Effect of different doses of intrathecal dexmedetomidine on hemodynamic parameters and block characteristics after ropivacaine spinal anesthesia in lower-limb orthopedic surgery:a randomized clinical trial
2019-07-11LalehFarokhmehrHesameddinModirBijanYazdiAlirezaKamaliAmirAlmasiHashiani
Laleh Farokhmehr,Hesameddin Modir ,Bijan YazdiAlireza KamaliAmir Almasi-Hashiani
1 Student Research Committee,Arak University of Medical Sciences,Arak,Iran
2 Departments of Anesthesiology and Critical Care,Arak University of Medical Sciences,Arak,Iran
3 Department of Epidemiology,School of Health,Arak University of Medical Sciences,Arak,Iran
4 Traditional and Complementary Medicine Research Center (TCMRC),Arak University of Medical Sciences,Arak,Iran
Abstract
Key words:dexmedetomidine; ropivacaine; hemodynamic changes; block characteristics; blood pressure; heart rate; oxygen saturation; sensory block; motor block; randomized clinical trial
INTRODUCTION
Any human body area intended for surgery needs to be anesthetized by spinal anesthesia (SA)1among which subarachnoid SA accomplished by local anesthetics covers some benefits such as fast onset of action,patient comfort,less adjuvant required,and good sensory-motor block.1,2Postoperative pain can be improved by stimulation of α-2 adrenergic receptor agonists in the spinal cord,which include dexmedetomidine.3-6Dexmedetomidine produces a prolonged duration of postoperative analgesia and a longer duration of sensory-motor block with minimal complications.7Some studies have been done on the effect of the addition of dexmedetomidine to ropivacaine,showing that dexmedetomidine can prolong the duration of sensory-motor block and hasten the onset.7-10The onset of action is shorter in ropivacaine than that of bupivacaine and this,hence,is highly important in consequence of anesthesia.1
Moreover,a study by Zhang et al.11with different doses of dexmedetomidine as an adjuvant to bupivacain reported that intrathecal dexmedetomidine prolongs the duration of SA,though increasing the risk of bradycardia in the subject.According to the study of Sharma et al.10on the effect of the addition of dexmedetomidine to 0.2% ropivacaine for femoral nerve block,dexmedetomidine,if added,prolonged the duration of postoperative analgesia and that of the block in their subjects.As reported by Singh et al.12in another trial comparing the effects of different doses of intrathecal dexmedetomidine as an adjuvant to ropivacaine in abdominal surgeries,dexmedetomidine 10 μg/kg would prolong the duration of analgesia without any adverse side effects.Various studies have focused on the doses (between 2-15 μg/kg) in SA and on adding dexmedetomidine to bupivacain,but not using ropivacaine.13-15
Merely one study has so far been published on adding different doses of dexmedetomidine to ropivacaine in the SA.12In comparison to Singh et al.'s study,12the present study was completed based on the different doses of ropivacaine used,as well as the difference in the type of surgery.In this study we intended to see if a lower dose might provide sufficient and acceptable duration of block and analgesia,as well as less complications.Therefore,we decided to perform a study aiming at comparing different doses of dexmedetomidine on hemodynamic parameters and block characteristics after SA using ropivacaine in lower-limb orthopedic surgery.
SUBJECTS AND METHODS
Design
We followed the CONsolidated Standards of Reporting Trials (CONSORT) Statement in conducting and reporting this randomized trial.16This study was a blinded,randomized,placebo-controlled,parallel-group clinical trial.Intentionto-treat approach was used to analyze the data.This study as a residency thesis was registered and approved by the Iranian Registry of Clinical Trials in 2017 (IRCT No.IRCT2017070614056N12).All participants in three groups and also research team were blinded regarding grouping information.It should be noted that the data were measured and recorded by a resident anesthesiologist,without any awareness of the patient group,when an anesthesiologist prepared adjuvants in each group and a resident anesthesiologist,having performed the SA,was unaware of the nature of adjuvants in each syringe.
