Cost-analysis of inpatient and outpatient parenteral antimicrobial therapy in orthopaedics:A systematic literature review
2019-08-14ChristophKoljaBoesePhilippLechlerMichaelFrinkMichaelHacklPeerEyselChristianRies
Christoph Kolja Boese,Philipp Lechler,Michael Frink,Michael Hackl,Peer Eysel,Christian Ries
Abstract
Key words: Antibiotic therapy;Outpatient parenteral antibiotic therapy;Inpatient parenteral antibiotic therapy;Cost analysis;Periprosthetic joint infection;Parenteral
INTRODUCTION
There is a continuous increase in numbers of total joint arthroplasties (TJA) and an expansion of indications has been noted in recent years[1,2].In addition,predictions show a growing demand for the coming years[1,2].On the one hand,more older and multi-morbid patients undergo TJA,on the other hand,indications have been extended to younger and more active patients with high functional demands and longer life expectancy[1,2].Due to a general increase in life expectancy the consecutive risk for revision surgery rises.Every revision surgery is associated with a risk for infections as are co-morbidities (e.g.,diabetes mellitus,obesity,immune suppression)[3].Due to increasing numbers of joint replacements,a subsequent increase in numbers of periprosthetic joint infections (PPJI) can be expected.Treatment of PPJI usually consists of surgical intervention and a long-term antimicrobial therapy[4].Surgical intervention includes one-stage revision with either retention or revision of components in combination with debridement and irrigation.Alternatively,patients can undergo a staged revision with explantation of the prosthesis combined with debridement and irrigation and potentially reimplantation after several weeks to months.Both surgical principles are combined with antimicrobial treatment - mostly antibiotics[4,5].
Empiric antimicrobial therapy is followed by calculated therapy as soon as the pathogenic agent is identified and a resistogram is available.In PPJI,a bone-infection must be assumed and therefore antiinfective therapy lasts for several weeks (usually 6-12 wk)[4].Initially,antimicrobial therapy is started as parenteral therapy to achieve high plasma concentrations as well as sufficient concentrations in the targeted bone and joint as fast as possible (e.g.,time to peak serum concentration and peak serum concentration).Additionally,there are reports indicating an increase in multi-resistant bacteria.Here,extended parenteral antiinfective therapy is often required and no oral antibiotics are available.Another advantage of parenteral therapy is the fast(immediate) absorption and bio-availability of the drug.Potential risks of malabsorption do not occur.Usually,parenteral therapy requires an inpatient setting[Inpatient parenteral antibiotic therapy (IPAT)] due to monitoring,need for intravenous lines and administration of detergents by healthcare providers.This inpatient therapy goes along with high direct as well as indirect costs for the health system[6].An alternative to IPAT is outpatient parenteral treatment [Outpatient parenteral antibiotic therapy (OPAT)].To conduct a health economic cost-benefit analysis of OPAT,a detailed cost analysis of IPAT and OPAT is required.While calculation of direct costs hospital and outpatient settings is generally possible,there are no standards for methods and reporting.Additionally,exact cost-benefit analyses are a difficult endeavour as they should take into account direct cost savings (e.g.,hospital stay,physician visits,drugs and supplies,childcare,housekeeping,transportation,etc.) as well as indirect benefits (lost wages,both for patient and family members,etc.)[7].So far,there is a lack of knowledge regarding health economic effects of IPAT and OPAT for PPJI.
The aim of this study is an economic comparison of IPAT and OPAT.A systematic literature review was performed for this purpose.
MATERIALS AND METHODS
Systematic literature review
A systematic literature review was performed.Medline was searchedviaPubMed after a previous pilot-search to identify relevant search terms and strategies.The literature search and presentation of results followed the most recent version of the PRISMA guidelines (Preferred Reporting Items for Systematic Reviews and Meta-Analyses).A PRISMA checklist was used in a modified form for this study.This systematic literature review was registered in the international,prospective registry for systematic literature reviews (PROSPERO) at the Centre for Reviews and Dissemination of the University of York (York,United Kingdom) (No.71005).
Search strategy and screening
The exact search strategy using Medical Subject Headings (MeSH) is presented in Figure 1.Identified hits were entered into proprietary literature management software(EndNote v.7.7.1 for Mac).All articles were subsequently screened based on titles and abstracts.
