18F-FDG PET/CT for Detecting Vulnerable Carotid Plaque:A Systematic Review of Literatures
2019-04-23PingZhouWeijieXiePingZhengYifanSun
Ping Zhou,Weijie Xie,Ping Zheng ,Yifan Sun
1Institute of Medicinal Plant Development, Chinese Academy of Medical Sciences & Peking Union Medical College,Beijing, China. xwjginseng@126.com; zhoup0520@163.com. 2Department of Gynecology, Chinese Academy of Medical Sciences (CAMS) & Peking Union Medical College Hospital (PUCMH), Beijing, China.3Institute of Medical Information,Chinese Academy of Medical Sciences,Beijing,China.
Introduction
Stroke is one of the leading causes of death worldwide.Nearly 6 million people die from stroke each year,and it is estimated that the lifetime risk for stroke is 8% to 10% [1]. Between 1990 and 2010 the number of strokes increased by 10% in the developing world [2].Ischemic stroke accounts for 85% of all strokes [3],while hemorrhagic stroke accounts for 15% [4]. Risk factors for a vulnerable population include high saturated fat diet, hyperglycemia, insulin resistance,obesity, smoking, air pollution and family history of heart disease, etc [5]. Each of these factors in combination increase the likelihood of incurring carotid plaque even stroke.Unstable carotid plaque can cause acute stroke and heart attack.The morphological changes of unstable plaque is usually shown the inflammation, neo-angiogenesis and calcification lesions [6]. Inflammation occurs in all processes of carotid artery plaques, from plaque formation to rupture [7]. Therefore, identification of the major components that contribute to plaque instability plays an important role in improving the diagnosis and treatment of carotid artery disease and reducing the risk of stroke. Traditional methods of studying carotid plaque include echo color doppler,magnetic resonance imaging,computed tomography,and angiography.
In morphology,the stability of carotid plaque cannot be accurately determined[8].As a matter of fact,given the vulnerability to rupture,vulnerable plaques are still a huge challenge so far [9]. Inflammation, as a substrate or irritant in a chronic or acute environment,especially important in the progression and instability of atherosclerotic plaque, causes subsequent cerebrovascular and cardiovascular events.18F-fluorodeoxyglucose (18F-FDG) is useful for positron emission tomography/computed tomography(PET/CT),and excellent reproducibility was observed during noninvasive quantification [10].18F-FDG PET/CT,represents an emerging morpho-functional technique able to identify highly inflamed and consequently the highest levels of carotid plaque risk [11]. Activated macrophages have an obviously increased metabolic rate, therefore,18F-FDG has higher thermal inclusion than other plaque elements in plaque macrophages,and thus can serve as a biomarker for inflammation of the carotid artery wall,one of the key features of so-called"vulnerable plaques." [12]. Figueroa et al. followed 513 patients without symptomatic cardiovascular disease. One study of 513 asymptomatic patients with cardiovascular disease averaged 4.2 years of clinical studies have shown that18F-FDG uptake within the wall of the ascending aorta was an independent predictor of future cardiovascular events[13].Also the RCT results from the Dublin Carotid Atherosclerosis Stroke Study showed, that carotid plaque inflammation,measured by18F-FDG PET/CT,regardless of the degree of stenosis,it is associated with a high risk of early stroke recurrence[14].
According to published studies on carotid artery plaques,inflammatory processes play a role in the early stages of lesions, which may explain the plaque18F-FDG PET/CT uptake reported by patients with carotid artery plaques [15], had verified the value of18F-FDG as a biologic marker of carotid wall inflammation. The purpose of the present study was to evaluate the relationship between18F-FDG PET/CT results and plaque histological data to assess vulnerabilities of carotid plaque to prevent acute stroke by analysis of the data from the following articles we found.
Methods
Literature search
Searching for relevant articles was conducted using Cochrane library,Web of science,Journal of Nuclear Medicine (JNM), Clinical Nuclear Medicine (CNM) and PubMed. The search included combinations of the following terms:PET/CT;18F-FDG, fluorodeoxyglucose; carotid plaque, limiting studies on human subjects published in English in the last five years.
