lntermediate-advanced hepatocellular carcinoma in Argentina:Treatment and survival analysis
2019-07-27FedericoPieroSebastiMarcianoNoraFernndezJorgeSilvaMargaritaAndersAlinaZeregaEzequielRidruejoGustavoRomeroBeatrizAmeigeirasClaudiaAmicoLuisGaiteCarlaBermdezVirginiaReggiardoLuisColombatoAdriGadanoMarceloSilva
Federico Piñero, Sebastián Marciano, Nora Fernández, Jorge Silva, Margarita Anders, Alina Zerega,Ezequiel Ridruejo, Gustavo Romero, Beatriz Ameigeiras, Claudia D'Amico, Luis Gaite, Carla Bermúdez,Virginia Reggiardo, Luis Colombato, Adrián Gadano, Marcelo Silva
Abstract BACKGROUND Hepatocellular carcinoma (HCC) represents the sixteenth most frequent cancer in Argentina. The rise of new therapeutic modalities in intermediate-advanced HCC opens up a new paradigm for the treatment of HCC.AIM To describe real-life treatments performed in patients with intermediateadvanced HCC before the approval of new systemic options.METHODS This longitudinal observational cohort study was conducted between 2009 and 2016 in 14 different regional hospitals from Argentina. Included subjects had intermediate-advanced Barcelona Clinic Liver Cancer (BCLC) HCC stages (BCLC B to D). Primary end point analyzed was survival, which was assessed for each BCLC stage from the date of treatment until last patient follow-up or death.Kaplan Meier survival curves and Cox regression analysis were performed, with hazard ratios (HR) calculations and 95% confidence intervals (95%CI).RESULTS From 327 HCC patients, 41% were BCLC stage B, 20% stage C and 39% stage D.Corresponding median survival were 15 mo (IQR 5-26 mo), 5 mo (IQR 2-13 mo)and 3 mo (IQR 1-13 mo) (P < 0.0001), respectively. Among BCLC-B patients (n =135), 57% received TACE with a median number of 2 sessions (IQR 1-3 sessions).Survival was significantly better in BCLC-B patients treated with TACE HR =0.29 (CI: 0.21-0.40) than those without TACE. After tumor reassessment by RECIST 1.1 criteria following the first TACE, patients with complete response achieved longer survival [HR = 0.15 (CI: 0.04-0.56, P = 0.005)]. Eighty-two patients were treated with sorafenib, mostly BCLC-B and C (87.8%). However,12.2% were BCLC-D. Median survival with sorafenib was 4.5 mo (IQR 2.3-11.7 mo); which was lower among BCLC-D patients 3.2 mo (IQR 2.0-14.1 mo). A total of 36 BCLC-B patients presented tumor progression after TACE. In these patients,treatment with sorafenib presented better survival when compared to those patients who received sorafenib without prior TACE [HR = 0.26 (CI: 0.09-0.71); P= 0.013].CONCLUSION In this real setting, our results were lower than expected. This highlights unmet needs in Argentina, prior to the introduction of new treatments for HCC.
Key words: Hepatocellular carcinoma; Therapeutics; Survival; Real-life
INTRODUCTION
According to the latest estimates made by the International Agency for Research on Cancer [IARC (http://gco.iarc.fr)] for the year 2018, Argentina has an incidence rate of 212 cases per 100000 inhabitants[1]. This figure places it within the countries of the world with medium-high incidence of cancer (range 177 to 245.6 per 100000 inhabitants) and in seventh place in Latin America. Although liver cancer or hepatocellular carcinoma (HCC) is currently the 5thmost common cancer and the 2ndcause of death from cancer worldwide, in Argentina represents the sixteenth most frequent cancer (www.argentina.gob.ar/salud/instituto-nacional-del-cancer)[1].
Given that in more than 90% of the cases this tumor develops in patients with cirrhosis or chronic infection with hepatitis B or C virus, the diagnostic, staging and therapeutic management in our country is mainly done by hepatologists or hepatobiliary surgeons, rather than clinical oncologists[2].
Transarterial chemoembolization (TACE) and systemic treatment with sorafenib or lenvatinib are the standard treatments for patients with intermediate and advanced stage HCC[3-5]. The rise of new therapeutic modalities such as radioembolization, the combination of antiangiogenic agents with locoregional therapies and other first and second line systemic options, open up a new paradigm for the treatment of HCC.
In this dual cohort study, we aimed to describe treatments performed in the real life setting before the approval of these new systemic options. It is of interest to know the real life context, in order to evaluate the therapeutic management in these patients and gaps that should be explored more thoroughly as areas of public health improvement.
MATERIALS AND METHODS
Study design, setting and participating centers
This longitudinal observational cohort study was conducted in 14 different regional hospitals from Argentina. Two cohorts of consecutive adult patients (> 17 years of age) with newly diagnosed HCC were included. Between January 1 2009 and September 1 2014, a retrospective cohort was followed-up until death or last ambulatory visit until January 1 2016 (Cohort 1). A second prospective cohort was included from September 2 2014, followed until January 1 2016 (Cohort 2). Participating centers appointed a study coordinator responsible for data collection. Sites were instructed to enroll all eligible patients on a sequential basis and to record data from medical charts into a web-based electronic system. In cases of conflicting or missing data, central revision and resubmission was requested.
