Overview of organic anion transporters and organic anion transporter polypeptides and their roles in the liver
2019-04-22TingTingLiJiaXingAnJingYuXuBiGuangTuo
Ting-Ting Li, Jia-Xing An, Jing-Yu Xu, Bi-Guang Tuo
Ting-Ting Li, Jia-Xing An, Jing-Yu Xu, Bi-Guang Tuo, Department of Gastroenterology, Affiliated Hospital, Zunyi Medical University, Zunyi 563100, Guizhou Province, China
Abstract
Key words: Organic anion; Substrate transport; Liver fibrosis; Liver cirrhosis; Liver cancer; Targeted therapy
INTRODUCTION
Organic anions are a general term for a class of materials containing a carbon skeleton with a net negative charge under physiological pH conditions.Both organic anion transporters (OATs) and organic anion transporter polypeptides (OATPs) belong to the SLC family.OATs are classified in the SLC22A superfamily.SLC22 transporters have at least six subfamilies:OAT, OAT-like, OAT-related, organic cation transporter(OCT), organic cation/carnitine transporter (OCTN), and OCT/OCTN-related[1].OATPs are encoded by genes in the SLCO superfamily.This superfamily was originally named SLC21A.In 2004, it was updated and standardized according to phylogenetic relationships.This superfamily was renamed SLCO, the solute carrier family of OATPs[2].OATs and OATPs are important transmembrane transporters that are usually composed of 12 transmembrane polypeptide chains with extracellular glycosylation regions (Figure 1).OATs and OATPs are abundantly expressed in the liver and are mainly distributed on the basolateral membrane.They mediate the transport of a variety of endogenous and exogenous substrates through the cellular membrane[3].The substrates for OATs are small and hydrophilic organic anions such as dicarboxylates and cyclic nucleotides[4], while OATPs transport large hydrophobic organic anions such as bile acids, thyroid hormones, prostaglandins, testosterone, and steroid hormone conjugates.However, they are all involved in the intestinal-hepatic circulation of bile.To maintain this important physiological process, hepatocytes recover bile acids from portal vein blood through some members of the OATP family,such as OATP1B1, OATP1B3, and OATP2B1[5].OAT3, a member of the OAT family,plays a central role in the movement of bile acids through the “gut-liver-kidney” axis and participates in the absorption, metabolism, and excretion of bile acids[6](Figure 2).OATs and OATPs, together with other SLC transporters, play a key role in inter- and intra-tissue molecule communication, in neuroendocrine, growth factor-cytokine, and other homeostatic systems and in the regulation of local and systemic homeostasis[1].In liver disease, such as liver fibrosis, cirrhosis, and liver cancer, the expression of these uptake transporters changes, eventually affecting the rate of endogenous and exogenous drug transport, causing intracellular and extracellular signal transduction dysfunction and increasing the accumulation of metabolites in the plasma.This brief review will summarize our current understanding of the similarities and differences between these two transporter family members, with an emphasis on tissue composition and substrates, regulation of their expression, and their roles in liver diseases.
STRUCTURE AND TISSUE DISTRIBUTION OF OATS AND OATPS
Structure and tissue distribution characteristics of OATs
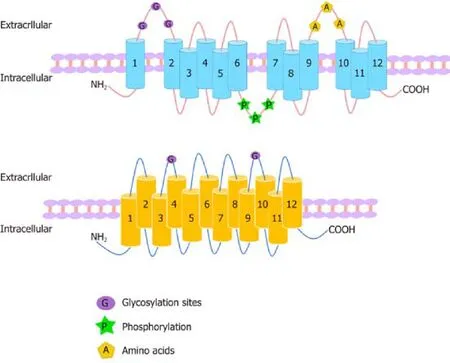
Figure 1 Structures of organic anion transporters and organic anion transporter polypeptides.
The OAT family members have similar membrane topologies[7]and consist of 12 αhelical transmembrane domains (TMD) with three highly conserved regions in their structure that are important for their function:A large extracellular loop with many glycosylation sites between TMD1 and TMD2; a large intracellular loop in the central region between TMD6 and TMD7 with conserved residue phosphorylation; and some motifs in TMD9 and TMD10 with amino acids critical for protein transport activity[8].No specific residues or domains were found to determine the specificity of the substrates, indicating that the three domains are compatible[9].OATs contain 526 to 568 amino acid residues, and the C-terminus and N-terminus of OATs are located in the cell cytoplasm[10,11](Figure 1).There are more than 20 identified human OAT subtypes, which can be divided into three subclades:(1) OAT:OAT1 (SLC22A6),OAT2 (SLC22A7, originally known as novel liver-specific transporters [NLTs])[12],OAT3 (SLC22A8), OAT7 (SLC22A9), OAT5 (SLC22A10), OAT4 (SLC22A11), urate transporter 1 (URAT1; SLC22A12), OAT6 (SLC22A20), SLC22A orphan (S22AO),SLC22A24, OAT8 (SLC22A25, also known as unknown substrate transporter 6[UST6]), SLC22A26, OAT9 (SLC22A27), SLC22A28, SLC22A29, and SLC22A30, which is formed by the best functionally characterized OATs; (2) OAT-like:OAT10(SLC22A1) and organic cation transporter-like 2 (OCTL2; SLC22A14); and (3) OATrelated:BOIT (SLC22A17), ORCTL2 (SLC22A18), Boct2 (SLC22A23), and SLC22A31,the members of which seem to be able to transport organic cations[8,13].Most OATs are highly expressed in the human kidneys and/or liver and are expressed at lower levels in the brain, placenta, prostate, and testis[11].OAT1, OAT2, and OAT3 are located on the basolateral membrane of renal proximal tubule cells, where they are involved in the secretion of drugs and toxins that are subsequently eliminated in urine[14].In contrast, OAT4, OAT10, and URAT1 are expressed on the apical membrane of proximal tubular cells and participate in the reabsorption of substances from tubular fluids[14].OAT2, OAT5, and OAT7 are located on the sinus membrane of hepatocytes and participate in the liver detoxification process[15].Recently, there has been controversy over the main distribution of OAT2.Ohtsukiet al[16]compared the protein expression levels with corresponding mRNA expression levels and activities in 17 human liver samples and found that OAT2 protein expression did not correlate with the corresponding mRNA expression.The difference between the mRNA and protein expression levels may be due to posttranscriptional modification, intracellular trafficking, and/or membrane sorting.Thus, mRNA expression may not be a surrogate marker of transporter function, and as such, the use of it can cause misleading results because some of the transmembrane proteins localize to the membranes of intracellular organelles.Vildhedeet al[17]found that OAT2 protein expression was 30-100-fold lower than that of other liver uptake transporters,including OATP1B1 and OATP1B3.Low OAT2 expression may result in its low activity in the human liver.However, recently, Nakamuraet al[18]adopted a largerscale proteomics approach and determined that the liver expression of OAT2 is comparable to that of OATP.Surprisingly, although it is hypothesized that human OAT2 is located in the sinus membrane of hepatocytes, the immunohistochemical staining for OAT2 protein has not been confirmed in human liver, which is the main organ where it is expressed.In addition, studies have shown that OAT2 is expressed in the embryonic liver, kidney, and other tissues, suggesting a role in the formation and maintenance of these tissues.OAT2 can play an important developmental role independent of its transport function[19].OAT8 (UST6) is a slc22 transporter homolog in flies, worms, and humans, which contributes to the definition of a subfamily within the OATs, the USTs.The expression of UST6 is restricted to the liver in adults and fetuses and may play a role in the development and differentiation of the liver[20].Other OATs include OAT6, which has less pharmacological relevance and are primarily expressed in the olfactory mucosa but not in the kidney or liver, and S22AO and OCTL2, which are poorly understood[21](Table 1).