Data selection
Studies were eligible for inclusion in the analysis based on the following criteria: (a) carotid plaque not other major arteries were evaluated; (b) 18FFDG PET/CT technics were used for diagnosis;and (c) immunohistochemical staining results and standard uptake value(SUV)of carotid plaque can be obtained from the data provided. As showed in Fig. 1, at least two authors double-checked and cor-determined whether the reports fitted were suitable for the inclusion criteria for this study(Fig.1).
Quality assessment
The methodological quality of the eligible studies were independently assessed by two reviewers.And internal validity was assessed to evaluate interpolation,including blind measurement of18FFDG PET/CT without knowledge of reference test,blind measurement of reference test without knowledge of18F-FDG PET/CT.In this systematic review, an assessment of external validity (EV)criteria was adopted to evaluate universality. If sufficient information is provided to determine the prevalence of the results, Jadad's criteria are scored.
Data extraction
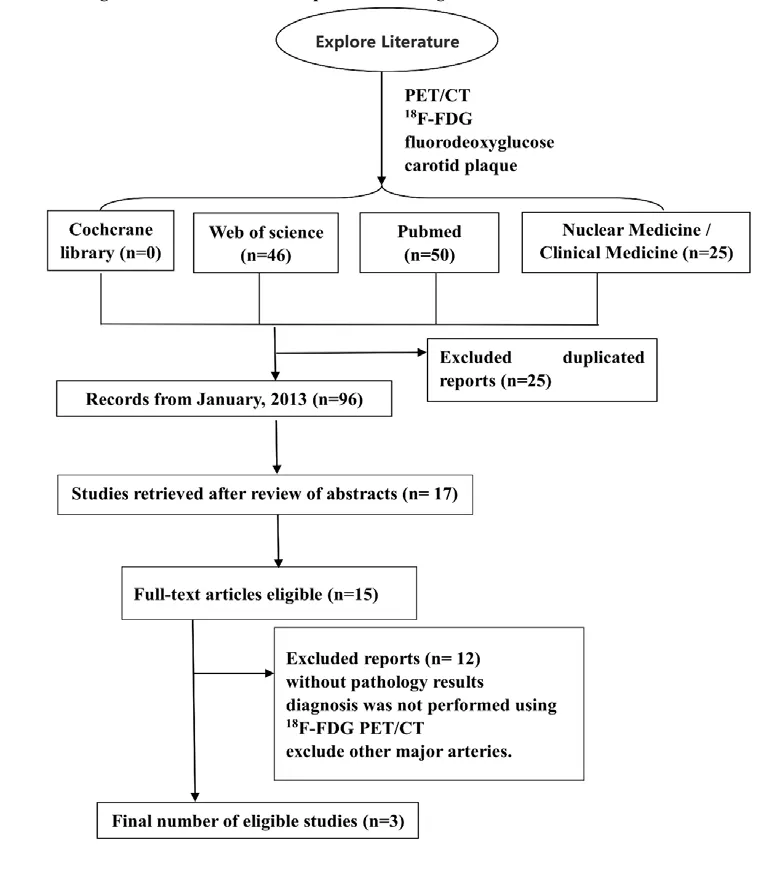
FIG 1 Flow chart of selection processes for eligible studies.(18F-FDG,fluorine-18 2-fluoro-2-deoxy-D-glucose;PET/CT,positron emission tomography/computer tomography)
A data extraction form will be used to collect data.Two authors will independently extract data and take the following aspects into consideration: general information (author name, year of publication and locations and other patient characteristics), study characteristics, eligibility criteria, interventions and outcome measurements. All searched studies will be stored in EndNote software that can assist reviewers to manage data and pick up duplicate publications. Any disagreement will be discussed and finally decided on by a third author.
Results
3 articles were included in the systematic review and form the study population analysis (Fig. 1). The total number of patients identified from the included studies was 89(mean age 70Y,72%male).The mean18F-FDG injected dose was 4.58 MBq/kg. A summary detail was shown in Table 1 and Table 2.