Subjects
Ninety patients undergoing SA in lower-limb orthopedic surgery,were included in study after obtaining written informed consent and verification of inclusion and exclusion criteria.Inclusion criteria were age 18-60 years,American Society of Anesthesiologist status I/II,patients selected from both genders,and patients undergoing lower-limb orthopedic surgery,patient satisfaction of SA,body mass index<30 kg/m2,no previous use of β-blockers,α-2 agonists and calcium channel blockers,no cardiovascular problems,lack of pregnancy,no coagulation disorders,no local infection in the spinal area,no history of allergy to dexmedetomidine and ropivacaine,no arrhythmia,no psychological problems,and lack of peripheral and central neuropathy.Exclusion criteria included failure in SA and patient dissatisfaction.All subjects were hospitalized at least a day before surgery and were kept nil per os for 8 hours.Once demographic data were recorded,two IV lines were placed in different areas,first to administrate the adjuvants studied,and second to use for serum and other drugs.This study was approved by Ethical Committee of Arak University of Medical Sciences in 2017 (Ethical Code:IR.ARAKMU.REC.1396.37).The fl owchart of patient's recruitment was shown in Figure 1.
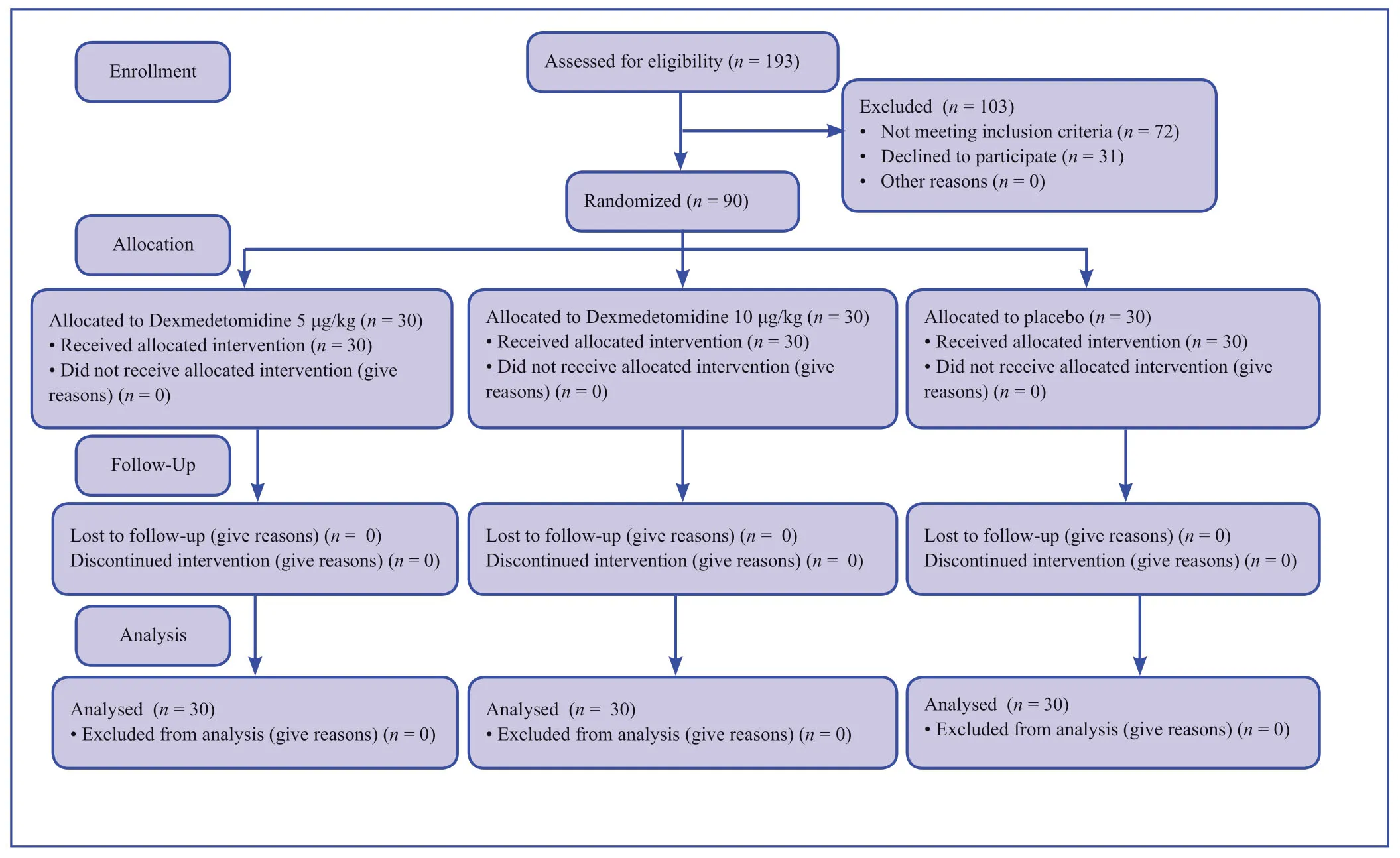
Figure 1:The fl owchart of patient's recruitment.
