Diabetes Mellitus and Stable Ischemic Heart Disease
2019-08-03CodySchwartzDOandDavidWinchesterMD
Cody Schwartz,DO and David Winchester,MD
1 Malcom Randall VAMC,1601 SW Archer Rd 111-D,Gainesville,FL 32608,USA
Abstract
Keywords:ischemic heart disease;diabetes mellitus;noninvasive testing
Introduction
In 2015 it was estimated that 30.3 million Americans(9.4% of the population)had diabetes mellitus(DM)[1].The substantial majority(30.2 million)are adults aged 18 years or older,of whom 7.2 million(23.8%)were not aware of their diagnosis[1].Prevalence increases with age:25.2% of those aged 65 years or older have DM[1].The overall prevalence of DM increased from 0.93 in 1958 to 6.3% in 2008 and then to 9.4% in 2015[1,2].One contributor to the increased prevalence of DM may be the change in the criteria for diagnosing DM.In 1979 the criteria included a fasting plasma glucose level of 140 mg/dL or greater,2-hour plasma glucose level on an oral glucose tolerance test of 200 mg/dL or greater,or both[3].In 1997 the criterion for diagnosing DM was a fasting plasma glucose level of 126 mg/dL or greater,or casual plasma glucose level of 200 mg/dL or greater,or 2-hour plasma glucose level on an oral glucose tolerance test of 200 mg/dL or greater[4].In 201 1 the American Diabetic Association revised the criteria for diagnosing DM to incorporate hemoglobin A1cvalues.These criteria included a hemoglobin A1cfraction of 6.5% or greater,for which the test should be performed in a laboratory by a method that is National Glycohemoglobin Standardization Program certif ed and standardized to the Diabetes Control and Complications Trial reference assay[5].
Projections of DM Prevalence
Current projections are that DM prevalence will continue to increase for decades,from a current rate of 21-33% by 2050.The continued growth is attributed to several factors,including aging of the population,an increase in higher-risk minority populations,and declining mortality among people with chronic illnesses,such as DM[6].Among patients with DM,cardiovascular disease(CVD)is a principal cause of death.In 2004,heart disease was the primary cause of DM-related death in 68% of people and stroke was the cause of DM-related death in an additional 16%[7].Adults with DM have heart disease and stroke death rates about two to four times the rates of adults without DM[7].
Risk of DM Patients Developing Stable Ischemic Heart Disease
Persons with DM are at higher risk of developing stable ischemic heart disease(SIHD)by several mechanisms,including a higher incidence of f ssured plaques,increased blood viscosity,enhanced platelet aggregation,increased synthesis of thromboxane A2,relatively elevated f brinogen levels,increased levels of factor VIII and f brinopeptide A,impaired endothelial function,and impaired endogenous f brinolysis[8].The endothelial dysfunction seen in DM stems from the metabolic abnormalities that characterize DM,particularly hyper glycemia,altered free fatty acid metabolism,and insulin resistance,that provoke molecular mechanisms altering the function and structure of blood vessels.These include increased oxidative stress,disturbances of intracellular signal transduction(such as activation of protein kinase C),and activation of the receptor for advanced glycation end products[8].
These changes result in decreased availability of nitric oxide,increased production of endothelin 1 and angiotensin II,activation of transcription factors such as nuclear factor κ B and activator protein 1,and increased production of prothrombotic factors such as tissue factor and plasminogen activator inhibitor 1.Decreased availability of nitric oxide along with increased production of endothelin 1 and angiotensin II leads to vasoconstriction,hypertension,and vascular smooth muscle cell growth.Activation of nuclear factor κ B and activator protein 1 causes inf ammation and leads to increased numbers of chemokines,cytokines,and cell adhesion molecules.Decreased nitric oxide kevels and increased production of tissue factor and plasminogen activator inhibitor 1 lead to thrombosis,hypercoagulation,and platelet activation,all of which promote endothelial dysfunction and increase the risk of SIHD[8].