Discussion
A review of variable tracers in carotid plaque imaging has long been published [16]; however,the diagnostic accuracy of18F-FDG PET/CT cannot be determined due to the lack of histological results. Through this study, the systematic evaluation and evaluation of18F-FDG imaging was successfully applied to the prediction of fragile carotid plaque. The last three articles discussed in this review are prospective. The overall results showed that18F-FDG could accurately distinguish fragile and stable carotid atherosclerotic plaques,and accurately image thehighly inflammatory areas in the fragile carotid atherosclerotic plaques through histological analysis.
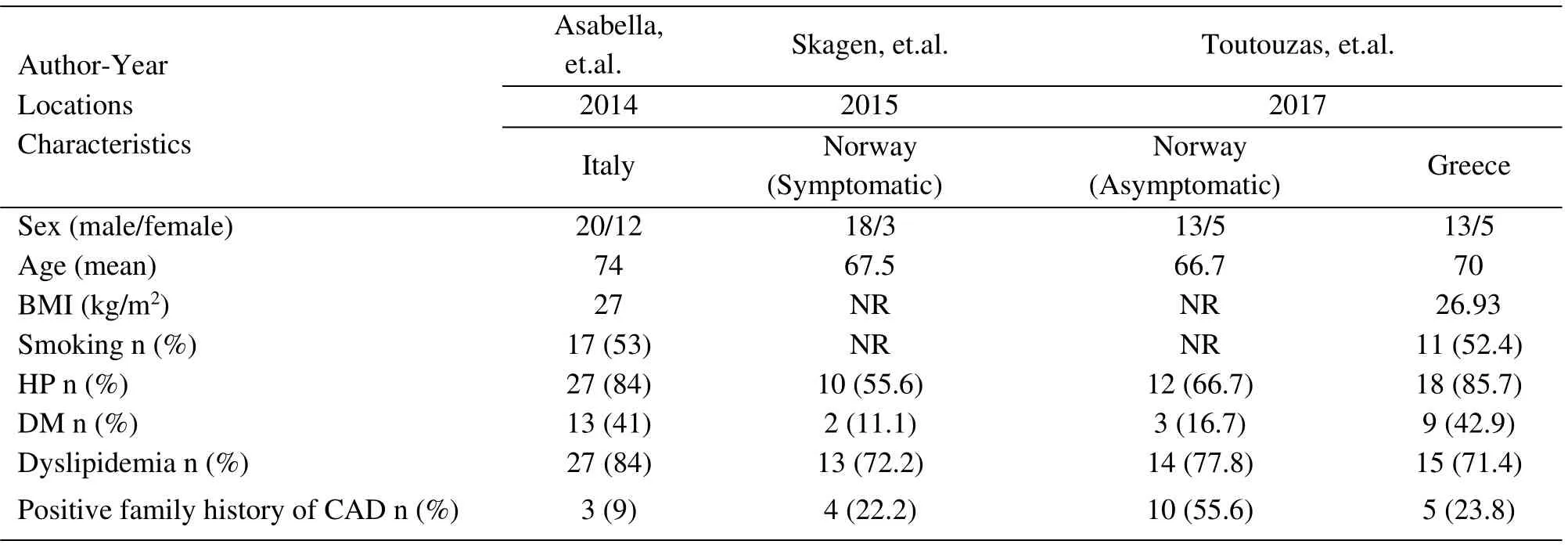
Table 1. Patient characteristics for selected studies from the three articles(HP:hypertension;DM:diabetics;CAD:cardiovascular disease).