Intervention
Before the procedure we measured and recorded baseline heart rate (HR) and mean arterial pressure (MAP) (assessed by noninvasive blood pressure monitoring,as well as arterial oxygen saturation,then all participants were received 10 mL/kg of crystalloid (Ringer's solution) in the supine position on arrival to the operating room,and finally divided into three groups using block randomization:SA was performed with a 25-26-gauge Quincke needle at the L3/L4 or L4/L5 intervertebral space,for which we used 3 mL (15 mg) 5.0% ropivacaine (Ropivacaina Molteni®,Molteni Farmaceutici,Italy) for all subjects,1i.e.,the first group (dexmedetomidine 5 μg/kg group) received 3 mL (15 mg) of ropivacaine with 5 mg of dexmedetomidine (2 mL) intrathecally,while the second (dexmedetomidine 10 μg/kg group),3 mL (15 mg) of ropivacaine with 10 μg/kg dexmedetomidine (2 mL),and the third (Placebo group),3 mL (15 mg) of ropivacaine with 2 mL distilled water.The dexmedetomidine used was manufactured by Hospira,King of Prussia,PA,USA,and distilled water vials by Darou Pakhsh Co.,Tehran,Iran.
Outcomes
After AS,patients were placed in a supine position,and MAP,HR,and oxygen saturation (SaO2) were recorded in the three groups at the first 15 minutes and then every 15 to 180 minutes at recovery by anesthesia resident.Hypotension was defined as a decrease in pressure by more than 20% of baseline bradycardia was a decrease in HR<45 beats/min.If be stable,any appropriate remedial action was performed/recorded,6when a resident anesthesiologist measured and recorded the sensory-motor block (to ≥ T8) in each group.The sensory block was evaluated with a needle or pinprick every one minute after anesthesia while the motor block was done using Bromage scale,every 5 minutes.14It should be noted that the surgeon started surgery once the sensory-motor block was assessed.The resident anesthesiologist recorded pain scores using visual analog scale (VAS) at recovery and 2,4,6,and 12 hours postoperatively:0 is the lowest,and 10 is the highest.Pethidine (Meperidine) 0.5 mg/kg was given intramuscularly to subjects,at any time postoperatively when the VAS score was>4,15while recording the time to achieve sensory block to T12/L1 and Bromage score of 0/1.Complications like nausea,vomiting and bradycardia,hypotension and dizziness,were recorded,while taking remedial action if a severe one occurred.
Randomization and sequence generation
Permuted balanced block randomization approach stratified by gender was used to allocate patients into groups.17In this method,the size of each block was 6.Allocation concealment was addressed due to the use of balanced block randomization.
Statistical analysis
Data were described as the mean ± standard deviation (SD) or frequency (%) for continuous and categorical variables,respectively.Likelihood ratio chi-square test (to compare the categorical variables) and one way analysis of variance (to compare the continuous variables) followed by Bonferronipost hoctest were used to compare the interested variables among study groups.The statistical software Stata 14.0 (StataCorp.LLC.,College Station,TX,USA) was used to data analysis.APvalue less than 0.05 was considered as statistically significance level.
RESULTS
In this study,90 patients undergoing SA in lower-limb orthopedic surgery were randomly assigned into three groups (n=30/group).Baseline characteristics of participants are compared in Table 1.All three groups were similar in term of age,gender,body mass index,MAP,HR and SaO2at baseline (P>0.05).The similarity of the groups at the beginning of the study demonstrates the success of the randomization process in generating exchangeable groups.
