The Relationship Between Mean Platelet Volume and ln-Hospital Mortality in Geriatric Patients with ST Segment Elevation Myocardial lnfarction Who Underwent Primary Percutaneous Coronary lntervention
2019-08-12meratroluMDMurtazaEmreDurakolugilMDseyinAvniUyduMDHakanDumanMDMustafaetinMDkselekMDandTuranErdoanMD
Ömer Şatıroğlu,MD ,Murtaza Emre Durako ğlugil,MD ,Hü seyin Avni Uydu,MD ,Hakan Duman,MD ,Mustafa Çetin,MD ,Yüksel Çiçek,MD and Turan Erdoğan,MD
1 Department of Cardiology,Faculty of Medicine,Recep Tayyip Erdoğan University,53100 Rize,Turkey
2 Department of Medical Biochemistry,Faculty of Medicine,Recep Tayyip Erdo ğ an University,53100 Rize,Turkey
Abstract
Objective: We planned to investigate the effect of mean platelet volume (MPV) on in-hospital mortality and coronary risk factors in geriatric patients with ST segment elevation myocardial infarction (STEMI) who underwent primary percutaneous coronary intervention (PCI).
Methods:We enrolled 194 consecutive STEMI patients.The study population was divided into two groups on the basis of admission MPVs.The high-MPV group ( n = 49) included patients in the highest tertile ( > 8.9 fL),and the low-MPV group ( n = 145) included patients with a value in the lower two tertiles ( ≤ 8.9 fL).Clinical characteristics,in-hospital mortality,cardiovascular risk factors,and outcomes of primary PCI were analyzed.
Results:The patients in the high-MPV group were older,more of them had three-vessel disease,and they had higher in-hospital mortality.Patients with in-hospital death were older,had higher Gensini score,creatinine concentration,and MPV,and had lower HDL cholesterol concentration.MPV,age,HDL cholesterol concentration,creatinine concentration,and Gensini score were found to be independent predictors of in-hospital death.
Conclusion:These results suggest that high admission MPV levels are associated with increased in-hospital mortality in geriatric patients with STEMI undergoing primary PCI.
Keywords:geriatric;ST segment elevation myocardial infarction;primary percutaneous coronary intervention;mean platelet volume;in-hospital mortality
lntroduction
ST segment elevation myocardial infarction (STEMI) is an important cause of morbidity and death.Inflammation has a major role in every stage of coronary artery disease (CAD) [1].
Treatment of acute coronary syndrome involves inhibition of platelet activity and thrombus formation.Platelets play a significant part during myocardial infarction by enhancing microvascular obstruction and secreting vasoactive peptides.Those in turn affect tissue perfusion and patency of the infarct-related artery (IRA) [2,3].Platelet reactivity is an important matter,and there is evidence that larger platelet size,measured as mean platelet volume (MPV),is associated with enhanced platelet activity [4,5].Higher MPVs are observed in patients with acute coronary syndromes compared with patients with stable angina or normal coronary arteries [6,7].Elevated MPV is associated with myocardial infarction and death [5].
There have been some reports regarding the prognostic value of MPV in geriatric patients with STEMI who underwent primary percutaneous intervention (PCI).We hypothesized that higher MPVs would be associated with in-hospital death following primary PCI in geriatric patients with STEMI.
Methods
Patient Population and Study Protocol
We included 194 consecutive patients with acute STEMI presenting at the Recep Tayyip Erdogan University Training and Research Hospital between December 2012 and May 2014 in this retrospective observational study.The inclusion criteria were as follows:electrocardiography revealing STEMI,which was defined as more than 30 minutes of continuous typical chest pain and ST segment elevation of 2 mm or more in two contiguous electrocardiography leads within 12 hours of symptom onset or up to 18 hours if there was evidence of continuing ischemia or hemodynamic instability.
The study population of 194 patients was divided into two groups on the basis of admission MPVs.Patients in the high-MPV group (n= 49) had an MPV in the third tertile ( > 0.89 fL),and patients in the low-MPV group (n= 145) had an MPV in the lower two tertiles ( ≤ 0.89 fL).