Mortality Associated with CV Events in Patients with DM
When patients with DM do have a cardiovascular(CV)event,such as an acute coronary syndrome(ACS),their mortality is substantially higher than that among patients without DM.Donahoe et al.[9]showed this in data from a secondary analysis of studies by the Thrombolysis in Myocardial Infarction study group.They pooled data on patients with ACS from 11 clinical trials from 1997 to 2006,including 62,036 patients(46,577 with ST-elevation myocardial infarction[STEMI]and 15,459 with unstable angina[UA]/non-ST-elevation myocardial infarction[NSTEMI]).Overall,10,613 patients(17.1%)had DM.A multivariable model was constructed to adjust the data for baseline characteristics,aspects of presentation,and treatments for the ACS event.They found that mortality was signif cantly higher among patients with DM than among patients without DM at 30 days following either UA/NSTEMI(2.1 vs.1.1%)or STEMI(8.5 vs.5.4%).Similar results at 1 year showed mortality was signif cantly higher among patients with DM presenting with either UA/NSTEMI(7.2 vs.3.1%)or STEMI(13.2 vs.8.1%).By 1 year following ACS,patients with DM presenting with UA/NSTEMI had a risk of death that approached that of patients without DM presenting with STEMI(7.2 vs.8.1%).
Risk Stratifi cation and Evaluation of a Diabetic Patient
Because of the increased CV risk associated with DM,all DM patients are considered to be at high risk,def ned as greater than 10% CVD event risk at 10 years.Similarly to the general population,further risk ref nement can be made both through clinical assessment and with a variety of tests and procedures.Clinical CV risk factors in common between DM patients and the general population include a history of or current use of tobacco,noncoronary vascular disease,renal disease,age,sex,and family history of early onset coronary artery disease.Noninvasive testing options include both functional tests(left ventricular function,exercise testing,stress imaging)and anatomic imaging(coronary calcium scoring,cardiac computed tomographic angiography[CCTA],coronary angiography).These additional tests must be considered in the context of the individual patient for whom they are ordered.For example,testing recommendations for patients with symptoms suggestive of SIHD are very dif ferent from testing recommendations for asymptomatic patients.Another key factor is whether or not the patient already has established SIHD.
The Diabetic Patient with no Ischemia Symptoms and No Evidence of Coronary Artery Disease
While CVD is the major cause of death in patients with DM,the utility of screening patients with type 2 DM for SIHD continues to be controversial.The Detection of Ischemia in Asymptomatic Diabetics study was a randomized trial of CV testing in DM patients.In this study,1123 participants with DM and no symptoms were randomly assigned to be screened with adenosine-stress radionuclide myocardial perfusion imaging(MPI)or not to be screened.Both groups received standard-of-care treatment for DM and prevention for SIHD.Participants were recruited from DM clinics and practices and prospectively followed up from August 2000 to September 2007.The rates of CV events were not dif ferent between the two groups:seven nonfatal myocardial infarctions(MIs)and eight cardiac deaths(2.7%)occurred among the screened group and ten nonfatal MIs and seven cardiac deaths(3.0%)occurred among the not-screened group(hazard ratio 0.88,95% conf dence interval 0.44-1.88,P=0.73).The positive predictive value for CV events after moderate or large MPI defects were found was only 12%.The results are limited by the fact that the CV event rates were low,only 2.9% over a mean follow-up of 4.8 years,for an average of 0.6% per year.In this contemporary study population of patients with DM,the cardiac event rates were low and were not signif cantly reduced by MPI screening for myocardial ischemia over 4.8 years[10].
The similarly designed FACTOR-64 study tested the value of screening DM patients for SIHD,this time with CCTA.In this randomized clinical trial,900 patients with type 1 or type 2 DM and without symptoms of coronary artery disease(CAD)were enrolled and randomly assigned to receive SIHD screening with CCTA(n=452)or standard national guidelines-based optimal DM care(n=448).Unlike in the Detection of Ischemia in Asymptomatic Diabetics study,the investigators were directed to achieve specif c care tar gets(for standard therapy,hemoglobin A1clevel below 7.0%,low-density lipoprotein cholesterol level below 100 mg/dL,systolic blood pressure below 130 mmHg;for aggressive therapy,hemoglobin A1clevel below 6.0%,low-density lipoprotein cholesterol level below 70 mg/dL,high-density lipoprotein cholesterol level above 50 mg/dL[women]or above 40 mg/dL[men],triglyceride level below 150 mg/dL,systolic blood pressure below 120 mmHg).Enrollment occurred between July 2007 and May 2013,and follow-up extended to August 2014.The primary outcome was a composite of all-cause mortality,nonfatal MI,and UA requiring hospitalization;the secondary outcome was ischemic major adverse CV events(composite of CAD death,nonfatal MI,and UA).The results of the study showed at a mean follow-up of 4.0 years,the primary outcome event rates were not signif cantly different between the CCTA group and the control group(6.2 vs.7.6%).The incidence of the composite secondary end point of ischemic major adverse CV events also did not differ between the groups(4.4 vs.3.8%).Among asymptomatic patients with type 1 or type 2 DM,use of CCT A to screen them for SIHD did not reduce the composite rate of all-cause mortality,nonfatal MI,and UA requiring hospitalization at 4 years.These f ndings do not support CCT A screening in this population[11].In summary,despite the data from the Detection of Ischemia in Asymptomatic Diabetics and FACTOR-64 studies,the current version of the appropriate use criteria for SIHD rates some tests as“ may be appropriate ”for patients with high CV risk[12].