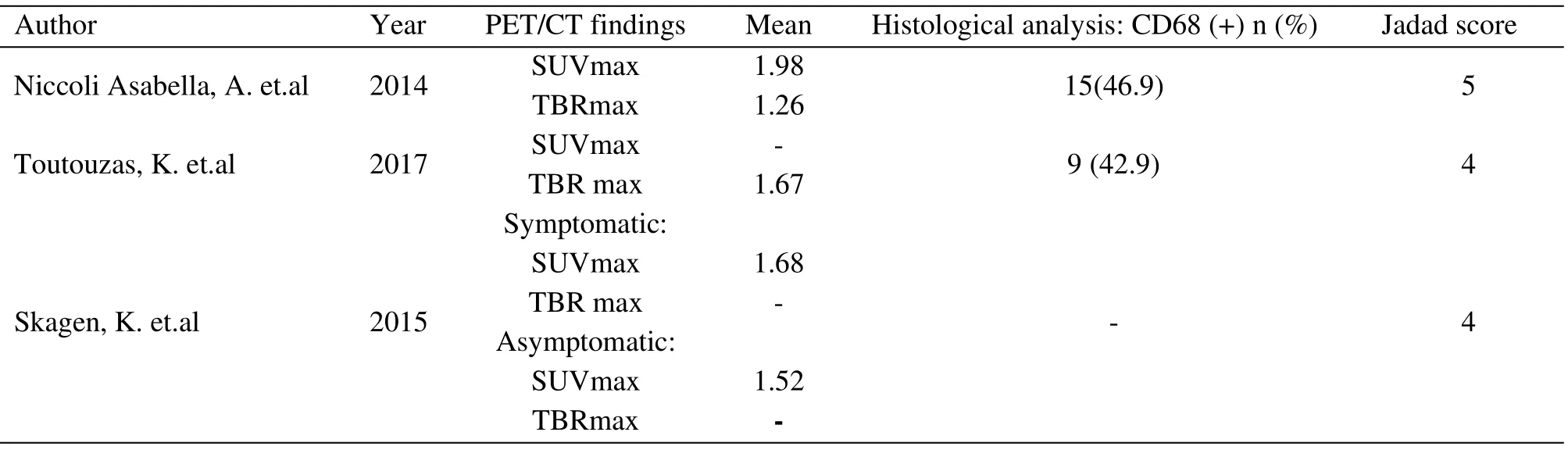
Table 2. Clinical characteristics for selected studies.
The first prospective study was performed to evaluate the role of18F-FDG PET/CT comparing target background ratio(TBR)and standardized uptake value(SUV) with the histopathological inflammatory status of the carotid plaques [8]. The higher SUV max and SUV mean values were observed in patients with inflamed carotid plaques than patients with noninflamed ones, and the results showed no statistical significance. The mean values of TBR max and TBR shows a statistically significant differences between the two groups and carotid artery inflammation (p < 0.01 and p < 0.001, respectively), and resulted higher in patients with inflamed carotid plaques (respectively,1.42±0.32 and 1.34±0.26)than in patients with noninflamed ones (respectively, 1.16 ± 0.19 and 1.03 ±0.20).
All of these researches suggest that TBR (max and mean values) is a more reliable than SUV in the identification of high-risk plaques in particular in patients with high risk of cardiovascular events. To explore the role of PET/CT imaging within the carotid plaque, further studies have continued, and the results found patients with plaques containing increased CD68 expression exhibited higher FDG uptake measurements[11]. The18F-FDG uptake level in plaques and were significantly associated with inflammation level on histological assessment, and18F-FDG uptake was higher in patients with symptomatic compared with asymptomatic carotid artery plaques. Findings were consistent in the final 3 articles. All of these indicated the availability of18F-FDG PET/CT in the detection of vulnerable carotid plaque.