The demographic characteristics of the patients,cardiovascular history,and risk factors (hypertension,diabetes mellitus,smoking,hyperlipidemia) were obtained from medical records.We recorded the reperfusion time and door-to-balloon times.The exclusion criteria included the presence of renal failure (serum creatinine concentration greater than 1.5 mg/dL),chronic liver disease,chronic inflammatory disease,autoimmune syndromes,congenital heart disease,anemia,active infection,hematoproliferative disorders,chronic obstructive pulmonary disease,serious arrhythmia,hypothyroidism or hyperthyroidism,and active malignancy.
Biochemical Analyses
Venous peripheral blood samples for MPV and blood biochemistry tests were drawn before any treatment.Blood samples were collected in standardized tubes containing dipotassium EDTA,and all measurements were performed by an optical laser method with a Mindray BC-5800 analyzer.High-sensitivity troponin T was quantified with a cobas e 411 analyzer (Roche).A 12-lead electrocardiogram was recorded in each patient just after hospital admission,and the myocardial infarction type was obtained from the electrocardiogram.All biochemical measurements were performed by standard laboratory procedures.
Coronary Angiography,Primary Angioplasty,and Stenting
All patients received chewable 300 mg aspirin and clopidogrel (600 mg loading dose) before coronary angiography.Angiographic data of the patients were evaluated from catheter laboratory records.Emergency coronary angiography and angioplasty were performed via the percutaneous femoral approach.A nonionic,iso-osmolar contrast medium was used in all patients.The contrast medium was injected first into the artery that was presumed to be unobstructed.Blood flow in the IRA was graded according to the Thrombolysis in Myocardial Infarction (TIMI) classification [8].Heparin (100 IU/kg) was administered when the coronary anatomy was first defined.
After visualization of the left and right coronary arteries,nitrate was selectively injected into the IRA to rule out a possible coronary spasm if appropriate.Angiographic evaluation was done by visual assessment.Primary angioplasty (including balloon angioplasty and/or stent implantation) was performed only for the IRA according to the lesion type.For each procedure,success of the intervention was determined as reduction to less than 30% obstruction and stenosis of the IRA with TIMI 3 flow just after primary angioplasty.After angioplasty,the Gensini score was calculated [9] and all patients were admitted to the coronary care unit.Aspirin (100 mg per day) and clopidogrel (75 mg per day) use was continued in all patients.The use of glycoprotein IIb/IIIa inhibitors was left to the discretion of the interventional cardiologist.
Statistical Analysis
PASW Statistics for Windows (version 18.0,SPSS,Chicago,IL,USA) software package was used for all statistical calculations.Continuous variables are given as the mean ± standard deviation or median and as appropriate;categorical variables are given as percentages.Data were tested for a normal distribution by the Kolmogorov-Smirnov test.Student' sttest was used for the univariate analysis of normally distributed continuous numerical variables and the Mann-WhitneyUtest was used for nonnormally distributed numerical variables.Categorical variables were compared with the Pearson chi-square or Fisher exact test.The Spearman correlation coefficient was calculated to evaluate the association between two continuous variables.Variables with P < 0.05 were included in the logistic regression analyses with the “ enter” method.All tests of significance were two-tailed.Statistical significance was defined as P < 0.05.
Results
Baseline Characteristics
The baseline characteristics of the patients are presented in Table 1.Patients in the high-MPV group were older (80 ± 6 years vs.78 ± 4 years,P = 0.038) at admission than patients in the low-MPV group.The other remaining clinical characteristics were similar between the groups.Patients in the high-MPV group experienced higher in-hospital mortality (29 vs.15%,P = 0.037) than patients in the low-MPV group.