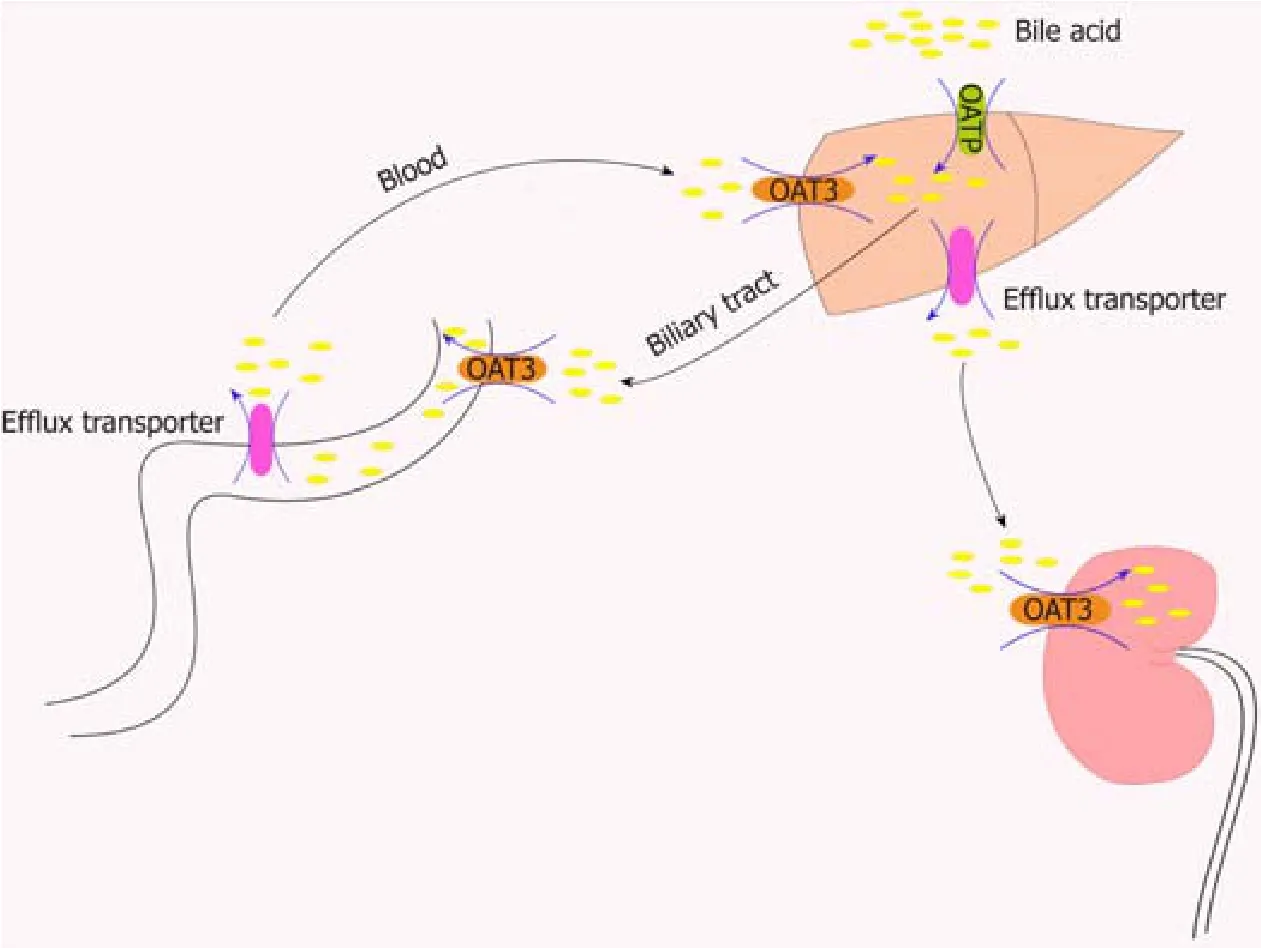
Figure 2 Role of organic anion transporters/organic anion transporter polypeptides in the transport of bile acids through the “intestinal-liver-kidney” axis.