Cohort characteristics and study variables
Patients with intermediate (BCLC-B) or advanced-end stage (BCLC C-D) HCC were included[6,7]. Criteria for inclusion required patients to be adult recipients with newly diagnosed HCC either by pathological criteria or imaging evaluation as recommended by international Western guidelines[6,7]. Intermediate stage or BCLC B includes patients with preserved liver function with multifocal tumors, in the absence of cancer related symptoms, vascular invasion or extrahepatic spread. In these patients the recommended treatment is TACE. Advanced-stage HCC (BCLC C) comprises patients with preserved liver function, good performance status or ECOG 1-2, with extrahepatic spread (lymph node involvement or metastases) or vascular invasion. In this subgroup, sorafenib or lenvatinib are the recommended treatments. As lenvatinib has been recently approved in our country (March 2019), this cohort includes patients treated under sorafenib. Best supportive care (BSC) or symptomatic treatment is recommended for patients with unpreserved liver function (Child Pugh C) or ECOG> 2 or cancer related symptoms[8]. Patients were excluded if (1) clinical baseline data was missing; (2) BCLC stage was either 0 or A; and (3) patients with BCLC-B-D who underwent liver transplantation.
Baseline characteristics at HCC diagnosis included patients demographics,performance status (ECOG grade 0-4), grade of liver fibrosis (I-IV) assessed by liver biopsy or elastography or other non-invasive measurements or by clinical data(including imaging data, presence of gastro-esophageal varices or ascites or splenomegaly > 120 mm diameter, or other complications related to portal hypertension),Child Pugh score; selected laboratory variables, serum alpha-fetoprotein (AFP) levels and tumor characteristics at diagnosis, as well as treatments performed. Computed tomography (CT) or magnetic resonance images (MRI) were evaluated considering tumor number and diameter, vascular invasion and extrahepatic or lymph node metastasis.
Tumor treatment after HCC diagnosis was reviewed, namely: Liver resection (LR),radiofrequency ablation (RFA), percutaneous ethanol injection (PEI), trans-arterial chemoembolization (TACE), trans-arterial radioembolization (TARE), sorafenib and best supportive care (BSC). Each treatment was discussed at each center on a case-bycase basis. Imaging tumor reassessment after treatments were done according to RECIST 1.1 criteria as recommended by international Western guidelines[6,7].
Study end-points
Primary end point analyzed was survival, which was assessed for each BCLC stage from the date of treatment until last patient follow-up or death. Secondary objectives were to (1) describe treatments performed in each BCLC stage; (2) to evaluate the sequential treatment of TACE-sorafenib in BCLC-B patients; and (3) to evaluate adverse events and tolerability of sorafenib in the daily practice.
All procedures followed were in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement[9]. This study was approved by the Austral University School of Medicine and by each center; complied with the ethical standards (institutional and national) and with Helsinki Declaration of 1975, as revised in 2008.
Statistical analysis
Statistical significance is e xpressed as P < 0.05. Categorical data were compared using Fisher's exact test or Chi-Square test. Continuous variables were compared with Student's T test or Mann-Whitney U test according to their distribution, respectively.Multiple comparisons for continuous data were done according to its distribution with ANOVA or Kruskal Wallis tests as appropriate. Dummies for ordinal variables were assessed. For survival analysis, Cox regression analysis estimating hazard ratios(HR) and 95%CI for baseline variables related with mortality was performed.Proportional hazards through graphic and statistical evaluation (Schoenfeld residual test) were done. Kaplan Meier survival curves were compared using the log-rank test(Mantel-Cox) Collected data was analyzed using STATA 13.0.
RESULTS
From a total of 721 consecutive adult patients with HCC during the study period, 327 patients with newly diagnosed intermediate and advanced HCC were included.Patients who received a liver transplant in BCLC-B (n = 16), BCLC-C (n = 2) and BCLC-D (n = 28) were excluded.
Table 1 describes the main baseline patient characteristics. Overall, 41.3% of the patients were in BCLC stage B (n = 135), 19.9% in stage C (n = 65) and 38.8% in stage D (n = 127). Treatments performed during the whole follow-up period were LR (n =36), RFA or PEI (n = 19), TACE (n = 126), TARE (n = 6), sorafenib (n = 82) and BSC (n =146).
Outcomes were assessed in all patients during follow-up with a median survival of 12.0 mo (IQR 4.0-27.0 mo). Corresponding median survival for BCLC stages were as follows: stage B 15 mo (IQR 5-26 mo), stage C 5 mo (IQR 2-13 mo) and stage D 3 mo(IQR 1-13 mo)(Figure 1).
Characteristics and management of patients treated with TACE
TACE was performed in 126 patients (38.5%); 77 were BCLC-B, 22 were BCLC-C and 27 patients were BCLC-D. According to the type of endovascular treatment, 43.6% of the patients were treated with conventional TACE (cTACE), 45.2% with TACE with drug eluting beads (TACE-DCbeads) and 11.2% with transarterial embolization(TAE).
Among BCLC-B patients (n = 135), 57% received TACE (n = 77) whereas 43% did not (Table 2). Median number of TACEs sessions was 2 (IQR 1-3 sessions); 40%, 26%and 34% of these patients received 1, 2 and 3 or more sessions, respectively. Other treatments than TACE were performed in BCLC-B patients, as follows: RFA or PEI in 7 patients, liver resection in 21 patients, sorafenib in 15 patients and BSC in 5 patients.
Of the 22 BCLC-C patients who were treated with TACE, 13 had non-main portal trunk vascular invasion and 12 patients had extrahepatic disease (lymph node metastasis in 5, bone metastasis in 3 and 4 patients with lung involvement). Sorafenib was the following treatment performed in 7 patients. Among BCLC-D, 27 patients received TACE, 19 were Child Pugh C, 10 patients presented performance status ECOG 3-4, 2 patients presented non-main portal trunk vascular invasion and 1 had extrahepatic disease (lymph node metastasis). Best supportive care following TACE was done in all patients except for 1 who received sorafenib in this latter group.
Survival was significantly better in BCLC-B patients treated with TACE HR 0.29(CI: 0.21-0.40) with a median survival of 15 mo (IQR 7-25 mo), when compared with BCLC-B without TACE and BCLC-C or D patients treated with TACE (Figure 2A).According to tumor reassessment after the first TACE, patients with complete response (CR) achieved a better overall survival with a HR of 0.15 (CI: 0.04-0.56. P =0.005) (Figure 2B).