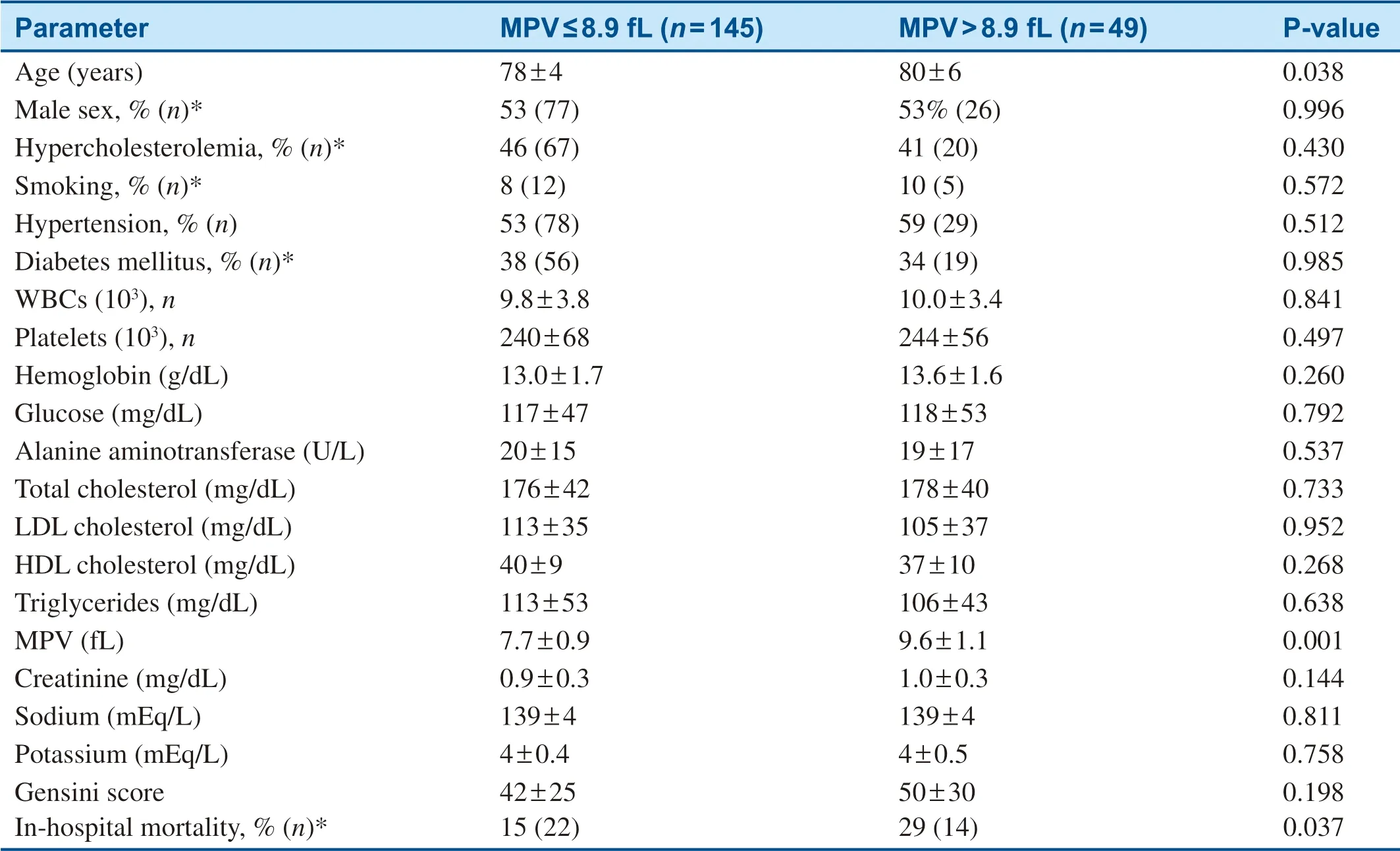
Table 1 Baseline Characteristics of the Study Population.
Angiographic and Procedural Characteristics
Angiographic and procedural characteristics of the two groups are detailed in Table 2.The proportions of culprit lesions and the TIMI flow rates were similar in the two groups.However,patients in the high-MPV group had more prevalent three-vessel disease ( Table 2).
The Relationship Between ln-Hospital Death and the Study Parameters
Patients with in-hospital death were older,had higher Gensini scores,creatinine concentrations,and MPVs,and had lower HDL cholesterol concentrations than patients who survived ( Table 3).
Multivariate Analysis
Multiple logistic regression analysis revealed MPV,age,creatinine concentration,HDL cholesterol concentration,and Gensini score to be independent predictors of in-hospital death ( Table 4).
Discussion
We demonstrated that high MPV is an important factor predicting increased in-hospital mortality in geriatric patients with STEMI undergoing primary PCI.Moreover,we revealed that mortality is also related to age,the extent of CAD as assessed by the Gensini score,and the degree of renal impairment as assessed by serum creatinine and HDL cholesterol concentrations following primary PCI.