In Table 2,the means of MAP,HR and SaO2among three groups over time were compared.The mean of MAP did not has a significant difference between groups (PGroups=0.155),but its changes over time have been significant (PTimes=0.001),and these changes over time were similar across all three groups (PInteraction=0.147).The mean of HR in groups who received 5 and 10 μg/kg dexmedetomidine was similar but there was mild evidence regarding differences between these groups compared to placebo group (PGroups=0.063) and it seems that the observed difference is clinically important.The trend observed in the means was significantly reduced (PTimes=0.001) and the trend on changes among groups was not similar (PInteraction=0.001) so that the changes in the placebo group were modest,but the changes in intervention groups were significantly reduced.The changes of SaO2between groups was not significant (PGroups=0.650),but their changes over time was significant (PTimes=0.001) and it was different between groups (PInteraction=0.033).
The mean VAS score was significantly less in intervention groups than placebo group (PGroups=0.001) and there was no significant difference (P>0.05) between groups who received 5 and 10 μg/kg dexmedetomidine (Table 3).
According to the Table 3,the onset time of the sensory block (P=0.001),the time to reach the sensory block up to the T8 or higher dermatome (P=0.001),the onset time of the motor block (P=0.001) and time to achieve motor block at D8 or higher dormancy (Bromage Grade 3) (P=0.001) in the group who received 10 μg/kg dexmedetomidine was faster than the other two groups.Time to achieve sensory block at T12 and L1 dermatomes and SA wearing off (P=0.001) and time to achieve Bromage score of 0/1 (P=0.001) in dexmedetomidine 10 μg/kg group was more than that in dexmedetomidine 5 μg/kg group and in the placebo group.
Possible side effects were compared between the threegroups (Table 4).No cases of hypotension,bradycardia,nausea and vomiting and vertigo were observed among the groups.The mean duration of surgery was similar between the three groups and there was no significant difference (P=0.399).However,the need for meperidine injection was significantly higher in the placebo group (P=0.001).