Inclusion and exclusion criteria (screening/eligibility)
All studies reporting comparative costs of OPAT and IPAT were deemed eligible for inclusion in the systematic review.Exclusion was performed based on criteria outlined in Table 1.After screening,the full texts of all included articles were subjected to an in-depth analysis for inclusion and exclusion criteria.Finally,all eligible articles were stratified into five groups (Table 2).Studies were grouped into the highest possible category (A to E).Only category A studies were included into quantitative data analysis.Category B to E studies were used for background analysis and discussion.The inclusion process is depicted in Figure 2.
Statistical analysis
Extraction of data followed a standardized protocol.First authors,publication year,country of origin,study design,sample size,diagnosis,anti-infective therapy,costs of IPAT and OPAT and differences were extracted and entered into a digital spreadsheet.
RESULTS
The systematic literature search resulted in 524 hits for “outpatient parenteral antibiotic therapy”,570 hits for “outpatient parenteral anti-infective therapy”,and 514 for “outpatient parenteral antimicrobial therapy”.After deleting duplicates,619 potential studies of interest remained.Of these,328 were excluded based on title and abstract during screening.For the rest,215 full texts were available for in-depth analysis and 174 were categorized into group A-E.For quantitative analysis of OPAT and IPAT cost,21 studies were included (Table 3[8-28]).A detailed description of these studies can be found in Table 4[8-28].
Comparisons were performed based costs per day and costs per case.Table 5[8-28]shows costs per day and per case of IPAT and OPAT of included studies.
Five (24%) of the studies were performed in the United States,six (29%) in the United Kingdom,another five in the rest of Europe (24%) and the remainder in other countries.Except for one study,all showed relevant cost savings by OPAT compared to IPAT.Costs for IPAT were between 1.10 to 17.34 times higher than those for OPAT(Table 6[8-28]).
DISCUSSION
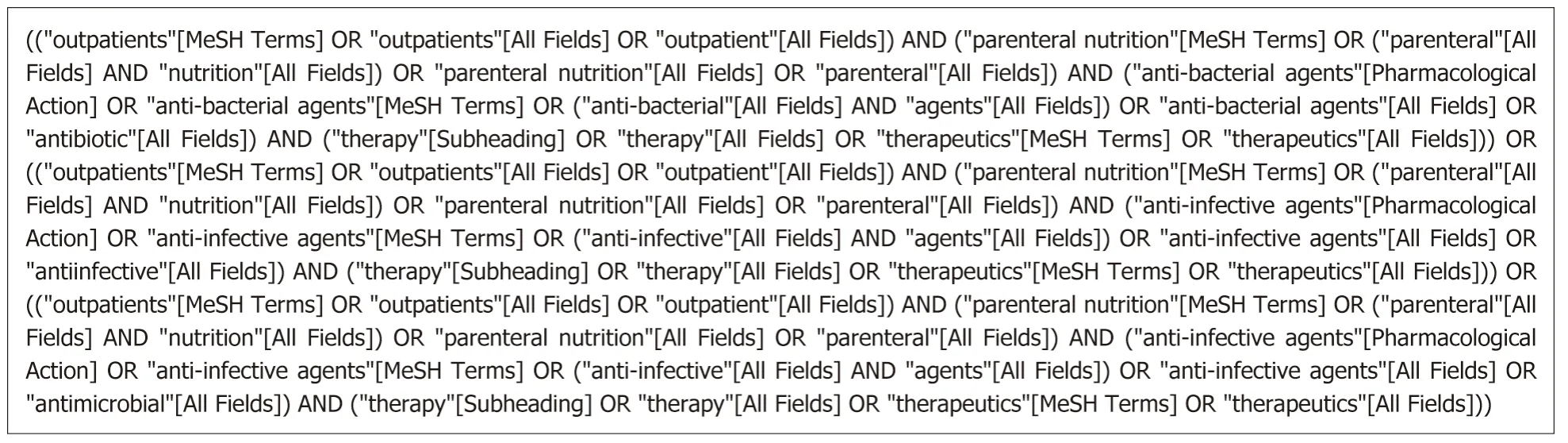
Figure1 Exact search strategy using Medical Subject Headings.
PPJI of large joints remains a multidisciplinary challenge.They are associated with significant socio-economic costs.Haddadet al[6]estimate the costs of PPJI to be approximately $1.62 billion (approx.€1.4 billion).Additionally,Parisiet al[29]used a Markov model including direct and indirect costs,and calculated costs per case to be$390000 to $474000 (circa €337000 to €409700).An increase in PPJI in recent years could be shown by the Nationwide Inpatient Sample[30].While 1104 cases were documented in 1990,a continuous increase was noted and reached 5838 cases in 2004.Interestingly,direct costs were stable at $55.000 per case.However,in the same timeframe,the length of hospital stay was significantly reduced from 22.2 to 7.6 d[30].Kurtzet al[31]performed a follow-up study and calculated costs of infected total knee arthroplasties until the year 2020.The authors estimated costs of $330 billion in 2011;reaching $527 billion in 2020.Interestingly,the costs per case were stable in the calculation.This estimation was supported by the study and thus highlights the relevance of PPJI[30,31].