Structure and tissue distribution characteristics of OATPs
OATPs consist of 643-722 amino acids and have 12 transmembrane segments, which can form six extracellular loops and five intracellular loops, and both the C-terminus and N-terminus are located in the cytoplasm[13].OATP1B1 has been shown to be glycosylated in the second and fifth extracellular loops, and the unglycosylated protein remains in the endoplasmic reticulum (Figure 1).Therefore, all mammalian OATPs may be glycosylated in these two extracellular loops.Disulfide bonds can also have an effect on the proper folding and function of these proteins[22].Based on sitedirected mutagenesis of ten conserved cysteine residues in the large extracellular loop 5 of OATP2B1, all ten cysteine residues were determined to be usually disulfidelinked, and these disulfide bonds are the targets important for transporting OATP2B1 to the plasma membrane[23].The OATP family contains 11 members, which share 40%of their amino acid sequence identity.These members show similar structures in their 12 putative transmembrane regions[24].In the human genome, OATPs encoded by the solute carrier OAT (former SLC21) genes constitute an important transporter subfamily that consists of 11 members:OATP1A2 (SLCO1A2), OATP1B1 (SLCO1B1,formerly known as LST-1), OATP1B3 (SLCO1B3, formerly known as LST-2),OATP1C1 (SLCO1C1), OATP2A1 (SLCO2A1, also known as prostaglandin transporter PGT), OATP2B1 (SLCO2B1), OATP3A1 (SLCO3A1), OATP4A1(SLCO4A1), OATP4C1 (SLCO4C1), OATP5A1 (SLCO5A1), and OATP6A1(SLCO6A1)[25].OATPs are expressed in many human organs such as the gastrointestinal tract, liver, kidney, heart, lung, and brain[25]and commonly expressed in various tumors.The OATP1A2 protein is expressed in the cells of the brush border membrane of the duodenal midgut[26], the biliary cells of the liver, the distal nephron of the kidney, and the luminal membrane of the capillary endothelial cells of thebrain[27].OATP1C1 is present in the brain and testis[28].OATP2A1 is expressed in a variety of tissues[4].Its mRNA is found in several tissues, including the brain, colon,heart, kidney, liver, lung, and small intestine[29].Recently, OATP2A1 protein expression has been shown in the gastrointestinal tract, localized to the gastric antrum and the parietal cells of the stomach wall[30].OATP3A1 mRNA expression is high in the brain, heart, and testis, followed by the lung, spleen, peripheral blood leukocytes,and thyroid[31].OATP4A1 mRNA expression is high in the heart and placenta,followed by the lung, liver, skeletal muscle, kidney, and pancreas[32].OATP4C1 is expressed in the kidney, liver, and human colon[33].OATP5A1 is expressed in the fetal brain, prostate, skeletal muscle, and thymus.OATP6A1 is highly expressed in the testis, followed by the spleen, brain, fetal brain, and placenta[34,35].OATP1B1,OATP1B3, and OATP2B1 are mainly expressed in the liver[15].OATP1B1 is expressed in hepatocytes throughout the lobules, and OATP1B3 is mainly expressed around the central vein[36].The mRNA expression level of OATP1B1 in the liver is generally higher than that of OATP1B3[10].The level of OATP2B1 mRNA is highest in the liver,where the protein is located on the basolateral membrane of hepatocytes[37](Table 2).
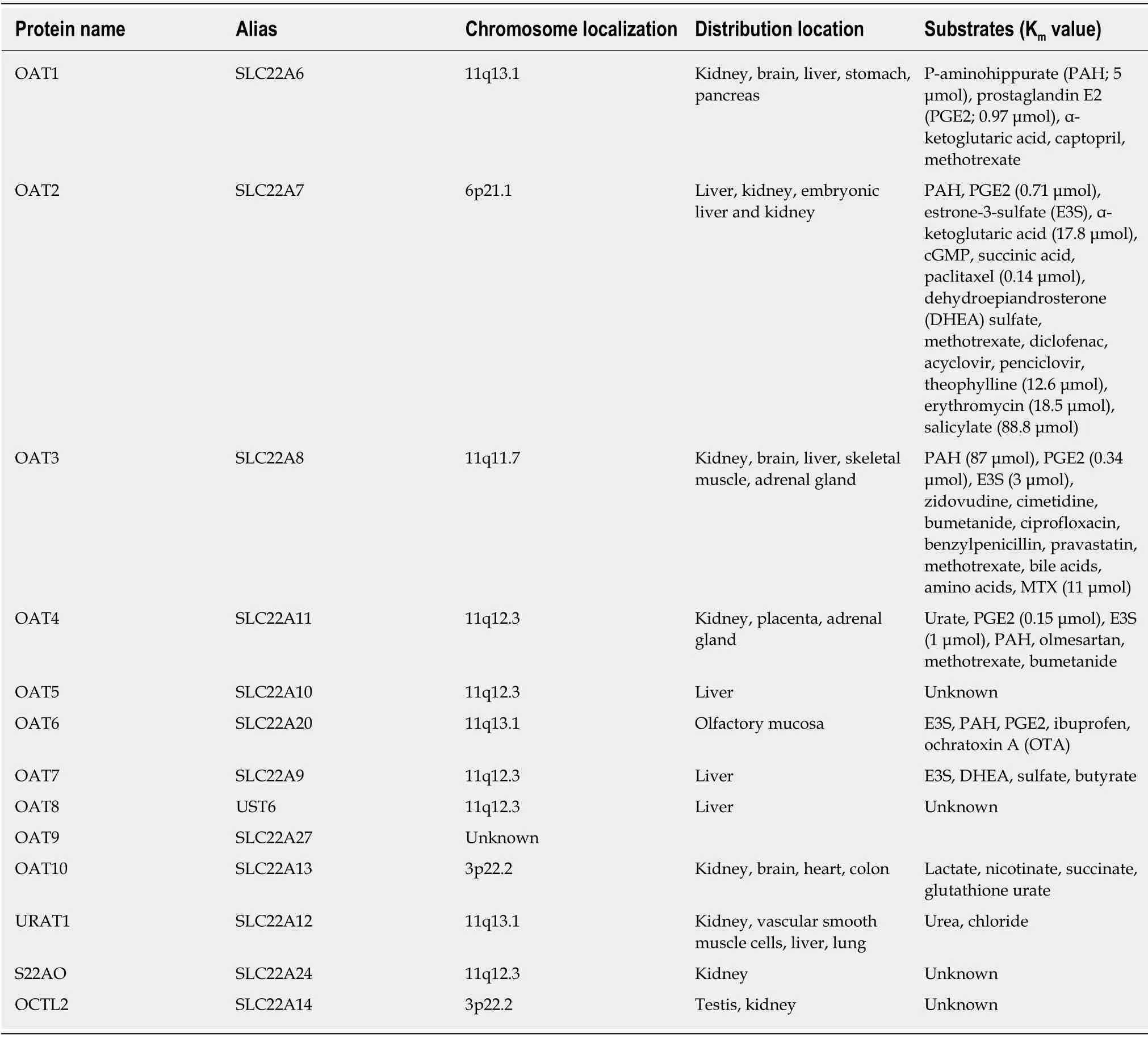
Table 1 Organizational characteristics and substrates of human organic anion transporters[4,14,21,45,63,151,152,153]
OATs and OATPs belong to the SLC superfamily and are anion transporters with 12 transmembrane structures (Figure 1).However, differences in glycosylation sites,amino acid sites, and phosphorylation sites in the transmembrane structure of the OATs and OATPs and the tissue distribution of them lead to differences in substrate apparent affinity (Km) (Tables 1 and 2) and functions.