Table 1:Baseline characteristics of participants in placebo,dexmedetomidine 5 μg/kg,and dexmedetomidine 10 μg/kg groups
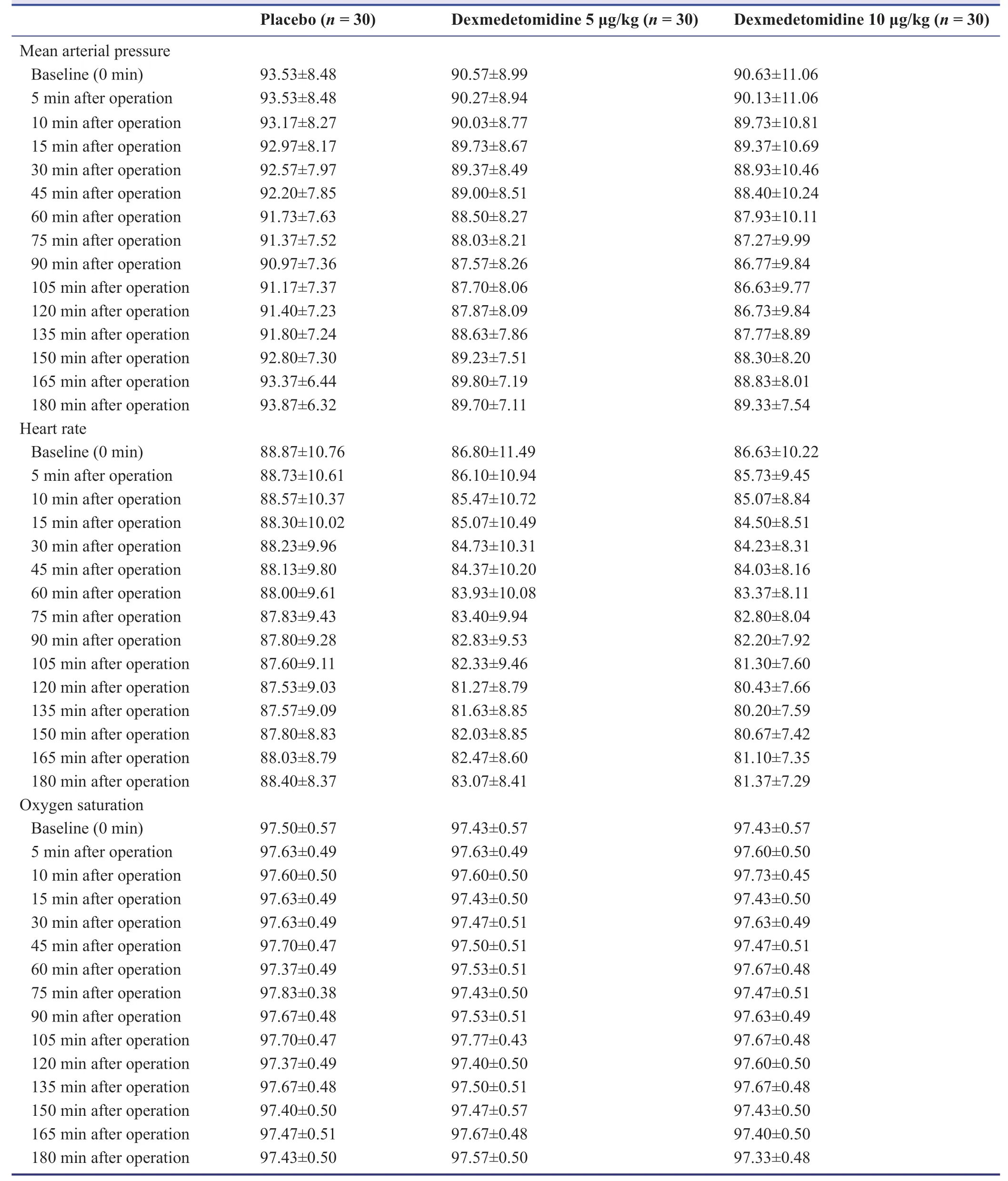
Table 2:Comparison of mean arterial pressure (mmHg),heart rate (beats/min) and oxygen saturation (mmHg) in placebo,dexmedetomidine 5 μg/kg,and dexmedetomidine 10 μg/kg groups over time
DISCUSSION
Regarding the results,no statistically significant difference was found in MAP,HR and SaO2among all groups,but the changes of HR and SaO2over time were different between groups.It means that there is a significant interaction between time and group.The onset time of the sensory block,the time to reach the sensory block up to the T8 or higher dermatome,the onset time of the motor block and time to achieve motor block at D8 or higher dormancy (Bromage Grade 3) in the 10 μg/kg dexmedetomidine group was faster than that in the other two groups.Time to achieve sensory block at T12 and L1 dermatomes and SA wearing off and time to achieve Bromage score of 0/1 in 10 μg/kg dexmedetomidine group was more than that in the 5 μg/kg dexmedetomidine group and in the placebo group.Also,the results showed that the use of dexmedetomidine with different doses resulted in a significant reduction in postoperative mean VAS score.There is no need for meperidine in the groups of 5 and 10 μg/kg dexmedetomidine at the 1sthour postoperatively but 19 cases given 35 mg/kg meperidine in the placebo group need for meperidine at 6 (n=4) and 12 (n=15) hours postoperatively,respectively.

Table 3:Comparison of visual analog scale,sensory and motor block in placebo,dexmedetomidine 5 μg/kg,and dexmedetomidine 10 μg/kg groups
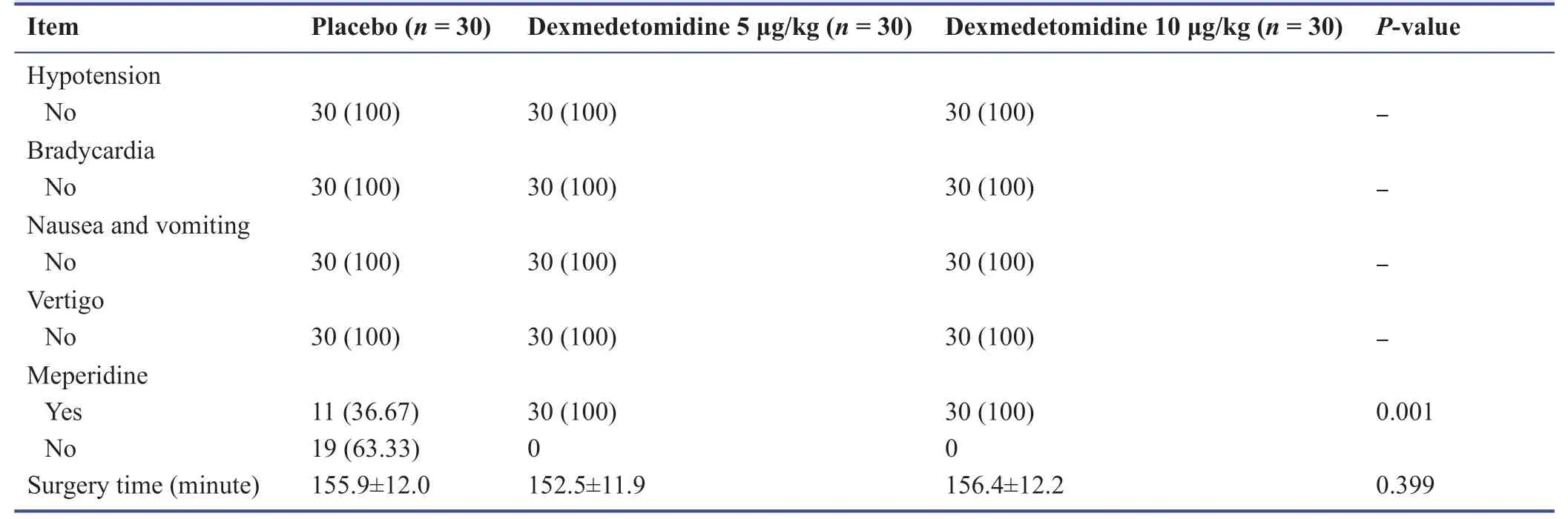
Table 4:Comparison of the frequency of meperidine use,surgery time and postoperative side effects among placebo,dexmedetomidine 5 μg/kg,and dexmedetomidine 10 μg/kg groups
A study of Anderson et al.7aimed at exploring the effective mechanism of dexmedetomidine added once as an adjuvant to ropivacaine in the peripheral nerve block and recorded the duration of block and the first block onset that was longer in the leg receiving dexmedetomidine than the other,and the first onset of sensory block was also faster in the leg receiving dexmedetomidine.They concluded that dexmedetomidine prolongs the duration of block,and their results were supported largely by our trial.