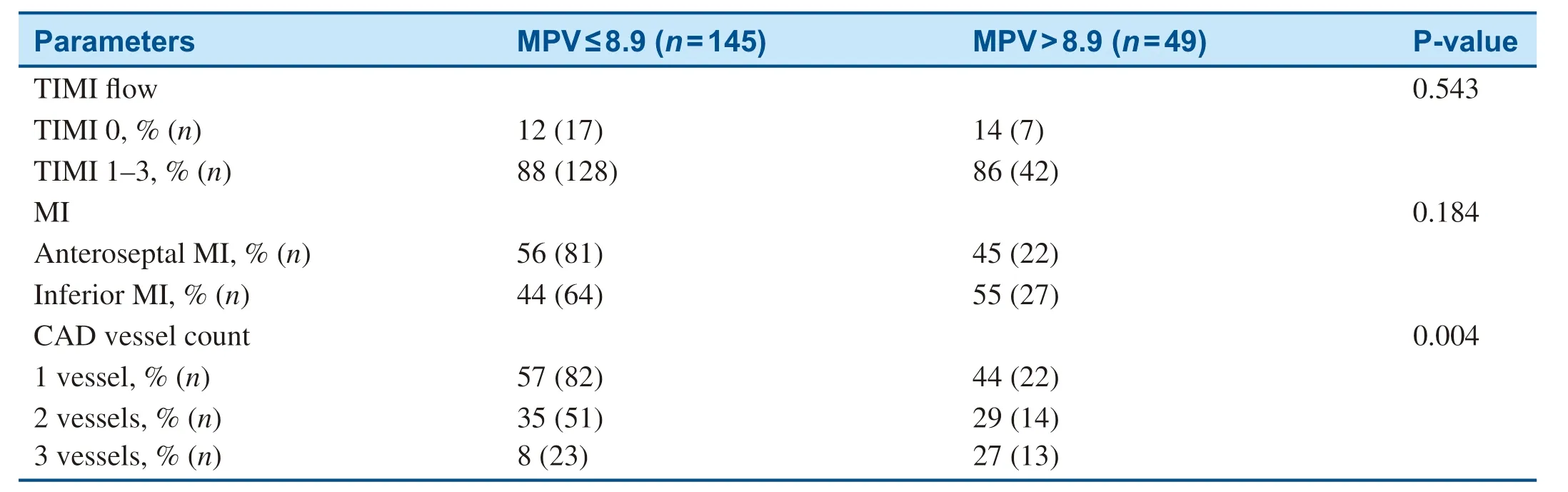
Table 2 Relationship Between Mean Platelet Volume (Mpv) and Thrombolysis in Myocardial Infarction (Timi) Flow,Location of Myocardial Infarction (MI),and Vessel Count.

Table 3 Relationship Between In-Hospital Death and Study Parameters.
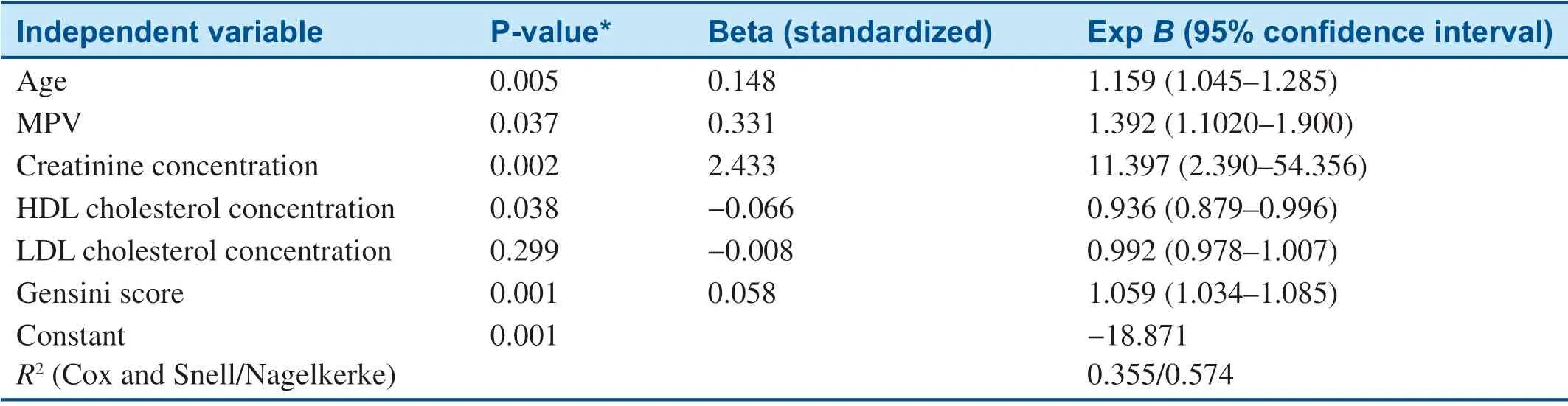
Table 4 Independent Predictors of In-Hospital Death.