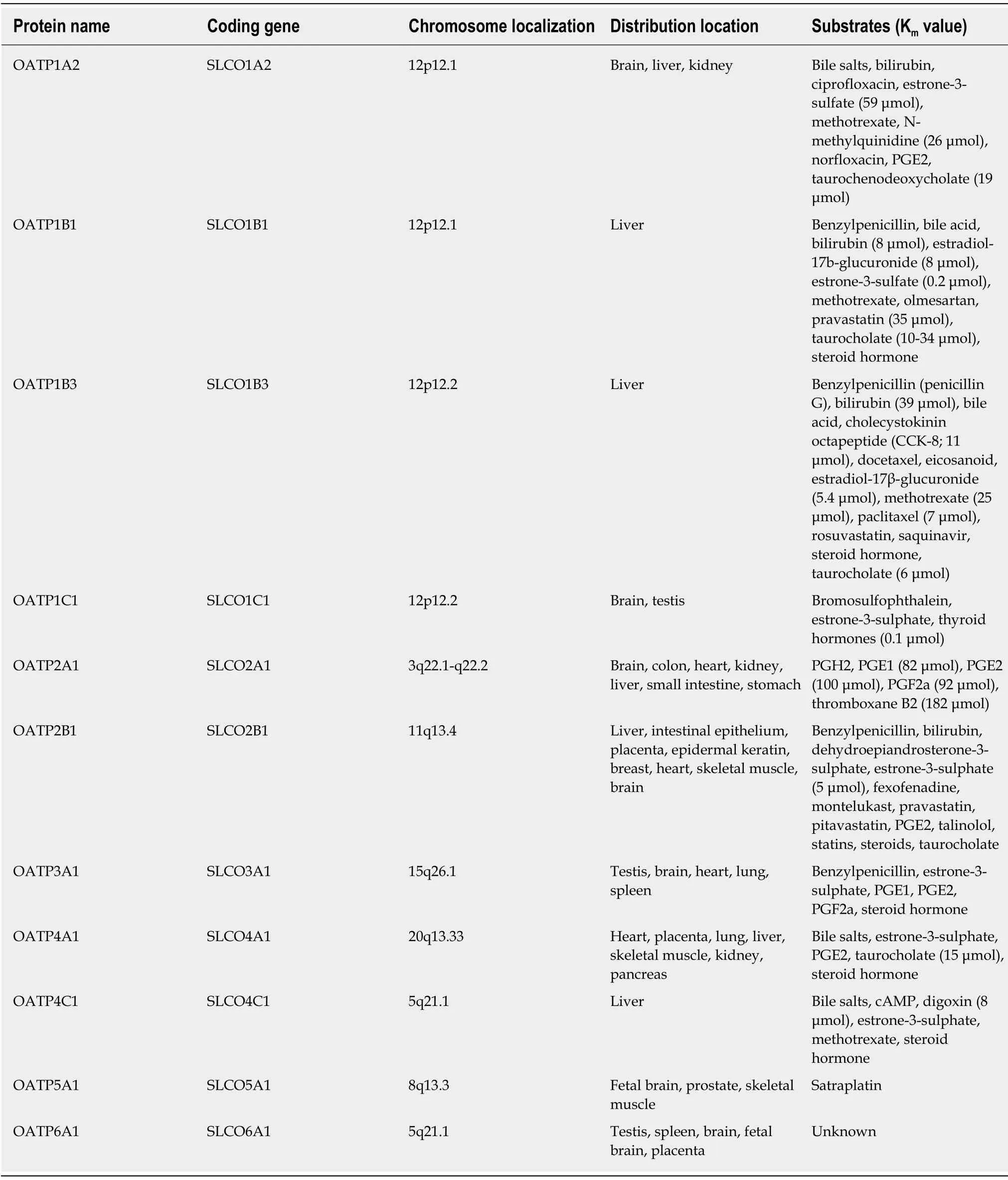
Table 2 Organizational characteristics and substrates of human organic anion transporter polypeptides[4,25,69,73,153,154,155,156]
SUBSTRATE SPECIFICITIES OF OATS AND OATPS
Substrate specificity of OATs
OATs can transport a variety of anionic endogenous metabolites and xenobiotic molecules, including many drugs[21].In 1999, OAT1 was used for the initial functional characterization of a multispecific organic anion-dicarboxylic acid exchanger[38,39].OAT1 plays an important role in the elimination of various toxins in the kidney.In addition to transporting p-aminohippurate (PAH)[40], OAT1 has been shown to transport prostaglandins, a-ketoglutaric acid, NSAIDs, antiviral drugs, and anticancer drugs[39,40].OAT2 was the first mammalian OAT to be cloned.OAT2 was renamed OAT2 due to its close homology to OAT1 and its interaction with organic anions[41].OAT2 has three variants, OAT2-546aa, OAT2-548aa, and OAT2-539aa[42,43].The OAT2-546aa protein is localized on the plasma membrane, and the OAT2-548aa protein is localized to the intracellular compartment.The OAT2-539aa differs greatly from OAT2-546aa and OAT2-548aa because the C-termini are significantly different between species[44].Different variants have different substrate specificities.Many previously identified OAT2-548aa substrates, such as PAH, estrone-3-sulfate (E3S),alpha-ketoglutarate, succinic acid, paclitaxel, and dehydroepiandrosterone (DHEA)sulfate, are not transported by OAT2-546aa[45].OAT2-546aa was found to be capable of transporting guanine nucleotide-related compounds and cGMP[44], as well as other endogenous substrates, suggesting that OAT2 may play a regulatory role in intracellular signaling[45].OAT2 is an important determinant of drug elimination due to the expression of OAT2 in the liver and its ability to transport and hence affect the deposition of multiple pharmacologically active agents[21].Therefore, some antitumor drugs interfere with OAT2-mediated transport, while others, such as methotrexate[46]or irinotecan[47], are substrates for this transporter.In addition, the drug substrates of OAT2 also include many antibiotics[48,49], antimetabolites[46,50], H-2 receptor antagonists[51], diuretic agents[49], nonsteroidal anti-inflammatory drugs[52], and antiviral drugs[53].Many of the substrates of OAT2 are also substrates of OAT1 and/or OAT3.Notably, the three OAT2 splice variants OAT2-546aa, OAT-548aa, and OAT2-539aa with different transport specificities have been used in different laboratories and have resulted in conflicting findings[45].OAT1 and OAT3 have similar specific drug substrates.However, it is not clear whether they have similar specific endogenous substrates[6].Typically, the substrates of OAT3 are bulkier and more lipophilic than those of OAT1.OAT3 can transport E3S[54], zidovudine[55], cimetidine[51],diuretics[56], antibiotics[57], and statins such as methotrexate[58].In addition, Bushet al[6]demonstrated that OAT3 is involved in the bile acid (Figure 2) and lipid metabolism pathways.OAT4 is unique in that it can absorb and transport certain substrates, such as urate and steroid sulfates (such as E3S)[59,60], but is an efflux transporter for other substances, such as PAH and olmesartan[61].Little is known about human OAT5,although Northern blot analysis has shown mRNA expression in the liver[46].Mouse