In the Zhang et al.'s study11to assess the effect of different doses of intrathecal dexmedetomidine on SA as a meta-analysis,high-dose dexmedetomidine was considered to be 5-15 μg/kg,while low dose was 2-5 μg/kg.Significant differences were seen in reducing the onset time of the sensory-motor block and prolonging the duration of motor block.Although the risk of bradycardia increased in high-dose dexmedetomidine,high-dose dexmedetomidine prolonged the duration of analgesia and decreased postoperative opioid drugs.They suggested that intrathecal dexmedetomidine prolonged the duration of SA,though increasing the risk of bradycardia at the time,whose results were consistent with ours in which the efficacy of dexmedetomidine 10 μg/kg was more than that of dexmedetomidine 5 μg/kg.
Sharma et al.10launched a study addressing the effect of adding dexmedetomidine to ropivacaine 0.2% for femoral nerve block and fifty subjects were included and randomly assigned to two groups; the dexmedetomidine group received 1.5 μg/kg dexmedetomidine,while the other group given ropivacaine 0.2% and normal saline.The dexmedetomidine group had less pain score and shorter time of first anesthesia,as well as a decreased consumption of anesthetic at 24 and 48 hours,while hemodynamics was not statistically significantly different between the groups.Moreover,they concluded that the addition of dexmedetomidine prolonged the duration of postoperative analgesia and the duration of block in their subjects.Their results were consistent with ours that dexmedetomidine had a proper effect.
Singh et al.12compared different doses of intrathecal dexmedetomidine as an adjuvant to ropivacaine in abdominal surgeries,administering 2.5 mL of ropivacaine added to i) 5 μg/kg dexmedetomidine,ii)10 μg/kg dexmedetomidine and iii) 5 mL normal saline in the control group,and then block factors were compared.The duration of block was higher in the 10 μg/kg group than the control group.The sensory-motor block was higher in the 10 μg/kg goup than the other groups,while hemodynamic changes were stable in all groups.They stated that 10 μg/kg dexmedetomidine would prolong the duration of analgesia without any adverse side effects.Their results were in line with the present study.