The fact that high MPV in patients with STEMI undergoing primary PCI is associated with in- hospital death was previously demonstrated.Akgul et al.[10] revealed that high MPVs were related to higher 6-month cardiovascular mortality and 6-month all-cause mortality,in addition to higher in-hospital cardiovascular mortality.
Higher MPV may parallel the increased number of both platelet-leukocyte and platelet-platelet aggregates [11].Martin et al.[12] revealed that the highest quartile of MPV,measured 6 months after myocardial infarction,was associated with increased risk of death and recurrent ischemic events at the 2-year follow-up.
Elderly patients exhibit several differences from young patients with myocardial infarction [13].First,longer lifespan causes prolonged exposure to risk factors,which may cause more extensive CAD.Second,elderly patients with myocardial infarction tend to exhibit atypical symptoms such dyspnea,fatigue,and dizziness rather than angina.Lastly,elderly patients have longer admission times compared with younger patients,probably due to abnormalities in pain perception [14,15].Even though elderly patients may feel angina,the severity would be less than expected.Dysfunctions in the autonomic system,cerebral cortex,and sensory nerves may be responsible alone or in combination for increased pain threshold [16,17].
Previous studies documented similar success of primary PCI in elderly patients despite more extensive disease,more prevalent three-vessel disease,and comorbid conditions [18,19].However,as we observed in our study,more complex CAD,longer delay to hospital admission,and higher MPV increase in-hospital mortality in this special subgroup.Feliciano et al.[19] investigated the effect of primary PCI in patients aged more than 75 years and in a younger group.Even though the success rate of primary PCI was similar in both groups,elderly patients had higher mortality.
We documented that MPV is a significant predictor of in-hospital death.Patients with higher MPV have increased levels of platelet granules,microparticles,and receptors.Platelets have a major role in the pathogenesis of acute coronary syndromes.Since platelets are consumed during myocardial infarction,bone marrow produces and releases new platelets to the circulation.The association of MPV with platelet activation and aggregation and subsequent acute coronary syndromes has already been shown [20,21].MPV,a simple and reliable indicator of platelet functions,has been demonstrated to be larger in patients with CAD compared with normal individuals [22].There is long-standing evidence regarding the role of MPV in acute coronary syndromes [23].MPV has been identified as an independent predictor of poor angiographic reperfusion and 6-month mortality in patients with STEMI who underwent primary PCI [24].
Reperfusion injury may have affected our results as well.Since we know that cooperation among platelets,leukocytes,and endothelial cells is important in atherosclerosis and in maintenance of blood flow in both healthy and diseased vascular segments,increased MPV and leukocyte count in patients with STEMI implies that these cells may participate in reperfusion injury,either alone or in combination.Leukocytes and platelets may mediate reperfusion injury in different pathways.Plugs formed by leukocyte or platelet aggregates,or combined complexes,may hinder coronary blood flow,especially in the microvessels [25].Evidence demonstrated that platelets and neutrophils act synergistically in provoking postreperfusion cardiac dysfunction and that this may be largely due to cellto-cell interactions mediated by P-selectin [26].Platelets may also create impairment in reperfusion through secretion of inflammatory,vasoconstrictor,and prothrombotic mediators,thus increasing reperfusion injury [27].
We demonstrated higher creatinine levels and a higher Gensini score are associated with in- hospital death.The effect of increased creatinine concentration on long-term mortality in patients with STEMI following primary PCI has been demonstrated [28].A recent study confirmed increased in-hospital mortality and major adverse cardiovascular events in patients with impaired renal functions [29].Previous studies identified that coronary lesion complexity has been associated with higher short-term mortality since the thrombolytic era [30].Similarly,low levels of HDL cholesterol,a known independent risk factor for increased cardiovascular events,were related to significantly higher risk of in-hospital death in a large registry of STEMI patients [31].
