figure 1).
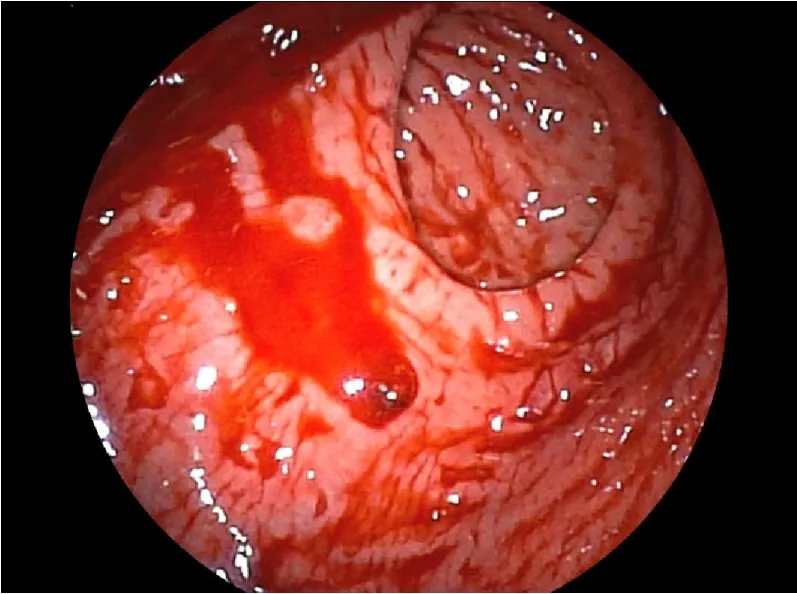
Figure1 Endoscopic appearance of Dieulfoy's lesion.
FINAL DIAGNOSIS
The final diagnosis of the presented case was a RDL.
TREATMENT
For the management of the hypovolemic shock,proper resuscitation with crystalloids,transfusion of packed red blood cells and vasoactive agents was performed.After hemodynamic stabilization,endoscopic therapy with two hemoclips (Figure 2) was done.
OUTCOME AND FOLLOW-UP
Immediate hemostasis was achieved with endoscopic management,and on the fifth day the patient was discharged.There were no signs of recurrent bleeding at thirty days of follow-up.
DISCUSSION
DLs represent an unusual cause of non-variceal gastrointestinal bleeding,accounting for less than 5% of all cases.More than 90% of these lesions are located at the esophagus,stomach and duodenum;only 2% are found at the rectum.The most relevant histological findings are aneurysm and inflammation,but a biopsy is not usually necessary[2].The reference standard for diagnosis is endoscopy.Common findings include a small,usually less than 3 mm,protruding pulsatile lesion surrounded by normal mucosa,with or without active bleeding[3].
Unlike the manifestations described in other parts of the digestive tract,RDL usually present with rectorrhagia or hematoquezia.There are previous case reports of profuse rectal bleeding,but most of them didn't evolve to hypovolemic shock as occurred with our patient.A computed tomography angiography was canceled due to hemodynamic instability in the CT-room.This hemodynamic instability can impact in the morbidity and mortality of these patients[4,5].
If technically feasible,the first line of treatment is endoscopic hemostasis.The European Gastrointestinal Endoscopy Society (ESGE) recommends endoscopic hemostasis for DLs,including: thermal coagulation,mechanical hemostasis(hemoclips or band ligation),or combined therapy (diluted adrenaline injection plus contact thermal or mechanical therapy)[6].These endoscopic hemostasis techniques are safe and have similar outcomes in observational studies.As in other causes of nonvariceal bleeding,there is superiority of combined,thermal and mechanical methods over injection monotherapy[6].Endoscopic treatment achieves an initial hemostasis rate > 93.6% of cases,with a rebleeding rate of 12.1%,including cases of RDL[7,8].A prospective study demonstrated superiority of mechanical endoscopic treatment with hemoclips or band ligation versus injection with diluted adrenaline[9].Regarding to the mechanical therapy,there is no differences in endoscopic band ligationvshemoclips.A meta-analysis that included 5 studies,compared endoscopic band ligation (75 patients) versus hemoclips (87 patients) for primary hemostasis of DLs;results didn't find any difference for the primary outcome [0.96 (95%CI: 0.88-0.99)vs0.91 (95%CI: 0.83-0.96),respectively];there were no differences in rebleeding rates neither [0.06 (95%CI: 0.02-0.15)vs0.17 (95%CI: 0.10-0.28),respectively][10].In our patient,there was no rebleeding after the initial effective hemostasis with the placement of two hemoclips.Table 1 shows a summary of endoscopic treatment modalities.