利用SPSS 21.0软件统计两组患者治疗期间产生的数据,计量资料取(%)格式记录,统计学意义检验值为x2,结果显示P<0.05时,数据之间差异有统计学意义。
While avoiding PPJI is the best method to reduce costs,increasing numbers of total joint replacements makes this an illusionary aspiration.Occurrence of PPJI is associated with high costs and long-term therapy.By replacement of inpatient treatment with outpatient treatment,a significant cost reduction seems possible[32-34].Already in the 1970s,studies showed higher levels of patient satisfaction with OPAT in comparison to IPAT[8,35].Furthermore,no increase in risks and complications was noted by OPAT[36,37].
The first identified cost analysis with potential cost reduction were reported in the 1970s[9,38].Antoniskiset al[9]reported the first detailed outpatient antibiotic therapy in 1978.Cost structures of OPAT as well as IPAT showed significant variability.This may result from the large timeframe of the included studies.For example,studies of Antoniskiset al[9]and Grizzardet al[15]were much older than comparable studies from 2000 to 2017.To allow for a better comparison of studies,therapy costs were calculated for per-day-costs and transformed using the exchange rate for the mid of the year of publication.Correction for inflation was not performed.Additionally,analysis and interpretation of costs per case are severely influenced by individual cases and as such demonstrate immense heterogeneity.Thus,the analysis of costs per day was deemed more suitable for comparison.Costs per day ranged from €110 to€1125 for IPAT and from €28 to €269 for OPAT.Comparability is,however,restricted by specific peculiarities of each healthcare system.The complexity of the healthcare system in the United States adds to these limitations as does reimbursement in each of the included countries.The highest comparability was probably achieved in United Kingdom studies.Here,the NHS National Institute for Health Research supports OPAT research and therapy.This is highlighted by “The Community Intra Venous Antibiotic Study” (CIVAS) by Mintonet al[39].One part of this research project was a systematic literature review on economic aspects of OPAT[39].Cost-effectiveness was one of the five main research questions of the project and showed potential reduction in costs.Good acceptance of OPAT by patients and treating healthcare personnel was identified.Furthermore,safety and clinical effectiveness of OPAT were shown to be acceptable and comparable to IPAT.So far,no other comprehensive systematic literature review has been performed on cost comparisons of OPAT and IPAT.The aim of this study was the identification of costs of IPAT compared to OPAT.This systematic literature review identified 21 studies with sufficient information on costs of IPAT and OPAT.While the studies were published over a long time period (1978-2017) with wide geographical distribution,some generalized conclusions may be drawn.Here,the IPAT costs per day ranged from €110 to €1125 since 2001,OPAT costs were between €28 to €228.More comparable might be the ratio between IPAT and OPAT costs for each study.As shown in Table 6[8-28],the mean cost ratio was 3.6(1.0-10.4) per case and 4.8 (1.1-17.3) per day.Thus,the assumption of cost reduction by OPAT seems reasonable.Additional effects by indirect opportunity costs were not included in this study and might therefore increase the beneficial effect of OPAT.

Table1 Exclusion criteria for systematic literature review
Notably,all studies had some limitations in design and data analysis.Overall,all studies used simplified methods to calculate IPAT costs.OPAT costs were mostly calculated in a more complex fashion.Cost reductions were beneficial in most cases and most publications did not differentiate between cost-effects for payers/insurances and hospitals.Therefore,it cannot be conclusively demonstrated whether cost reductions led to reduced costs to the health care system (e.g.,insurance) or increased profit to the hospitals;mixed effects are possible as well.Additionally,the information regarding to PPJI was limited.Thirteen publications mentioned treatment of bone and joint infections (Table 7[9-11,13-15,17,18,20,21,23,25-28]).Of those,only two defined the affected bones or joints in detail.One study (Simset al[25]) specifically looked at PPJI of the hip and knee.Therefore,it was the only study to provide economic information for this particular subset of patients.
In the United States and the United Kingdom,OPAT is already well accepted.Efficacy and safety of OPAT was comparable to IPAT and associated with higher patient satisfaction (11,18-21).Still,in many countries (e.g.,Germany) there is none or only very limited availability of facilities to support OPAT.