Our study has several limitations.Mainly,the study population was relatively small.Moreover,our study is retrospective and observational.Thus,we cannot infer causality.However,we included a specific patient group and investigated in-hospital mortality,which is a solid end point.
Conclusion
Our results suggest that a high admission MPV is associated with increased in-hospital mortality in geriatric patients with STEMI undergoing primary PCI.
Conflict of lnterest
The authors declare that they have no conflicts of interest.
REFERENCES
1.Hansson GK.Inflammation,atherosclerosis,and coronary artery disease.N Engl J Med 2005;352:1685- 95.
2.Davi G,Patrono C.Platelet activation and atherothrombosis.N Engl J Med 2007;357:2482- 94.
3.Meadows TA,Bhatt DL.Clinical aspects of platelet inhibitors and thrombus formation.Circ Res 2007;100:1261- 75.
4.Van der Loo B,Martin JF.A role for changes in platelet production in the cause of acute coronary syndromes.Arterioscler Thromb Vasc Biol 1999;19:672- 9.
5.Chu SG,Becker RC,Berger PB,Bhatt DL,Eikelboom JW,Konkle B,et al.Mean platelet volume as a predictor of cardiovascular risk:a systematic review and meta-analysis.J Thromb Haemost 2010;8:148- 56.
6.Cameron HA,Phillips R,Ibbotson RM,Carson PH.Platelet size in myocardial infarction.Br Med J (Clin Res Ed) 1983;287:449- 51.
7.Pizzulli L,Yang A,Martin JF,Luderitz B.Changes in platelet size and count in unstable angina compared to stable angina or non-cardiac chest pain.Eur Heart J 1998;19:80- 4.
8.Chesebro JH,Knatterud G,Roberts R,Borer J,Cohen LS,Dalen J,et al.Thrombolysis in Myocardial Infarction (TIMI) trial,phase I:a comparison between intravenous tissue plasminogen activator and intravenous streptokinase.Clinical findings through hospital discharge.Circulation 1987;76:142- 54.
9.Gensini GG.A more meaningful scoring system for determining the severity of coronary heart disease.Am J Cardiol 1983;51:606.
10.Akgul O,Uyarel H,Pusuroglu H,Gul M,Isiksacan N,Turen S,et al.Prognostic value of elevated mean platelet volume in patients undergoing primary angioplasty for ST-elevation myocardial infarction.Acta Cardiol 2013;68:307- 14.
11.Tsiara S,Elisaf M,Jagroop IA,Mikhailidis DP.Platelets as predictors of vascular risk:is there a practical index of platelet activity? Clin Appl Thromb Hemost 2003;9:177- 90.
12.Martin JF,Bath PM,Burr ML.Influence of platelet size on outcome after myocardial infarction.Lancet 1991;338:1409- 11.
13.Gregoratos G.Clinical manifestations of acute myocardial infarction in older patients.Am J Geriatr Cardiol 2001;10:345- 7.
14.Haase KK,Schiele R,Wagner S,Fischer F,Burczyk U,Zahn R,et al.In-hospital mortality of elderly patients with acute myocardial infarction:data from the MITRA (Maximal Individual Therapy in Acute Myocardial Infarction) registry.Clin Cardiol 2000;23:831- 6.
15.Guagliumi G,Stone GW,Cox DA,Stuckey T,Tcheng JE,Turco M,et al.Outcome in elderly patients undergoing primary coronary intervention for acute myocardial infarction:results from the Controlled Abciximab and Device Investigation to Lower Late Angioplasty Complications (CADILLAC) trial.Circulation 2004;110:1598- 604.
16.Norgaz T,Hobiko lu G,Aksu H,Esen A,G ü l M,Ö zer HO,et al.The relationship between prehospital delays of patients with ST-elevation acute myocardial infarction and clinical,demographic,and socioeconomic factors:importance of patient education.Turk Kardiyol Dern Ars 2005;33:39227.