The Diabetic Patient with Ischemia Symptoms and Evidence of CAD
When ischemia symptoms are present,and there is suff cient suspicion of heart disease to warrant cardiac evaluation,current recommendations are to make a probability estimate of the likelihood of obstructive CAD before selection of testing[12].There are a number of validated risk assessment models that can be used to calculate this probability[13,14].Testing recommendations are typically made on the basis of the following classif cation system[12]:
· Low pretest probability:less than 10% pretest probability of obstructive CAD
· Intermediate pretest probability:between 10 and 90% pretest probability of obstructive CAD
· High pretest probability:more than 90% pretest probability of obstructive CAD
Although not incorporated into the algorithm,other risk factors may also af fect the pretest likelihood of obstructive CAD.Detailed nomograms are available that incorporate the effects of a history of prior MI,ECG Q waves,and ST-segment and T-wave changes,DM,and other cardiac risk factors[15].As a result,most patients with symptoms of ischemia and DM are likely to have at least intermediate or high pretest probability of obstructive CAD.In the current version of the appropriate use criteria,most testing options are considered appropriate for patients with ischemia symptoms and intermediate or high pretest probability.
The Diabetic Patient with no Ischemia Symptoms and with Evidence of Silent Ischemia
Data are sparse regarding outcomes after noninvasive testing for the management of asymptomatic patients with DM and SIHD.Silent ischemia is a prominent clinical concern in this patient population.Asymptomatic myocardial ischemia determined by ST changes on ambulatory electrocardiographic monitoring has been shown to occur more often than symptomatic ischemia in patients with SIHD[16].The Asymptomatic Cardiac Ischemia Pilot Study revealed with ambulatory electrocardiographic monitoring that nearly half of patients with SIHD have transient ST-segment depressions that likely represent silent ischemic events[17].In one study by the Milan Study on Atherosclerosis and DM group,12% of non-insulin-dependent diabetic patients with no symptoms suggestive of CAD had abnormal exercise ECGs and resting ECGs[18].In another study,33% of diabetic patients with at least one additional CV risk factor had silent ischemia[19].In patients with mild-to-moderate CAD,silent ischemia provides similar prognostic infor-mation for adverse outcomes as does symptomatic ischemia[20].In patients with SIHD,the likelihood of death or MI during 7 years of follow-up was similar between patients with asymptomatic ST-segment depression with exercise and patients with symptomatic ST-segment depression with exercise[20].However,among patients with medically treated extensive SIHD,silent ischemia is associated with worse prognosis than symptomatic ischemia[21].
The presence of signif cant silent ischemia in the current era of optimal medical therapy might still identify a subset of patients with increased risk of CV events[20].As a result,SIHD testing is rated as“ may be appropriate ”for patients with prior revascularization,even without symptoms[12].While this recommendation does not strictly address the patient’s DM status,the concern for silent ischemia may make testing a reasonable option.
Ischemia Symptoms in Patients with SIHD and with or without DM
Testing is a reasonable choice for SIHD patients with symptoms of ischemia regardless of their DM status.The choice to test,however,should be made in the context of the individual patient.If the patient recently had complete revascularization and has persistent angina,testing would not likely be useful,and medical management of symptoms would be preferred.Even in patients without recent revascularization,contemporary randomized controlled trial data suggest that revascularization does not reduce myocardial infarction or mortality in patients with SIHD.