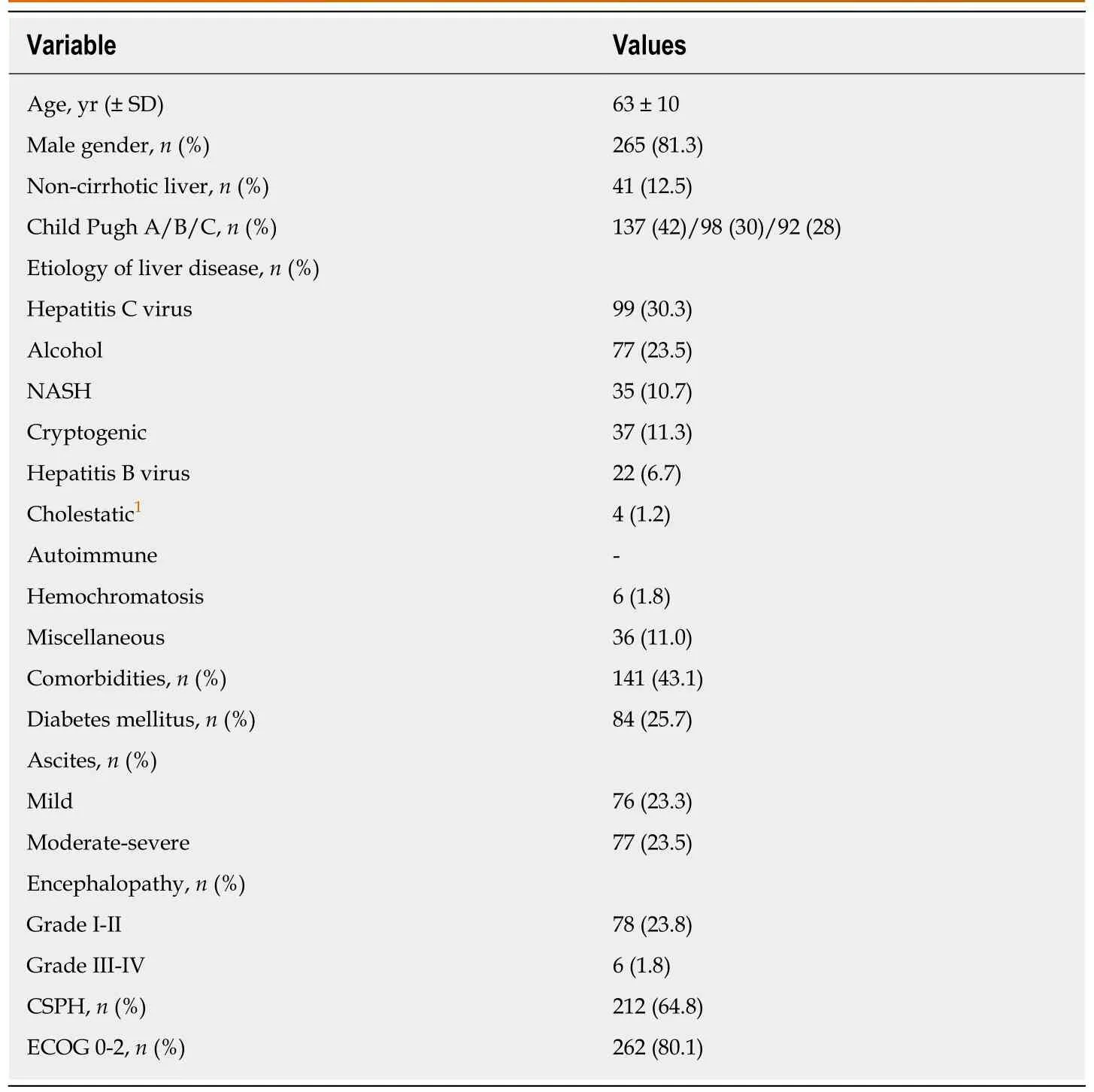
Table 1 Patients' baseline characteristics
Characteristics and management of patients treated with sorafenib
Table 3 describes baseline patient characteristic treated with sorafenib (n = 82). Of these, 43.9% were BCLC-B, 43.9% BCLC-C and 12.2% BCLC-D. Among BCLC-B, 15 were TACE naïve and 21 received a median number of 3 TACE sessions (IQR 2-4 sessions) until disease progression (n = 7) or no response (n = 14). Among BCLC-C patients (n = 65), 55.4% were treated with sorafenib, 21 received BSC and 8 patients received other treatments (4 patients TACE, 1 TARE and patients 3 LR).
Median sorafenib treatment duration was 4.0 mo (IQR 2-11 mo). The most frequent sorafenib starting dose was 400 mg/d in 41% of the patients, followed by 800 mg/d in 32%. During follow-up, 55% of the patients achieved 800 mg full-dose of treatment,35.4% had dose reductions (n = 29) of which in 21 patients dose-reduction were associated with drug-related adverse events. Most frequent adverse events (AEs) were fatigue (n = 27), diarrhea (n = 16), dermatologic events (n = 5), hand-foot-skin reaction(n = 3), and hypertension (n = 1). Permanent treatment discontinuation was observed in 12.2% of the patients secondary to treatment AEs (n = 10), tumor progression in 26.8%, (n = 22) and death in the rest of the patients. In 37 out of 82 patients in which radiologic evaluation after sorafenib initiation was performed, complete and partial responses were observed in 1.2% (n = 1) and 2.4% (n = 2), respectively. In these subgroup, median time to progression since sorafenib initiation was 7.3 mo (IQR 2.1-10.7 mo).