In conclusion,a large number of publications on OPAT is available.Notably,there are only few reports on the specific subject of PPJI.Detailed analyses to support economical or clinical guidelines are therefore limited.This systematic literature review could identify only three studies that explicitly covered PPJI (category C)[32-34].Overall,OPAT showed comparable efficacy,safety and success rates as did IPAT.

Table2 Classification of publications

Table3 Details of included studies

Table4 Detailed description of costs of outpatient parenteral antibiotic therapy and inpatient parenteral antibiotic therapy depending on available information

Table5 Daily costs calculated in Euro for inpatient parenteral antibiotic therapy and outpatient parenteral antibiotic therapy (exchange rate based on mid of publication year)

Table6 Cost comparison (ratio) per case of outpatient parenteral antibiotic therapy vs inpatient parenteral antibiotic therapy

1Calculation simplified based on limited data.Calculations not applicable for two studies.A ratio above 1.0 indicates higher cost of inpatient parenteral antibiotic therapy in comparison to outpatient parenteral antibiotic therapy.IPAT:Inpatient parenteral antibiotic therapy;OPAT:Outpatient parenteral antibiotic therapy.
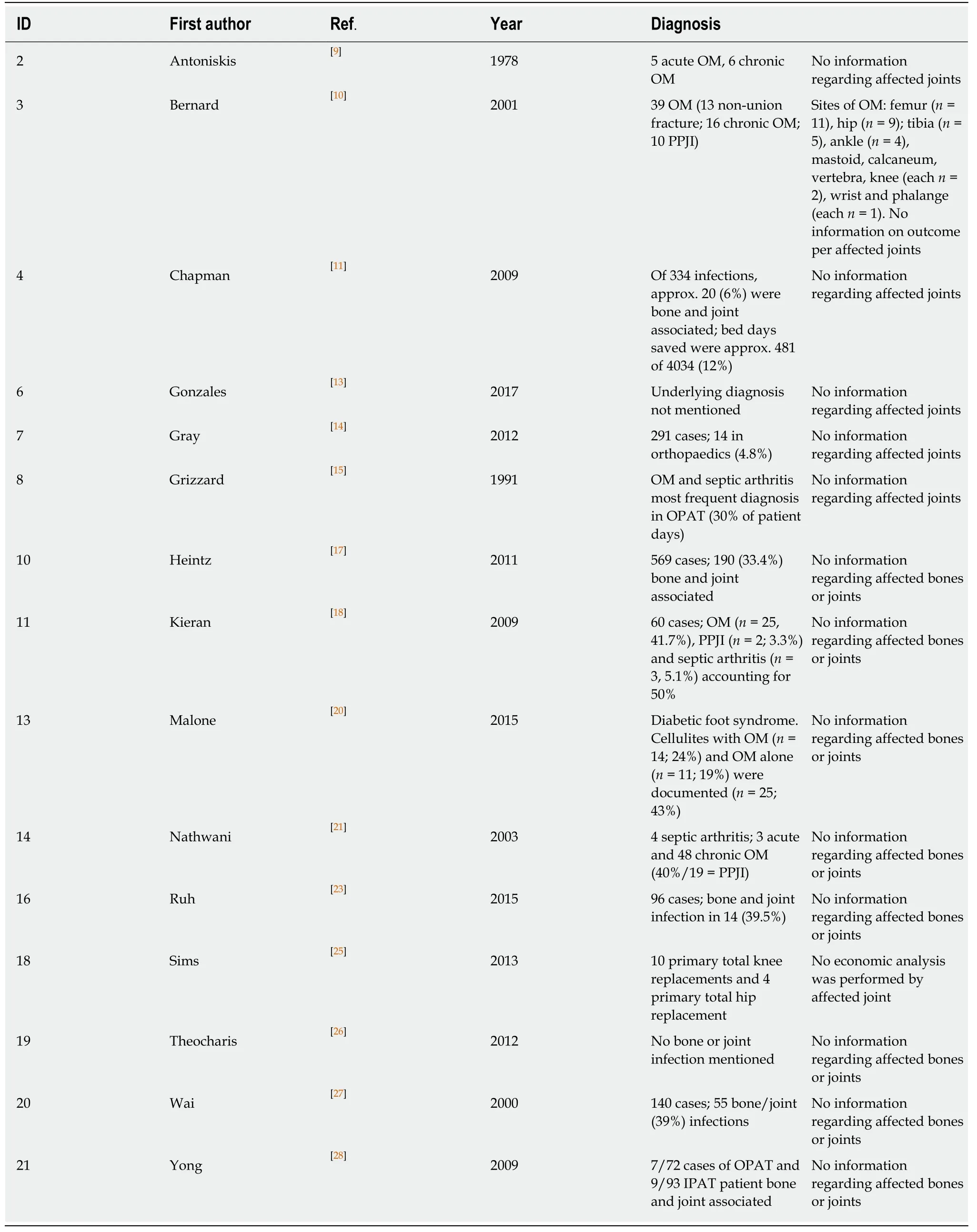
Table7 Literature details on bone and joint infections
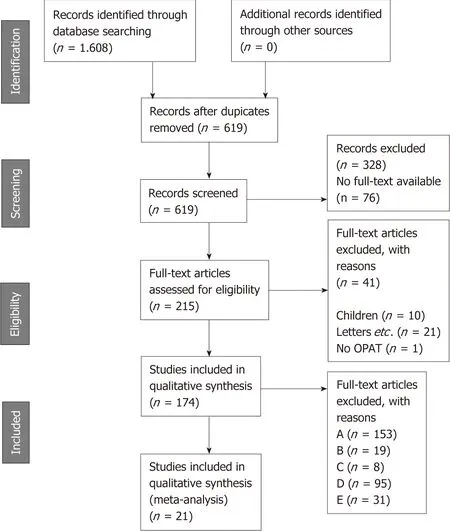
Figure2 Inclusion process depicted using the PRISMA Flowchart.
ARTICLE HIGHLIGHTS
Research background
Increasing numbers of total joint arthroplasties worldwide are noted.This is associated with rising risk for revision surgery.Periprosthetic joint infections (PPJI) play a significant role in revisions.Treatment of PPJI often requires long-term antimicrobial therapy.In PPJI,a boneinfection must be assumed and therefore antiinfective therapy lasts for 6-12 wk or longer.Parenteral antiinfective therapy is often required.Usually,parenteral therapy requires an inpatient setting [Inpatient parenteral antibiotic therapy (IPAT)] and goes along with high direct as well as indirect costs.An alternative is outpatient parenteral treatment [Outpatient parenteral antibiotic therapy (OPAT)].So far,there is a lack of knowledge regarding health economic effects of IPAT and OPAT in general and for PPJI specifically.
Research motivation