17.Miller PF,Sheps DS,Bragdon EE,Herbst MC,Dalton JL,Hinderliter AL,et al.Aging and pain perception in ischemic heart disease.Am Heart J 1990;120:22- 30.
18.Yazici HU,Durak MI,Ulus T,Temel K,Nasifov M,Nadir A,et al.The effect of aging on outcomes of primary percutaneous coronary intervention in patients with acute myocardial infarction.Turk J Geriatr 2012;15:255- 9.
19.Feliciano J,Fiarresga AJ,Timoteo AT,Pelicano N,Cacela D,Ferreira R,et al.Primary coronary angioplasty in the elderly.Rev Port Cardiol 2005;24:205- 14.
20.Ross R.Atherosclerosis - an inflammatory disease.N Engl J Med 1999;340:115- 26.
21.Oylumlu M,Dogan A,Ercan S,Kilit C,Amasyali B.The relationship between TIMI flow grade and hematological parameters in patients with ST-segment elevation myocardial infarction who underwent primary percutaneous coronary intervention.Gaziantep Med J 2014;20:165.
22.Bath PM,Butterworth RJ.Platelet size:measurement,physiology and vascular disease.Blood Coagul Fibrinolysis 1996;7:157- 61.
23.Kishk YT,Trowbridge EA,Martin JF.Platelet volume subpopulations in acute myocardial infarction:an investigation of their homogeneity for smoking,infarct size and site.Clin Sci (Lond) 1985;68:419- 25.
24.Huczek Z,Kochman J,Filipiak KJ,Horszczaruk GJ,Grabowski M,Piatkowski R,et al.Mean platelet volume on admission predicts impaired reperfusion and longterm mortality in acute myocardial infarction treated with primary percutaneous coronary intervention.J Am Coll Cardiol 2005;46:284- 90.
25.Engler RL,Schmid-Schonbein GW,Pavelec RS.Leukocyte capillary plugging in myocardial ischemia and reperfusion in the dog.Am J Pathol 1983;111:98- 111.
26.Lefer AM,Campbell B,Scalia R,Lefer DJ.Synergism between platelets and neutrophils in provoking cardiac dysfunction after ischemia and reperfusion:role of selectins.Circulation 1998;98:1322- 8.
27.Aziz KA,Cawley JC,Treweeke AT,Zuzel M.Sequential potentiation and inhibition of PMN reactivity by maximally stimulated platelets.J Leukoc Biol 1997;61:322- 8.
28.Yamaguchi J,Kasanuki H,Ishii Y,Yagi M,Nagashima M,Fujii S,et al.Serum creatinine on admission predicts long-term mortality in acute myocardial infarction patients undergoing successful primary angioplasty:data from the Heart Institute of Japan Acute Myocardial Infarction (HIJAMI) Registry.Circ J 2007;71:1354- 9.
29.Polanska-Skrzypczyk M,Karcz M,Bekta P,Kepka C,Przyluski J,Kruk M,et al.Prognostic value of renal function in STEMI patients treated with primary PCI:ANIN Registry.Br J Cardiol 2013;20:65.
30.Gibson CM,Bigelow B,James D,Tepper MR,Murphy SA,Kirtane AJ,et al.Association of lesion complexity following fibrinolytic administration with mortality in ST-elevation myocardial infarction.Am J Cardiol 2004;94:108- 11.
31.Ji MS,Jeong MH,Ahn YK,Kim YJ,Chae SC,Hong TJ,et al.Impact of low level of high-density lipoprotein-cholesterol sampled in overnight fasting state on the clinical outcomes in patients with acute myocardial infarction.J Cardiol 2015;65:63- 70.
杂志排行
Cardiovascular Innovations and Applications的其它文章
- Selective Coronary Angiography Following Cardiac Arrest
- Systemic Vasculitis:An Important and Underestimated Cause of Malignant Hypertension
- Predictive Value of Resting Pd/Pa for Fractional Flow Reserve Assessed with Monorail Pressure Microcatheter in Real-World Practice
- Ultrasound:The Potential Power for Cardiovascular Disease Therapy
- Giant Aneurysm of a Coronary-Pulmonary Artery Fistula:A Rare Cause of a Diastolic Murmur
- Superior Vena Cava Occlusion as a Complication of Transvenous Cardiac Device Implantation:A Case Report and Brief Review