Corresponding median survival in all patients treated with sorafenib was 4.5 mo(IQR 2.3-11.7 mo); 5.2 mo (IQR 3.7-12.6 mo) in BCLC-B, 3.8 mo (IQR 1.9-9.9 mo) in BCLC-C and 3.2 mo (IQR 2.0-14.1 mo) in BCLC-D (Figure 3). When comparing BCLCB and C vs BCLC-D treated patients, although it did not reach statistical significance, a better survival curve was observed in BCLC-B/C patients with a HR of 0.63 (CI: 0.31-1.27; P = 0.19).
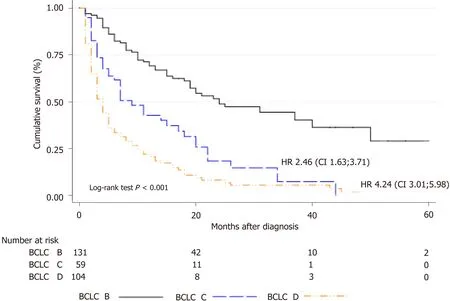
Figure 1 Cumulative survival stratified by Barcelona Clinic Liver Cancer staging in the overall cohort. BCLC: Barcelona clinic liver cancer.
Sequential treatment with Sorafenib after TACE and impact on survival
Imaging evaluation after the first TACE in BCLC-B patients was registered in 64 out of 77 patients in median time from TACE to evaluation of 5 wk (IQR 4-6 wk).According to RECIST 1.1 criteria tumor response was as follows: partial response in 62.5% (n = 40), stable disease 15.6% (n = 10), complete response in 12.5% (n = 8), and disease progression in 9.3% (n = 6). Thus, overall objective response (ORR) and disease control rates (DCR) were 75% and 90.7% after first TACE, respectively.
In BCLC-B patients treated with sorafenib after progression (n = 36), the sequential treatment of sorafenib following TACE presented better survival when compared to those patients who received sorafenib without prior treatment with TACE [HR = 0.26(CI: 0.09-0.71); P = 0.013] (Figure 4). Median number of TACEs in these patients prior to systemic treatment was 3 sessions (IQR 2-4 sessions). Among those patients not treated with TACE prior to sorafenib initiation, prior treatments were RFA/PEI (n =4) and LR (n = 5).
DISCUSSION
This is the first observational study of treatments performed in the real life setting from Argentina in patients with intermediate to advanced stage HCC and one of the only ones to report post-treatment survival in Latin America. Knowing the real life treatment patterns is of interest to highlight unmet needs in the daily practice prior to the introduction of new treatments for HCC.
In this cohort we observed that in the majority of patients in intermediate stage, the most frequent treatment in daily practice was TACE. The effect on survival was beneficial in these patients in particular when treatment was established in accordance with Western clinical practice recommendations[6,7]. In patients with unpreserved liver function or BCLC-C, TACE was performed in a smaller proportion with heterogeneous effect on survival. On the other hand, those patients in BCLC-B stage with complete tumor response after TACE showed a better survival. Likewise, a non-negligible proportion of BCLC-B patients started sorafenib in the absence of prior TACE as a decision of “treatment stage migration”[10]. In the era of sequential treatment recommendation, in those BCLC-B patients with tumor progression after TACE[11], a better survival with sorafenib was observed with respect to those patients without prior TACE.