The diagnostic performance showed no significant differences. The more the risk factors,the higher the uptake of18F-FDG. The higher the uptake of18F-FDG, the more vulnerable the plaque is. The percentage of population with hypertension and diabetes mellitus are significantly higher in the articles conducted by Asabella and Toutouzas than the one conducted by Skagen. However, the percentage of population with dyslipidemia and positive family history of cardiovascular adverse diseases hold the opposite results. Although it’s mismatched of some variables in the final 3 articles, the number of risk factors was matched and made little impact on the different results of the articles. However, bias still existed in this study, and the existence of clinical heterogeneity in the study design may affect the universality of the results.Risk factors for a vulnerable population include: hypercholesterolemia, high saturated fat diet, hyperglycemia, insulin resistance,hypertension, smoking, air pollution, obesity, ageing,and family history of heart disease [17]. Since it can detect the cholesterol level of patients and identify patients at risk (so-called vulnerable patients), etc.18FFDG PET/CT of this carotid plaque is of great value[18].In addition,such information can provide positive and effective feedback data for clinical practice. This method improves the traditional ideas and methods of using active statins and anti-inflammatory treatments,and its effect can be verified by endpoint evaluation,such as18F-FDG, PET reduction/CT uptake, and reduction in hard endpoint of major adverse cardiovascular events. As we all know, estrogen is a potential protection factor, decreasing adverse cardiovascular events by improving blood lipid metabolism and lowering cholesterol. However, there is a mismatch in gender ratio in the final 3 articles because the majority were men. This may lead to an underestimated uptake of18F-FDG and the ability to detect vulnerable plaque.
It is worth noting that there are different vulnerable plaque criteria, and the uptake of18F-FDG in plaque refers only to inflammation.The exfoliation with superficial platelet aggregation, thin cap with a large lipid core, crevices of fissure/injury, severe stenosis,superficial calcified nodules, yellow color, endothelial dysfunction, intraplaque hemorrhage and swelling(positive) remodeling are also major / susceptible secondary standard for plaque [19, 20]. The development of a number of novel tracers which identify other pathological processes (hypoxia, neoangiogenesis [21]) alongside more specific markers of inflammation (68Ga-DOTATATE [22]) will continue to enhance the role of molecular imaging. The development of a number of novel tracers will continue to enhance the role of molecular imaging.Such as, some were reported to identify other pathological processes(hypoxia,neo-angiogenesis[21])alongside more specific markers of inflammation(68Ga-DOTATATE [22]). CD68 was mostly expressed on the surface of neutrophils and monocytes/macrophagocyte, which cannot reflect the real inflammation of plaque.In the final 3 selected articles,2 articles just chose the density of CD68 as the index of histological results, while the 3rd article lacked the results. Although the effective extraction data is very limited, the analysis results of this article have provided us with a clue that18F-FDG PET/CT for Detecting Vulnerable Carotid Plaque has great potential.
Finally, we can draw the conclusion by this study that it is available to access vulnerable carotid plaque with18F-FDG-PET/CT and target-background ratio(TBR) is a more reliable parameter than SUV in identifying inflamed plaques.
Recommendations
●Further larger sample size studies should be included to verificate the conclusion.
●Further studies of controls and patients with stable and unstable carotid plaque are needed.
1. Feigin V L, Forouzanfar M H, Krishnamurthi R, et al. Global and regional burden of stroke during 1990-2010: findings from the Global Burden of Disease Study 2010. Lancet, 2014,383:245-254.
2. Lloyd-Jones D, Adams RJ, Brown TM, et al.Heart disease and stroke statistics--2010 update: a report from the American Heart Association.Circulation,2010,121:e46-e215.
3. Iburg, K.M. Global, regional, and national age–sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013:a systematic analysis for the Global Burden of Disease Study 2013.2015.
4. Wang QY1, Liu F, Wu FJ, et al. [Effects of ginsenoside Rg1 on the expressions of peRK1/2 and p-JNK in local cerebral ischemia/reperfusion injury rats]. Chinese Journal of Integrated Traditional & Western Medicine,2013,33:229-234.
5. Orellana MR, Bentourkia M, Sarrhini O, et al.Assessment of inflammation in large arteries with 18F-FDG-PET in elderly. Computerized Medical Imaging & Graphics, 2013, 37: 459-465.
6. Bural, G.G, Torigian DA, Chamroonrat W, et al. FDG-PET is an effective imaging modality to detect and quantify age-related atherosclerosis in large arteries. European Journal of Nuclear Medicine & Molecular Imaging,2008,35:562-569.
7. Skagen K, Johnsrud K, Evensen K, et al.Carotid plaque inflammation assessed with(18)F-FDG PET/CT is higher in symptomatic compared with asymptomatic patients.International Journal of Stroke Official Journal of the International Stroke Society, 2015, 10:730-736.