and rat oat5 (Slc22a19) proteins have been shown to be expressed only in the kidney[62]and are improbable homologs of the human OAT5 protein[7].OAT6 is capable of interacting with a variety of small organic anions of physiological, pharmacological,and toxicological significance, such as estrone sulfate, PAH, and prostaglandin E2(PG-E2).The preferred ligand for this transporter is an odor molecule[63].OAT7 is highly expressed in the liver.It transports butyric acid and other short-chain fatty acids into hepatocytes and affects the pathway of short-chain fatty acid metabolism but does not promote hepatocyte uptake of bile acids[11,64].In addition, OAT7 may be critical for the release of steroid hormones such as estrogen-3-sulfate into the bloodstream.Impaired function of OAT7 may result in slower metabolism of shortchain fatty acids and impaired steroid responses[11].OAT10 acts as an antiporter and exchanges extracellular nicotinate with intracellular lactate, nicotinate, succinate, or glutathione[65].URAT1 was originally cloned as a “renal specific transporter (Rst)”,and the human homolog transported urate; therefore, it was named “urate transporter 1 (URAT1)”[66].URAT1 is similar to other family members and operates as an anion exchanger.URAT1 can transport urea and chloride[66,67](Table 1).
Substrate specificity of OATPs
Most OATPs transport a wide range of compounds.Although most substrates are anionic, some OATPs can also transport neutral and ionic compounds[68].Typically,the substrate is an amphiphilic molecule with a molecular weight greater than 350 Daltons, including bile acids, conjugated steroids, thyroid hormones, linear and cyclic peptides and mushroom toxins, and many drugs, including statins, sartans,antibiotics, and antitumor drugs[4].Many of these compounds are substrates for a variety of OATPs.For example, both OATP1B1 and OATP1B3 regulate the transport of bile acids, eicosanoids, peptides, and some drugs, including the antitumor drug methotrexate[69].It has been reported that OATP-mediated transport may be affected by pH.Some studies have shown that OATP2B1 transport activity increases in acidic pH conditions[70-72].Under normal physiological pH, OATP2B1 transports estrone and DHEA though the membranes, while under acidic conditions, it can transport many other compounds such as taurocholate, bilirubin, fexofenadine, statins, and it is also a transporter of steroids that increases the amount of estradiol in tumor cells[73,74](Table 2).
Although the substrates of OATs are mainly small hydrophilic organic anions,OATPs mainly transport large hydrophobic organic anions.However, many members of OAT and OATP families are capable of transporting the same endogenous substrates such as PG-E2 (transported by OAT1, OAT6, and OATP1A2) and E3S(transported by OAT2, OAT3, OAT4, OAT6, OAT7, OATP1A2, OATP1B1, OATP1C1,OATP2B1, OATP3A1, OATP4A1, and OATP4C1), and exogenous drugs such as benzylpenicillin (transported by OAT3, OATP1B1, and OATP2B1), ciprofloxacin(transported by OAT3 and OATP1A2), diclofenac (transported by OAT2 and OATP1B3), methotrexate (transported by OAT1, OAT2, OAT3, OAT4, OATP1A2,OATP1B1, OATP1B3, and OATP4C1), olmesartan (transported by OAT1, OAT4, and OATP1B1), paclitaxel (transported by OAT2 and OATP1B3), and pravastatin(transported by OAT3, OATP1B1, OATP1B1, and OATP2B1)[4,14,21,45,63,69,73].