Knowing the therapeutic decisions in the daily practice is important because it reflects the gaps between interventional studies evaluating efficacy in ideal situations and those in the real-life setting. The BRIDGE study is an example, among others, of how therapeutic decisions in patients with HCC are complex, demanding a fine knowledge not only of tumor extension, but also of liver disease and its complications[12]. That is why the role of hepatologists is of utmost importance in the treatment of these patients. In our cohort, most of the patients were screened, diagnosed and treated by hepatologists, both in referral or local centers.
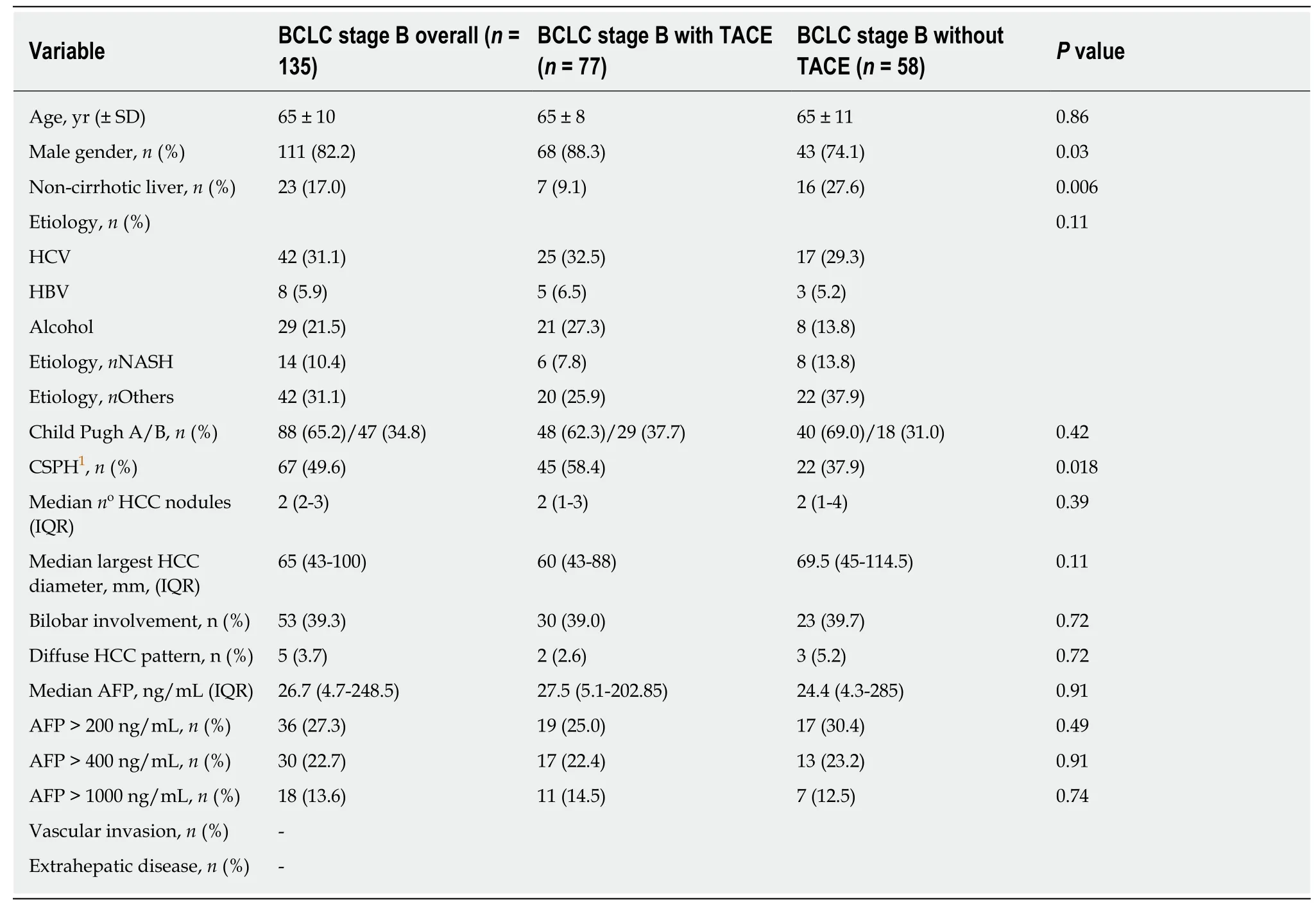
Table 2 Stratified analysis comparing transarterial chemoembolization treatment in barcelona clinic liver cancer stage B
Treatment with TACE has been established as the gold standard for intermediate stage HCC since more than 10 years ago[3,4]. Two randomized, placebo-controlled trials have shown its survival benefit[3,4]; results further underlined in a metaanalysis[13]. However, clinical and tumor heterogeneity, which are characteristic of BCLC-B patients, results in a diversity of established treatments[12]. In our analysis, we excluded BCLC-B patients who underwent transplantation, given that we considered performing a pure analysis in this stage. The same went for BCLC-D patients. In the original trials of TACE, a median survival was close to eighteen months[3,4,14]whereas in more recent observational studies, median survival of forty months has been reported[15]. In our study, median survival in BCLC-B patients treated with TACE was fifteen months. Survival was significantly better in BCLC-B patients treated with TACE with a 71% relative risk reduction of death when compared with BCLC-B without TACE and BCLC-C or D patients treated with TACE. According to tumor reassessment by RECIST 1.1 criteria after the first TACE, patients with complete response had the highest survival benefit, as previously reported elsewhere[16].
Systemic treatment of HCC is remarkably changing given the introduction of alternative therapies in first line such as lenvatinib[17]and second-line including regorafenib[18], cabozantinib[19]and ramucirumab[20]. In our country, as in many others from Latin America, approval of these new treatments usually takes between 12 and 24 mo later than other developed regions of the world. In 2009 and 2017, sorafenib and regorafenib were approved in our country, respectively. Recently, the use of lenvatinib has also been approved, not yet included in the daily practice. Treatment with immunotherapy, either with nivolumab[21]or pembrolizumab[22], has not been approved by the National Regulatory Agency in our country (ANMAT).
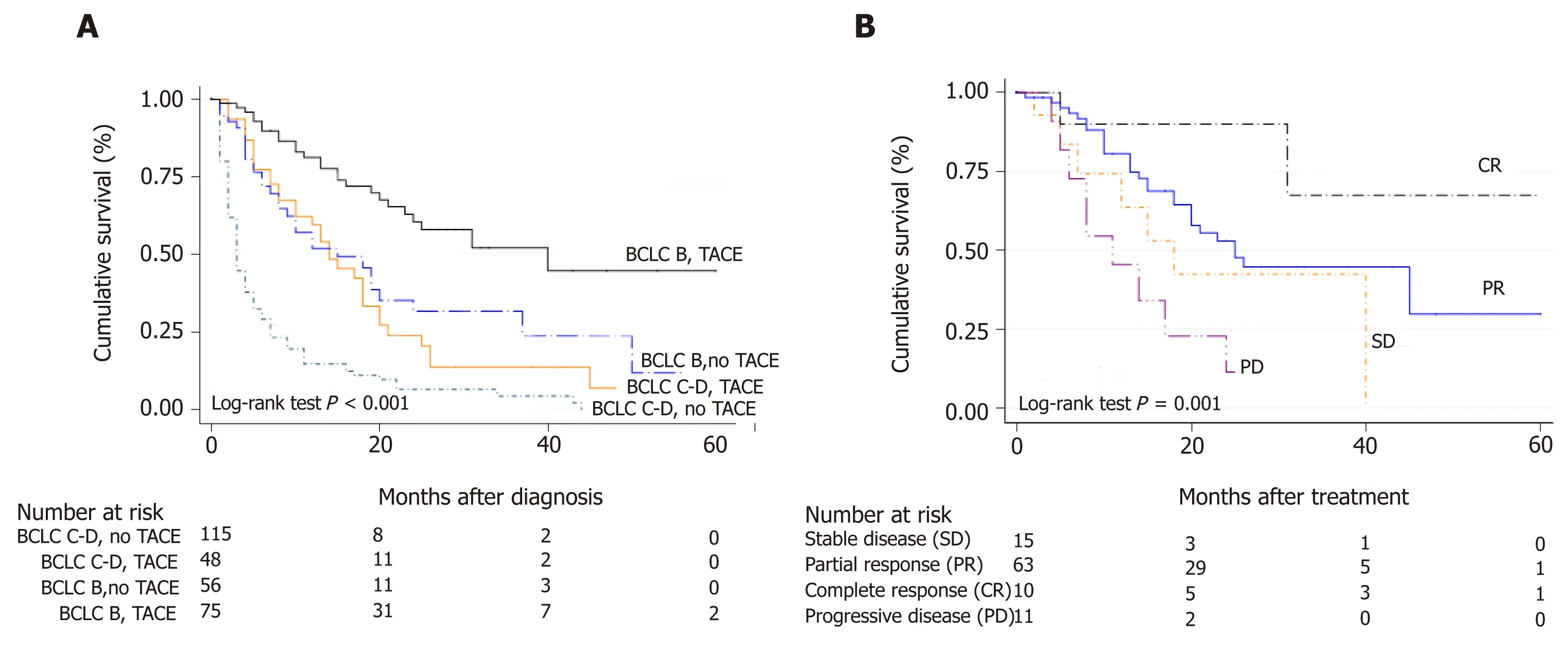
Figure 2 Characteristics and management of patients treated with transarterial chemoembolization. A: Kaplan Meier survival curves according to Barcelona Clinic Liver Cancer stage and treatment with/without trans-arterial chemoembolization; B: Survival according to radiological response after the first transarterial chemoembolization (TACE) evaluated by RECIST 1.1 criteria. BCLC: Barcelona clinic liver cancer.