To identify the proposed economical benefits of OPAT in comparison to IPAT health economic cost-benefit analysis are needed.While various publications dealt with OPAT,generalization of assumptions requires input from multiple studies.We aimed to perform a systematic literature review of published literature on cost comparisons of OPAT and IPAT to better delineate the effects.The motivation was gen erating evidence to support OPAT for PPJI and create awareness f or this alternative treat men t option.
Research objectives
The aim of this study was an economic comparison of IPAT and OPAT.A systematic literature review was performed for this purpose.
Research methods
For this purpose,a search strategy was developed and we performed a systematic review of published literature by searching the Medline database via PubMed.All abstracts meeting the inclusion criteria were identified,and relevant articles were analyzed in detail.Relevant data was extracted and homogenized.
Research results
The literature search identified 619 potential studies of interest.328 were excluded during screening.215 full texts were available for in-depth analysis.For quantitative analysis of OPAT and IPAT cost,21 studies were included.Costs for IPAT were between 1.10 to 17.34 times higher than those for OPAT.Only one study showed marginally lesser costs for IPAT.Only one study focused specifically on PPJI.
Research conclusions
To the best of our knowledge,this is the first comprehensive systematic literature review outside the CIVAS report on cost effectiveness of OPAT.The review provides a wide overview over the exiting literature with minimal exclusion criteria.The presentation of extracted data allows for detailed understanding of included studies.Limitations of the study were the heterogeneity of studies from different health care systems and a wide time interval.Still,this open inclusion allows for better understanding of the available data worldwide.
Research perspectives
While the beneficial cost effect of OPAT has been shown,there is need to provide more specific studies.In particular,there is need to analyze cost structures for PPJI treatment in different health care systems.With such studies,guidelines to implement OPAT into the standard of care might be created.
猜你喜欢
杂志排行

World Journal of Clinical Cases的其它文章
- Diagnostic-therapeutic management of bile duct cancer
- Current status of the adjuvant therapy in uterine sarcoma:A literature review
- New treatment modalities in Alzheimer's disease
- Endoscopic ultrasound-guided fine-needle aspiration biopsy - Recent topics and technical tips
- Antiviral treatment for chronic hepatitis B:Safety,effectiveness,and prognosis
- Prevalence of anal fistula in the United Kingdom