Outcomes in Patients with DM and SIHD from the Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation Trial
While abundant data from previous studies show that aggressive medical management in SIHD effectively reduces CV events,the benef t of percutaneous coronary intervention(PCI)is less clear.The Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation(COURAGE)trial was undertaken to determine whether PCI plus optimal medical therapy(consisting of lifestyle modif cation and antiplatelet,antianginal,blood pressure-and glucose-lowering,and lipid-modifying therapies)would decrease CV events compared with optimal medical therapy alone[22,23].The trial randomly assigned 2287 patients with obstructive SIHD evidence of ischemia on noninvasive testing(or 80% or more stenosis plus Canadian Cardiovascular Society class III angina without ischemia testing to a strategy of either optimal medical therapy alone or combined with coronary revascularization).Patients with DM experienced high event rates compared with those without DM.However,there was no difference between the two treatment strategies within each subgroup.In the patients with DM(n=766),the event rate was 25% in the PCI group compared with 24% in the medical therapy group.In the patients without DM(n=1468),the event rate was 17% in the PCI group compared with 15% in the medical therapy group[23].In summary,PCI does not reduce CVD events for SIHD in patients with and without DM.DM patients did,however,have more extensive CAD and are more suitable for coronary artery bypass grafting.
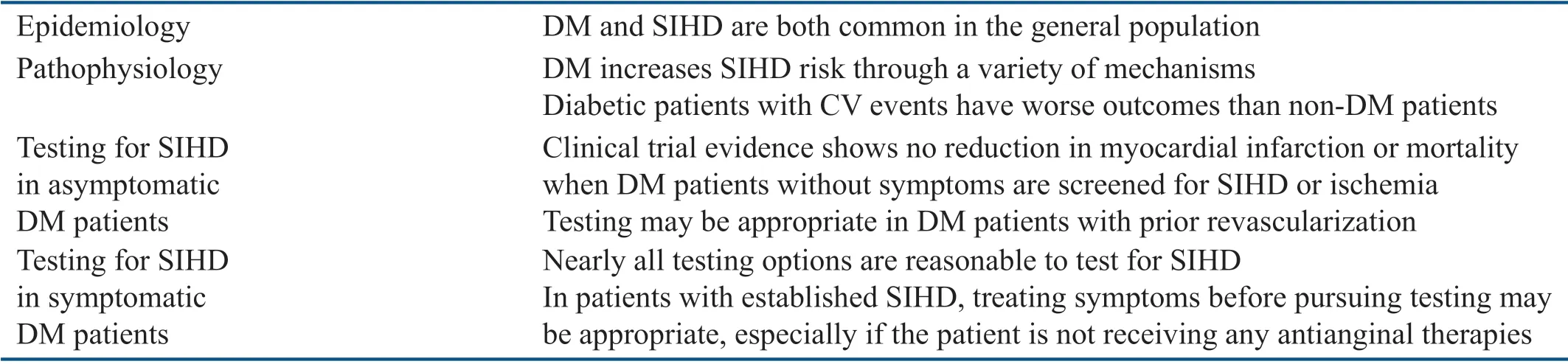
Table 1 Summary of Relevant Clinical Points.
Outcomes in Patients with DM and SIHD from the Bypass Angioplasty Revascularization Investigation in Type 2 DM Trial
Even more direct data on the question of revascularization for SIHD in DM patients comes from the Bypass Angioplasty Revascularization Investigation in Type 2 DM(BARI 2DM)trial.As with the COURAGE trial,revascularization did not reduce events over 5.3 years of follow-up[24].Neither of these studies directly addressed the question of whether noninvasive testing should be performed for SIHD patients with ischemic symptoms.Often the goal of such testing,however,is to select patients for revascularization that appears to have no benef-cial effect on outcomes such as death and MI.
Take-Home Message
Our take-home messages are summarized in Table 1.DM is a common disease that drives the development of SIHD through a variety of mechanisms.The presence of DM also increases the likelihood of poor outcomes after a CV event occurs.As the prevalence of DM continues to rise,so will the rates of CVD.The decision to test for ischemia may be a reasonable option in some DM patient groups;however,in many cases,revascularization for SIHD does not reduce mortality or the rate of MI.
Disclosure
David Winchester is supported by Career Development Award no.13-023 from the United States Department of Veterans Affairs Health Services Research and Development Program.
Confl ict of Interest
The authors declare that they have no conf icts of interest.
杂志排行

Cardiovascular Innovations and Applications的其它文章
- Contemporary Management of Patients with Stable Ischemic Heart Disease
- Left Ventricular Dysfunction in Ischemic Heart Disease
- Epidemiology,Pathophysiology,and Therapeutic Targets in Stable Ischemic Heart Disease
- Stable Ischemic Heart Disease in the Older Adult
- Sudden Cardiac Death in Adult Patients with Stable Ischemic Heart Disease
- Reading Electrocardiograms“Blind”