OATS AND OATPS IN LIVER DISEASE
OATs in liver disease
In liver fibrosis and cirrhosis, scar tissue spreads throughout the liver, which may result in a decrease in membrane protein.Changes in the liver uptake transporter OAT2 can have a profound impact on the pharmacokinetics (PKs) of drugs administered to patients with liver cirrhosis, which may result in unexpected adverse effects and/or potential changes in drug efficacy[75,76].For example, downregulation of OAT2 may affect liver uptake of entecavir.Entecavir, a guanosine cyclopentanoate analog, is a first-line drug used for hepatitis B and has a significant effect against hepatitis B virus (HBV) by inhibiting HBV polymerase[77].Entecavir needs to be organized in the liver to act as an anti-HBV agent.Previous studies have shown that entecavir is a substrate for OAT 1/3[78].Xuet al[78]first reported that liver fibrosis causes changes in the distribution of entecavir in the liver, and after liver fibrosis, the ability of the intestine to transport entecavir to the liver is significantly reduced due to the downregulation of OAT2[79], ultimately reducing the distribution of entecavir in the liver.In addition, studies have found that there are increased plasma hepatocyte growth factor (HGF) levels in patients with hepatic failure or liver cirrhosis[80].HGF is a ligand of the c-Met membrane receptor tyrosine kinase and a potent stimulator of DNA synthesis in hepatocytes, contributing to liver regeneration[81,82].Leet al[83]found that HGF (20 ng/mL) treatment for 48 h downregulated OAT2 mRNA levels.OAT2 downregulation may affect the liver’s transport of endogenous substances or drugs,thereby further promoting the development of cirrhosis.Besides, a non-alcoholic steatohepatitis (NASH) rat model induced by methionine-choline deficiency showed that two different stages of non-alcoholic fatty liver disease (NAFLD; simple fatty liver and more serious NASH) would lead to decreased liver uptake of transporter,such as OAT2, OAT3, OATP1a1, and OATP1b2.Furthermore, NAFLD may alter the plasma retention time of clinically relevant drugs that are dependent on these transporters and may increase potential drug toxicity.The impact of NAFLD on human hepatic uptake transporters is the focus of ongoing research[84].
The hepatitis-fibrosis-cirrhosis progression eventually leads to liver cancer.Hepatocellular carcinoma (HCC) is the most common primary liver cancer, and HCC patients have a poor prognosis.Enhanced surveillance of hepatitis/fibrosis/cirrhosis patients and additional risk analysis are important to prevent the development of HCC.OAT2 is not only an important independent risk factor for HCC but also the best predictor in the HCC recurrence index MO.Yasuiet al[85]examined the association betweende novoHCC development and OAT2 expression at baseline in 38 patients with hepatitis C without HCC who subsequently developed HCC, whose age, gender, and fibrosis stage data were matched with those of 76 hepatitis C patients who did not develop HCC.It was found that a decrease in the expression of OAT2 in the liver indicates a high risk of HCC for patients with chronic hepatitis C regardless of other risk factors[85].Based on current data, assessment of the transporter function from liver biopsy samples provides additional valuable predictors.In addition, serum albumin levels differ in patients with and without HCC, with serum albumin level of 4.0 g/dL being a critical predictor of HCC development.Low serum albumin levels constituted an independent risk factor for HCC development in patients matched by age, gender, and liver fibrosis stage[84].Nonetheless, in patients with higher serum albumin levels (≥4.0 g/dL), decreased expression of OAT2 remained an important independent risk factor for HCC development[85].A study showed that OAT2 is responsible for the uptake of orotic acid[86], which is reported to promote liver carcinogenesis[87,88].In a clinical setting, orotic aciduria was also detected in HCC patients without cirrhosis[89].Furthermore, gene set enrichment analysis showed that OAT2 expression was significantly associated with mitochondrial oxidoreductase activity and fatty acid metabolism.Mitochondrial dysfunction and oxidative stress are considered to be key mechanisms for the development of HCC[85].Taken together, the results from these studies suggest that reduced OAT2 expression may contribute to liver cancer by increasing the concentration of orotate around hepatocytes and promoting oxidative stress and mitochondrial dysfunction.It has been hypothesized that these microenvironmental changes may occur in patients with early chronic HCV infection[85].In fact, the precise mechanism of the association between OAT2 expression and HCC development requires further investigation.Clinically, OAT2 may be a predictive tool for HCC, and patients with reduced expression of OAT2 and reduced serum albumin levels are candidates for enhanced HCC surveillance, even if they do not exhibit risk factors for HCC.In addition, OAT2 and UST6 expressed in the embryonic liver may indicate involvement in liver differentiation and development.They may play a distinct role in the formation and maintenance of liver tissues.Although their most likely role seems to be in the transport of organic molecules, it is also conceivable that they have a role in an independent transport function[20].These speculations lead to the prediction that the high expression of embryonic OAT2 and UST6 is likely to be interesting in the context of cancer occurrence and regeneration.However, these effects have not been analyzed in detail, and their roles as embryonic transporters require further study.
HCC is an aggressive malignancy primarily due to tumor metastasis or recurrence,even after potentially curative treatment.Intrahepatic recurrence after hepatectomy for HCC includes intrahepatic metastasis (IM) and multicenter occurrence (MO)[89].The following MO criteria are defined as HCC characteristics:(1) Recurrent tumors consist of well-differentiated HCC cells that are found in different liver segments and were moderately or poorly differentiated in the previous HCC case; (2) Primary and recurrent tumors have well differentiated HCC cells; (3) Recurrent tumors include areas of dysplastic nodules in the peripheral zone; and (4) Multiple HCCs have a nodule of well-differentiated HCC cells and contain some nodules consisting of moderately or poorly differentiated HCC cells.MO is a type of intrahepatic HCC recurrence, in which the new HCC lesions are formed due to chronic liver disease,and the extant noncancerous liver tissue with oncogenic potential may explain the risk of MO after hepatectomy[90].It is unclear how liver dysfunction involving OAT failure leads to the development of HCC.Studies have focused on elucidating the relationship between liver dysfunction and MO after radical hepatectomy.According to the Gene Ontology database (GO:0015711) of theOATgenes for hepatocyte function, the best predictor of HCC MO is OAT2[91].Kudoet al[91]first elucidated the relationship between HCC and OAT2 expression in noncancerous liver tissues.They examined 49 noncancerous liver tissues from Milanese patients with standard HCC and found that high OAT2 expression prevented HCC after hepatectomy [odds ratio(OR) = 0.2;P= 0.004].In contrast, a new HCC may occur 1 year after hepatectomy in patients with low OAT2 expression[91].