Argentina is a South American country with a wide extension, a great sociocultural heterogeneity with a large variety in health care systems. In many cases, the main barrier for the access to health system is the authorization by insurances to carry out diagnostic studies or therapies due to costs or other barriers. This problem is common in Latin America[23]. In this study, the use of sorafenib slightly exceeded half of BCLC-C patients, presenting better survival when compared with those patients in the same stage but without systemic treatment. We observed that in our cohort,median survival with the use of sorafenib was strikingly low, being no more than 5 months. This lower than expected outcome can be explained, in part, by the delay in starting treatment, due to a wide range of authorizations and complex administrative processes. This might have leaded to a significant slowness in the initiation of systemic treatment. Moreover, most of the patients were initially treated with half dose rather than full dose.
It is noteworthy of mention that sorafenib tolerance was similar to that reported from first (SHARP and Asia-Pacific)[5,24]and second line (RESORCE)[18]clinical trials,with a rate of definitive treatment discontinuation due to related adverse events of 12.2%. On the other hand, in those patients in whom radiological response was evaluated, median time to progression under treatment with sorafenib was similar than that previously reported[18]. Finally, we observed that there was an inadequate use of sorafenib in patients with unpreserved liver function or BCLC-D that was associated with a poor prognosis, demonstrating an inadequate and inefficiency use of resources.