Shaikh et al.18carried out a study aimed at the administration of different doses of dexmedetomidine added to bupivacain in abdominal surgeries in two groups:The first received 15 mg of bupivacain 0.5% with normal saline and the other received the same amount of bupivacain with 5 μg/kg dexmedetomidine and then 10 μg/kg dexmedetomidine to a total volume of 3.5 mL,when recording the duration of the sensory-motor block,along with hemodynamic effects and duration of analgesia and side effects.Significant differences were observed in the duration of the sensory block in the 10 μg/kg dexmedetomidine group and that of the motor block with Bromage Grade 3 in the 5 μg/kg dexmedetomidine group,showing that dexmedetomidine prolongs the duration of sensory-motor block.Their results were consistent with our study in terms of favorable effect of dexmedetomidine on sensory and motor block,especially 10 μg/kg dexmedetomidine.
Halder et al.19performed a study to compare the effect of adding different doses of dexmedetomidine as an adjuvant to bupivacain in a subarachnoid block for lower-limb orthopedic surgery.They stated that increasing the dose of dexmedetomidine prolongs the duration of the sensory-motor block and decreases analgesic use.However,hemodynamic indices and side effects were not different between groups.
Mayank et al.20compared three different doses (2.5,5,and 10 μg/kg) of intrathecal dexmedetomidine for SA in lower-limb orthopedic surgery and concluded that the duration of block and analgesia was longer in all three intervention groups.They suggested that the higher dose of dexmedetomidine can cause stronger and more severe effect.
In summary,as the results have shown,the 10 μg/kg dexmedetomidine group is faster in the onset of sensory-motor block,in the time to achieve sensory block to ≥ T8 and to T12/L1 and SA wearing off,as well as in the time to achieve Bromage score of 0/1 and SA wearing off,as compared with the other groups.The Bromage score was greater in the 10 μg/kg group than the other groups,while the VAS score was lower in the 10 μg/kg group than the 5 μg/kg and placebo groups.The placebo group suffered the severest pain.The benefit of increasing dose is to improve the quality of life without any side effects.
Author contributions
Writing the manuscript:LF and HM; revision:HM,AA,BY,AK; drafting:LF,HM,BY,AK and AA.All authors read and approved the final version of the paper for publication.
Conflicts of interest
There is no confl ict of interest.
Financial support
None.
Institutional review board statement
This study as a residency thesis was registered and approved by the Iranian Registry of Clinical Trials (IRCT No.IRCT2017070614056N12) at 2017-07-29.Also this study was approved by Ethical Committee of Arak University of Medical Sciences in 2017 (Ethical Code:IR.ARAKMU.REC.1396.37).
Declaration of patient consent
The authors certify that they have obtained patients or their legal guardians consent forms.In the form,patients or their legal guardians have given their consent for the patients' images and other clinical information to be reported in the journal.The patients or their legal guardians understand that the patients' names and initials not be published and due efforts will be made to conceal their identity,but anonymity cannot be guaranteed.
Reporting statement
The writing and editing of the article was performed in accordance with the CONsolidated Standards of Reporting Trials (CONSORT) Statement.
Biostatistics statement
The statistical methods of this study were reviewed by the biostatistician of Arak University of Medical Sciences,Iran.
Copyright license agreement
The Copyright License Agreement has been signed by all authors before publication.
Data sharing statement
Datasets analyzed during the current study are available from the corresponding author on reasonable request.
Plagiarism check
Checked twice by iThenticate.
Peer review
Externally peer reviewed.
Open access statement
This is an open access journal,and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License,which allows others to remix,tweak,and build upon the work non-commercially,as long as appropriate credit is given and the new creations are licensed under the identical terms.
杂志排行

Medical Gas Research的其它文章
- Pediatric dental sedation
- Premedication effect of melatonin on propofol induction dose for anesthesia,anxiety,orientation and sedation after abdominal surgery:a double-blinded randomized trial
- 2019 International Hydrogen Molecular Medicine Summit
- Minimum alveolar concentration based anesthesia in high altitude and anesthetic overdose:result needs cautious acceptance
- Ozone therapy:a potential therapeutic adjunct for improving female reproductive health
- Clinical utility of hyperbaric oxygen therapy in dentistry