Figure2 Endoscopic management of Dieulafoy’s lesion.
Transcatheter angiographic embolization (TAE) should be the next option in cases that can't be treated endoscopically[6,11].Surgical resection should be reserved for selected cases that can't be treated with endoscopic or angiographic methods[6,12].
CONCLUSION
Rectal DLs represent a rare cause of lower gastrointestinal bleeding.Massive hemorrhage can increase the morbidity and mortality of these patients.Endoscopic management continues to be the reference standard in the diagnostic and therapeutic approach.Thermal,mechanical (hemoclip or band ligation),or combination therapy(adrenaline injection combined with thermal or mechanical therapy) should be considered the first choice for treatment.
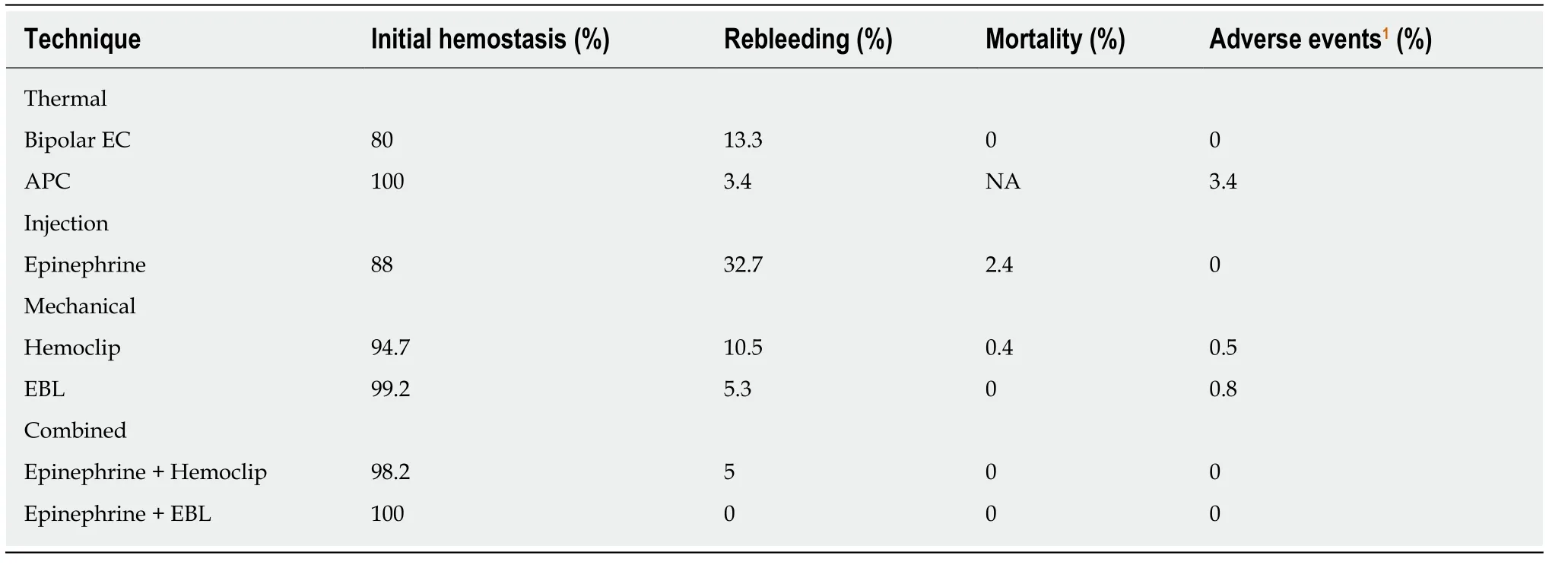
Table1 Endoscopic treatment modalities for Dieulafoy's lesion (modified from Nguyen et al[7])