Our study has limitations. In particular, given that it was mainly a retrospective cohort study, exposed to different selection and information biases. Specifically,neither radiological evaluation assessing time to progression was homogeneous nor there was a centrally blinded evaluation through all participating centers. However,we enrolled a group of centers presenting similar decision making processes trying to homogenize the sample.
In conclusion, in this dual cohort study from Argentina, we described the treatments performed in the real life setting before the approval of new systemic options.Knowing this life context is of interest, in order to assess the most common therapeutic decision making processes and management in these patients. In this real setting, our results highlights unmet needs and improvement areas in public health among developing regions, particularly to promote early and correct treatments in each stage, prior to the introduction of new treatments for HCC.
ACKNOWLEDGEMENTS
On behalf of the Latin American Liver Research, Education and Awareness Network(LALREAN).
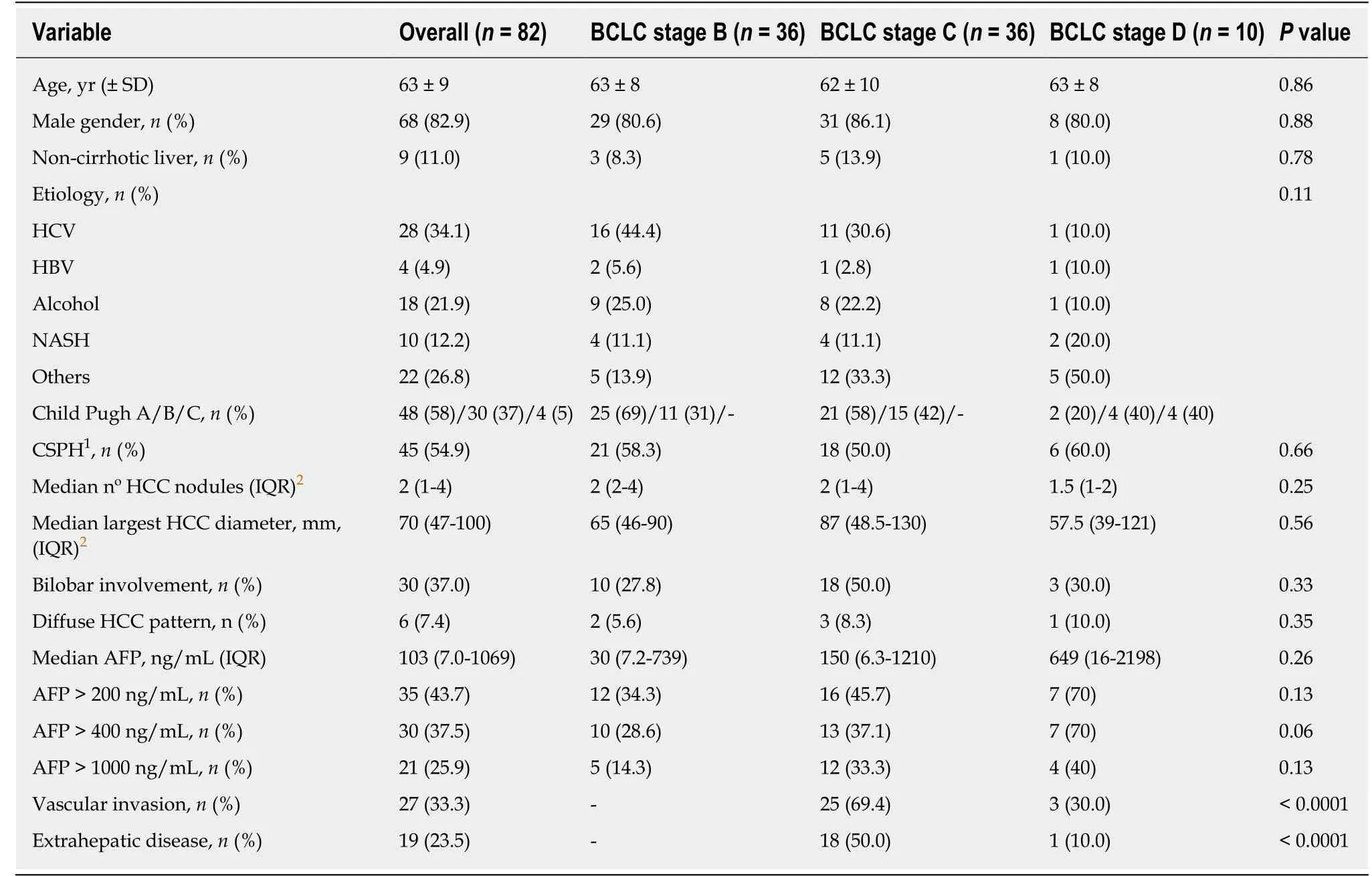
Table 3 Characteristic of patients treated with sorafenib
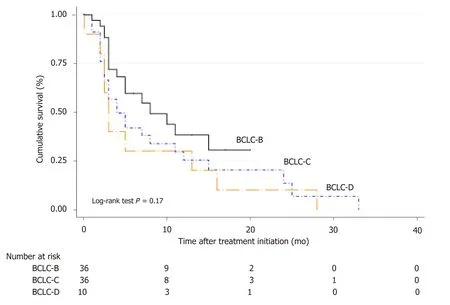
Figure 3 Corresponding survival curves for patients treated with Sorafenib stratified by Barcelona Clinic Liver Cancer stages. BCLC: Barcelona clinic liver cancer.
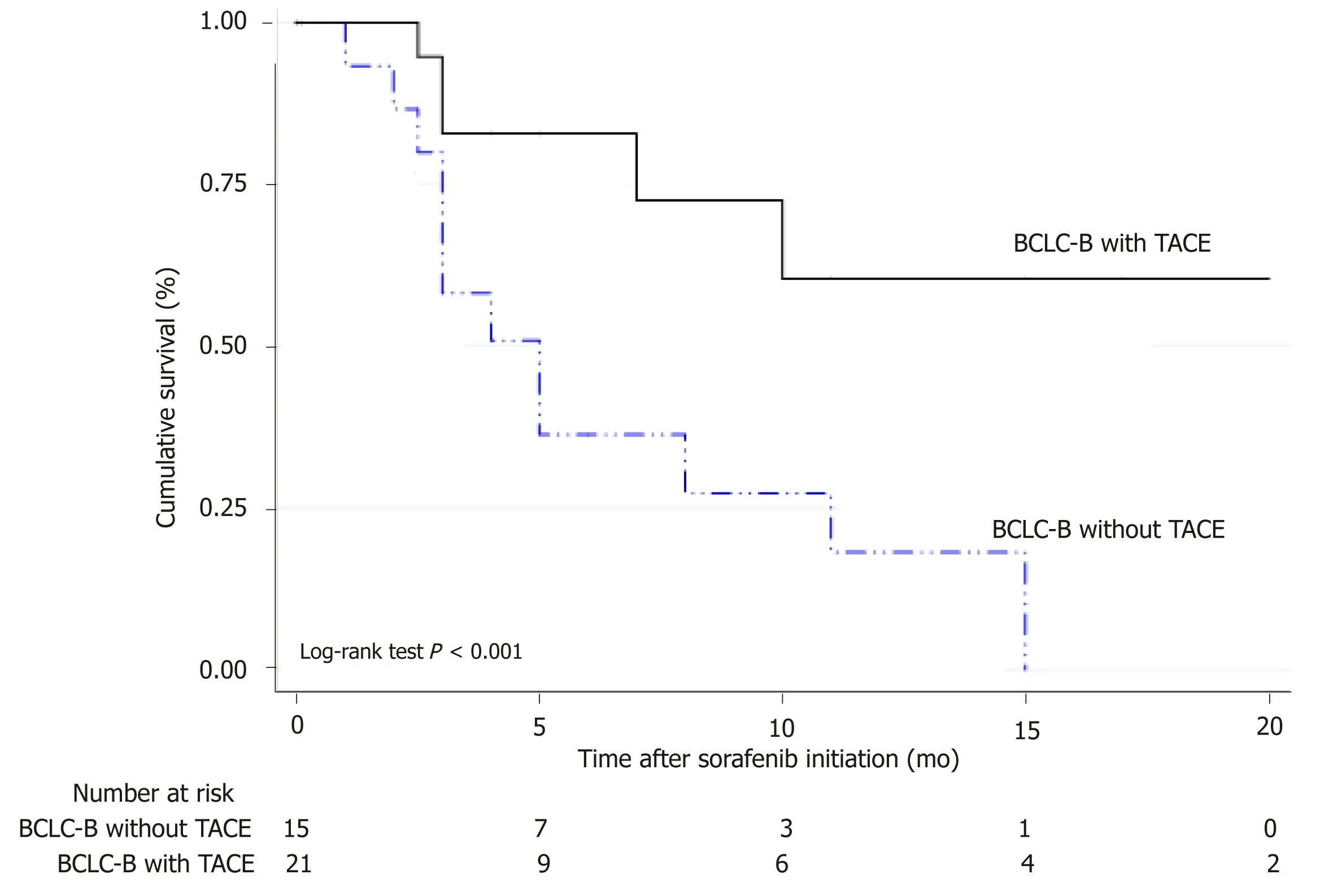
Figure 4 Survival in Barcelona Clinic Liver Cancer stage B patients under tumor progression with the sequential treatment of transarterial chemoembolization-sorafenib. BCLC: Barcelona clinic liver cancer.