OATPs in liver disease
There are many types of cirrhosis, including primary biliary cirrhosis (PBC), alcoholic cirrhosis, and hepatitis C virus (HCV)-related cirrhosis.The expression of OATP in different types of cirrhosis differs.In alcoholic cirrhosis, although the expression of OATP1B1 and OATP1B3 is decreased, the expression of OATP2B1 is increased[92].In PBC, uptake transporter expression is similar to that observed in the alcoholic cirrhotic liver[93,94].Ogasawaraet al[95]found a significant decrease in mRNA expression of OATP1B1, OATP1B3, and OATP2B1 in HCV-associated cirrhosis.However, Wanget al[92]found that the expression of OATP1B1 and 2B1 increased in HCV-associated cirrhotic liver.The reasons for these differences are not clear, but they may reflect ethnic differences (liver tissues from Japanese patients compared with those from Caucasian patients), endpoints (expression of mRNA and protein), disease severity, or sample size.This difference could also be due to different mechanisms of alcohol transporter regulation in the livers affected by the HCVvsthat from livers affected by PBC.In addition, studies have shown that OATP1B1-mediated transport determines the rate of repaglinide uptake in the liver[96].Hatorpet al[97]found that repaglinide plasma absorption increased four-fold in patients with cirrhosis, as determined by the area under the curve.This increase may be due to a decrease in the expression of OATP1B1[98].The PKs of drugs for hepatobiliary transporter clearance vary between patients with different types of cirrhosis and liver fibrosis, and patients should be differentiated in clinical PK studies.
OATPs, especially OATP1B3, play an increasingly important role in detecting liver diseases.Gd-EOB-DTPA-enhanced MRI (EOB-MRI) is increasingly used to detect and assess liver lesions[99].It was found that OATP1B3 expression was associated with an increase in EOB-MRI, indicating that it transports Gd-EOB-DTPA into HCC cells.It is generally believed that 85% of HCCs emit a low signal in the hepatobiliary phase of Gd-EOB-MRI compared to the noncancerous liver background, and the expression of OATP1B3 is reduced in tumors[100,101].Gd-EOB-DTPA can be used to assess the vascular distribution of liver lesions and the activity of the OAT OATP1B3 to further understand the prognosis of the disease.Yamashitaet al[102]found that EOB-MRI combined with serum alpha-fetoprotein (AFP) status reflects the stem/maturation status of HCC determined with different biological and prognostic information.Moreover, upregulation of OATP1B3 increased the uptake of Gd-EOB DTPA in the hepatobiliary phase and downregulated the low levels of serum AFP, an outcome that was associated with the maintenance of hepatocyte function and good prognosis.In contrast, HCC cells showed reduced Gd-EOB-DTPA uptake that was associated with high serum AFP levels, poor prognosis, and activation of the oncogene FOXM1[102].In addition, the identification of specific subclasses to which the tumor belonged prior to treatment informs the molecular targeted drug therapy.Activation of the Wnt/βcatenin signaling pathway has been identified as an important molecular marker in HCC and has been used to define specific HCC subclasses[103].Studies have found that HCC with OATP1B3 upregulation is a good candidate for inclusion into a specific subclass of Wnt/β-catenin-activated HCC.Defining an OATP1B3-upregulated HCC subclass would be useful in the current era in which molecular targeted therapies are rapidly developed, particularly with the advantage of being able to classify tumors noninvasively using EOB-MRI[103].In addition to being the most useful imaging modality for diagnosing HCC, Gd-EOB DTPA may be a very useful tool for detecting and describing pathological sinus syndrome, also known as hepatic venous occlusive disease, at a relatively early stage[104].It has been reported that Gd-EOB-DTPA can also be used to distinguish some liver diseases that are otherwise difficult to distinguish,such as focal nodular hyperplasia of alcoholic cirrhosis and HCC[105].Recently, studies have classified OATP1B3 into two types:(Lt)-OATP1B3 (hepatic type specifically expressed in the human liver) and (Ct) OATP1B3 (cancer type identified in colon cancer, lung cancer, and pancreatic cancer tissues and cell lines).Lt-OATP1B3 and Ct-OATP1B3 have different transport functions and membrane localization characteristics.Lt-OATP1B3 is mainly expressed on the plasma membrane, while Ct-OATP1B3 is mainly retained in the cytosol[106].Lt-OATP1B3 has significantly higher transport activity than Ct-OATP1B3 does.The expression and role of Lt-OATP1B3 in drug treatments are beneficial for drug deposition in the liver[107].The characterization of extrahepatic expression of Lt-OATP1B3 in cancer expands our understanding of the potential role of OATP1B3 in the influx of OATP1B3 substrates serving as anticancer drugs in cancer cells.Lt-OATP1B3 mediates the uptake of many clinically important anticancer drugs[108-111].Therefore, understanding the specific Lt-OATP1B3 expression in cancer has potential clinical relevance for cancer treatment.Future studies will need to compare the relationship between the appropriate levels of Lt-OATP1B3 and Ct-OATP1B3 expression in liver tissue.