8. Niccoli Asabella A,Ciccone MM,Cortese F,et al. Higher reliability of 18F-FDG target background ratio compared to standardized uptake value in vulnerable carotid plaque detection: a pilot study. Annals of Nuclear Medicine,2014,28:571-579.
9. Newby, D.E. Triggering of acute myocardial infarction: beyond the vulnerable plaque. Heart,2010,96:1247-1251.
10. Truijman MT, Kwee RM, van Hoof RH, et al.Combined 18F-FDG PET-CT and DCE-MRI to Assess Inflammation and Microvascularization in Atherosclerotic Plaques. Stroke; a journal of cerebral circulation,2013,44:3568-3570.
11. Toutouzas K, Koutagiar I, Benetos G, et al.Inflamed human carotid plaques evaluated by PET/CT exhibit increased temperature: insights from an in vivo study. Eur Heart J Cardiovasc Imaging,2017,18:1236-1244.
12. Strobl FF, Rominger A, Wolpers S, et al. Impact of cardiovascular risk factors on vessel wall inflammation and calcified plaque burden differs across vascular beds: A PET-CT study. Int J Cardiovasc Imaging,2013,29:1899-1908.
13. Figueroa AL, Abdelbaky A, Truong QA, et al.Measurement of arterial activity on routine FDG PET/CT images improves prediction of risk of future CV events. Jacc Cardiovascular Imaging,2013,6:1250-1259.
14. Marnane M, Merwick A, Sheehan OC, et al.Carotid plaque inflammation on 18F-fluorodeoxyglucose positron emission tomography predicts early stroke recurrence.Annals of Neurology,2012,71:709-718.
15. Quirce R, Martínez-Rodríguez I, Banzo I, et al.New insight of functional molecular imaging into the atheroma biology: 18F-NaF and 18F-FDG in symptomatic and asymptomatic carotid plaques after recent CVA. Preliminary results. Clin Physiol Funct Imaging,2016,36:499-503.
16. Pedersen SF,Hag AM,Klausen TL,et al.Positron emission tomography of the vulnerable atherosclerotic plaque in man--a contemporary review. Clinical Physiology & Functional Imaging,2015,34:413-425.
17. Niccoli Asabella A,Ciccone MM,Cortese F,et al.Higher reliability of 18F-FDG target background ratio compared to standardized uptake value in vulnerable carotid plaque detection: a pilot study.Annals of Nuclear Medicine,2014,28:571-579.
18. Nakahara, T, J. Narula, and H.W. Strauss,Molecular Imaging of Vulnerable Plaque.Seminars in Nuclear Medicine,2018,48:291-298.
19. Naghavi M, Libby P, Falk E, et al. From vulnerable plaque to vulnerable patient: a call for new definitions and risk assessment strategies:Part I.Circulation,2003,108:1664-1672.
20. Naghavi M1, Falk E, Hecht HS, et al. From vulnerable plaque to vulnerable patient--Part III:Executive summary of the Screening for Heart Attack Prevention and Education (SHAPE) Task Force report.Am J Cardiol,2006,98:2h-15h.
21. Joshi FR, Manavaki R, Fryer TD, et al.Vascular Imaging With 18 FFluorodeoxyglucose Positron Emission Tomography Is Influenced by Hypoxia.Journal of the American College of Cardiology,2017,69:1873-1874.
22. Tarkin JM, Joshi FR, Evans NR, et al.Detection of Atherosclerotic Inflammation by 68Ga-DOTATATE PET Compared to[18F]FDG PET Imaging. Journal of the American College of Cardiology, 2017, 69:1774-1791.
杂志排行

Clinical Research Communications的其它文章
- A meta-analysis of randomized controlled trials of combined treatment with DGSN and western medicine on diabetic peripheral neuropathy
- A case report of acupuncture of dysphagia caused by herpes zoster virus infection
- Xiaoaiping injection combined with cisplatin and gemcitabine for non-small cell lung cancer:a meta-analysis
- Clinical observation on TCM fumigation and washing for treatment of diabetic peripheral neuropathy by self-made water-washing footbath