ARTICLE HIGHLIGHTS
Research background
Although liver cancer or hepatocellular carcinoma (HCC) is currently the 5th most common cancer and the 2nd cause of death from cancer worldwide, in Argentina represents the sixteenth most frequent cancer. Transarterial chemoembolization (TACE) and systemic treatment with sorafenib are the standards of treatment for patients with intermediate and advanced stage HCC.
Research motivation
The rise of new therapeutic modalities such as radioembolization, the combination of antiangiogenic agents with locoregional therapies and other first and second line systemic options,open up a new paradigm for the treatment of HCC.
Research objectives
Our aim was to describe the treatments performed in the real life setting before the approval of these new systemic options.
Research methods
This longitudinal observational cohort study was conducted between in 14 different regional hospitals from Argentina between 2009 and 2016. Study data were registered into a web-based electronic system. Patients with intermediate (BCLC-B) or advanced (BCLC C-D) HCC were included. Patients were excluded if (1) clinical baseline data was missing; (2) BCLC stage was either 0 or A, in which potentially curative treatments are recommended such as liver resection(LR), percutaneous ethanol injection (PEI)/radiofrequency ablation (RFA) or liver transplantation(LT); and (3) patients with BCLC-B-D who underwent liver transplantation. Baseline tumor and patients characteristics at HCC diagnosis, as well as treatments performed were registered. Each treatment was discussed at each center on a case-by-case basis. Imaging tumor reassessment after treatments were done according to RECIST 1.1 criteria as recommended by international Western guidelines. Median survival was assessed for each BCLC stage from the date of treatment until last patient follow-up or death. For survival analysis, Cox regression analysis estimating hazard ratios (HR) and 95%CI for baseline variables related with mortality was performed. Kaplan Meier survival curves were compared using the log-rank test (Mantel-Cox).
Research results
A total of 327 consecutive adult patients with intermediate and advanced HCC were included, of which 41.3% of the patients were in BCLC stage B (n = 135), 19.9% in stage C (n = 65) and 38.8%in stage D (n = 127). Corresponding median survival for BCLC stages were as follows: Stage B 15 mo (IQR 5-26 mo), stage C 5 mo (IQR 2-13 mo) and stage D 3 mo (IQR 1-13 mo)(Figure 1). TACE was performed in 126 patients (38.5%); 77 were BCLC-B, 22 were BCLC-C and 27 patients were BCLC-C. Among BCLC-B patients (n = 135), 57% received TACE (n = 77) whereas 43% did not(Table 2). Median number of TACEs sessions was 2 (IQR 1-3 sessions). Survival was significantly better in BCLC-B patients treated with TACE HR 0.29 (CI: 0.21-0.40) with a median survival of 15 mo (IQR 7-25 mo), when compared with BCLC-B without TACE and BCLC-C or D patients treated with TACE. According to tumor reassessment after the first TACE by RECIST 1.1 criteria,patients with complete response (CR) achieved a better overall survival with a HR of 0.15 (CI:0.04-0.56, P = 0.005). Table 3 describes baseline patient characteristic treated with sorafenib (n =82). Of these, 43.9% were BCLC-B, 43.9% BCLC-C and 12.2% BCLC-D. Among BCLC-B patients who received sorafenib, 15 were TACE naïve and 21 received a median number of TACEs of 3(IQR 2-4) until disease progression (n = 7) or no response or un-TACE-able (n = 14). Among BCLC-C patients (n = 65), 55.4% were treated with sorafenib and those not treated with sorafenib received BSC (n = 21) and other treatments (4 patients TACE, 1 TARE and patients 3 LR).Corresponding median survival in all patients treated with sorafenib was 4.5 mo (IQR 2.3-11.7 mo); 5.2 mo (IQR 3.7-12.6 mo) in BCLC-B, 3.8 mo (IQR 1.9-9.9 mo) in BCLC-C and 3.2 mo (IQR 2.0-14.1 mo) in BCLC-D. In BCLC-B patients treated with sorafenib after progression (n = 36), the sequential treatment of sorafenib following TACE presented better survival since systemic treatment when compared to those patients who received sorafenib without prior treatment with TACE [HR = 0.26 (CI: 0.09-0.71); P = 0.013].
Research conclusions
In conclusion, in this dual cohort study from Argentina, we describe the treatments performed in the real life setting before the approval of new systemic options.
Research perspectives
Knowing the real life setting is of interest, in order to assess the most common therapeutic decision making processes and management in these patients. Our results highlights unmet needs and improvement areas in public health among developing regions such as Argentina,particularly to promote early and correct treatments in each stage, prior to the introduction of new treatments for HCC.
杂志排行

World Journal of Gastroenterology的其它文章
- lmmunotherapy with dendritic cells and cytokine-induced killer cells for hepatocellular carcinoma: A meta-analysis
- Bioartificial liver support systems for acute liver failure: A systematic review and meta-analysis of the clinical and preclinical literature
- Quantitative diffusion-weighted magnetic resonance enterography in ileal Crohn's disease: A systematic analysis of intra and interobserver reproducibility
- Lingguizhugan decoction attenuates diet-induced obesity and hepatosteatosis via gut microbiota
- Mucosal healing progression after acute colitis in mice
- ls the treatment outcome of hepatocellular carcinoma inferior in elderly patients?