In addition, studies have shown that decreased expression of OATP is significantly associated with HCC-related death after relapse.Vasuriet al[112]correlated the expression of OATP1B1 and OATP1B3 with HCC morphological features and the expression of bile keratin K7 and K19 [associated with a poor prognosis after orthotopic liver transplantation (OLT)] by observing the liver of 69 patients with HCC liver transplantation (OLT).OATP1B1 and OATP1B3 were hepatocyte-specific, while bile cells and biliary malignancies were always negative[113].The phenotypic expression of K19 implied a major risk of repaid recurrence and poor overall prognosis[114].They found a significant negative correlation between OATP and K7 and K19 expression (P< 0.001).In HCC patients with K7 and/or K19 positive expression, the OATP detection was always negative.Thus, there is an inverse correlation between OATP expression on the basolateral hepatocyte membrane and a biliary “phenotype” determined for the same hepatocytes.Although the meaning of this correlation is unclear, since OATP and keratin are molecules that have different functions and intracellular localizations, these findings seem to support the existence of morphological profiles for hepatic malignancies[112].
OATs and OATPs play important roles in a series of diseases, such as hepatitis,liver fibrosis, cirrhosis, and liver cancer.When liver diseases occur, changes in the expression of OATs and OATPs reduce the uptake of many drugs in the liver, such as entecavir and repaglinide, which ultimately has a profound impact on the PKs of drugs, including an increase in side effects.OATs and OATPs are closely related to the occurrence, recurrence, and prognosis of HCC.They can be used as important indicators to predict, detect, and distinguish different liver diseases.
REGULATION OF OAT AND OATP EXPRESSION IN THE LIVER
Regulation of OAT expression in the liver
The expression of OATs is regulated by a variety of transcription factors.Hepatocyte nuclear factors (HNFs) constitute a class of transcription factors that regulate genespecific expression in the liver.These transcription factors and their interactions constitute a complex regulatory network that precisely controls liver development and hepatocyte function.HNF-1a plays an important role in regulating a variety of hepatocyte-specific genes, although it is also expressed in other tissues[115].HNF-1α and/or HNF-1β were previously reported to increase the promoter activity ofOAT3[116]and affect the expression of URAT1 in the kidney[117].Kleinet al[115]showed that HNF-1a is able to increase human hepatocyteOAT5andOAT7promoter activities, and HNF-1a binds to two functional binding elements in the proximalOAT5promoter and binds to one element in theOAT7promoter; this binding is critical for the HNF-1α-mediated increase in promoter activities in liver-derived cells.They found a decrease inOAT5andOAT7mRNA expression when endogenous HNF-1a was knocked down[115].In contrast, humanOAT1andOAT2mRNA expression was not affected by the regulation of HNF-1a expression levels in hepatic cell lines.HumanOAT1[118]andOAT2[119]promoter activities are increased by another liver-enriched transcription factor:HNF-4a, which is in the nuclear receptor family and is known to have an indispensable role in hepatocyte differentiation and the maintenance of liver gene expression.Target genes encode proteins involved in a variety of physiological processes, particularly cholesterol and glucose metabolism[120-122].HNF-4ais also a gene encoding a transcriptional regulator of HNF-1a[123].Through a computer analysis of the 5’ flanking regions of theOAT2gene,Popowskiet al[119]identified a common binding site for the liver-enriched HNF-4a between 329 and 317 nt upstream of the transcription initiation site.It was found that HNF-4α is involved in the transactivation of theOAT2promoter, whereas chenodeoxycholic acid (CDCA) reduces the transactivation potential of HNF-4a and thereby inhibits the expression of endogenousOAT2mRNA in Huh7 cells[119].It is well known that HNF plays an important role in bile acid metabolism and transport through the transcriptional control of specific genes[124].A primary bile acid, CDCA,and secondary bile acids, deoxycholic acid (DCA) and lithocholic acid (LCA), have been identified as endogenous ligands and effective activators of farnesoid X receptor(FXR)[125].FXR is considered to play a key role in bile acid feedback regulation systems[126].Bile acids enhance the transactivation ability of FXR, which results in the induction of FXR target genes, such as the transcriptional repressor SHP[127].SHP is an orphaned member of the nuclear receptor family that inhibits other DNA-binding transcription factors, such as HNF-4a[128], through protein-protein interactions[129].Overexpression of the FXR-induced transcriptional repressor SHP can counteract HNF-4α-mediated endogenous activity.In addition to acting through a SHPdependent mechanism, FXR may directly bind to a negative response element located in theHNF-4apromoter[130,131], thereby counteracting HNF-4α-mediatedOAT2promoter activation (Figure 3).
Regulation of OATP expression in the liver
In addition to certain members of the OAT family, promoter regions of otherOATPgenes, such asOATP1B1andOATP1B3, have also been shown to be regulated by HNF[132].Studies have shown that theOATP1B1proximal promoter contains a functional HNF1a response element that is responsible for the expression of liver OATP1B1[132,133].In human hepatoma cell lines, HepG2 and Huh7, bile acids, including CDCA, DCA, LCA, cholic acid, and ursodeoxycholic acid (UDCA), were shown to inhibit HNF1a-mediatedOATP1B1gene activation through a cascade reaction.In this cascade, theHNF-1apromoter is regulated by HNF-4a, and SHP negatively targets HNF-4a (HNF-4a is a common target for SHP), thereby downregulating HNF-1a activity and ultimately inhibiting OATP1B3[132].Studies have found that UDCA increased the exposure of rosuvastatin and serum bilirubin in 12 healthy volunteers,probably because UDCA inhibited the transcription factor HNF1a and decreased the expression of the OATP1B1 transporter, which affected the liver uptake of sulvastatin and serum bilirubin[133].Previous studies have reported that transcription of theOATP1B3gene is regulated by three transcription factors:FXR, HNF1α, and HNF3β.Liver-specific expression of OATP1B3 is highly dependent on the liver-rich transcription factors HNF1α and HNF3β, and its expression is upregulated by CDCA and DCAviaFXR[126].In addition, some studies have reported that HNF4α interacts with β-catenin to promote the expression of hepatocyte target genes[134], such asOATP1B3[135].This interaction is attenuated when the activity of HNF4α is inhibited(Figure 3).
OATS AND OATPS IN THE TREATMENT OF LIVER DISEASE
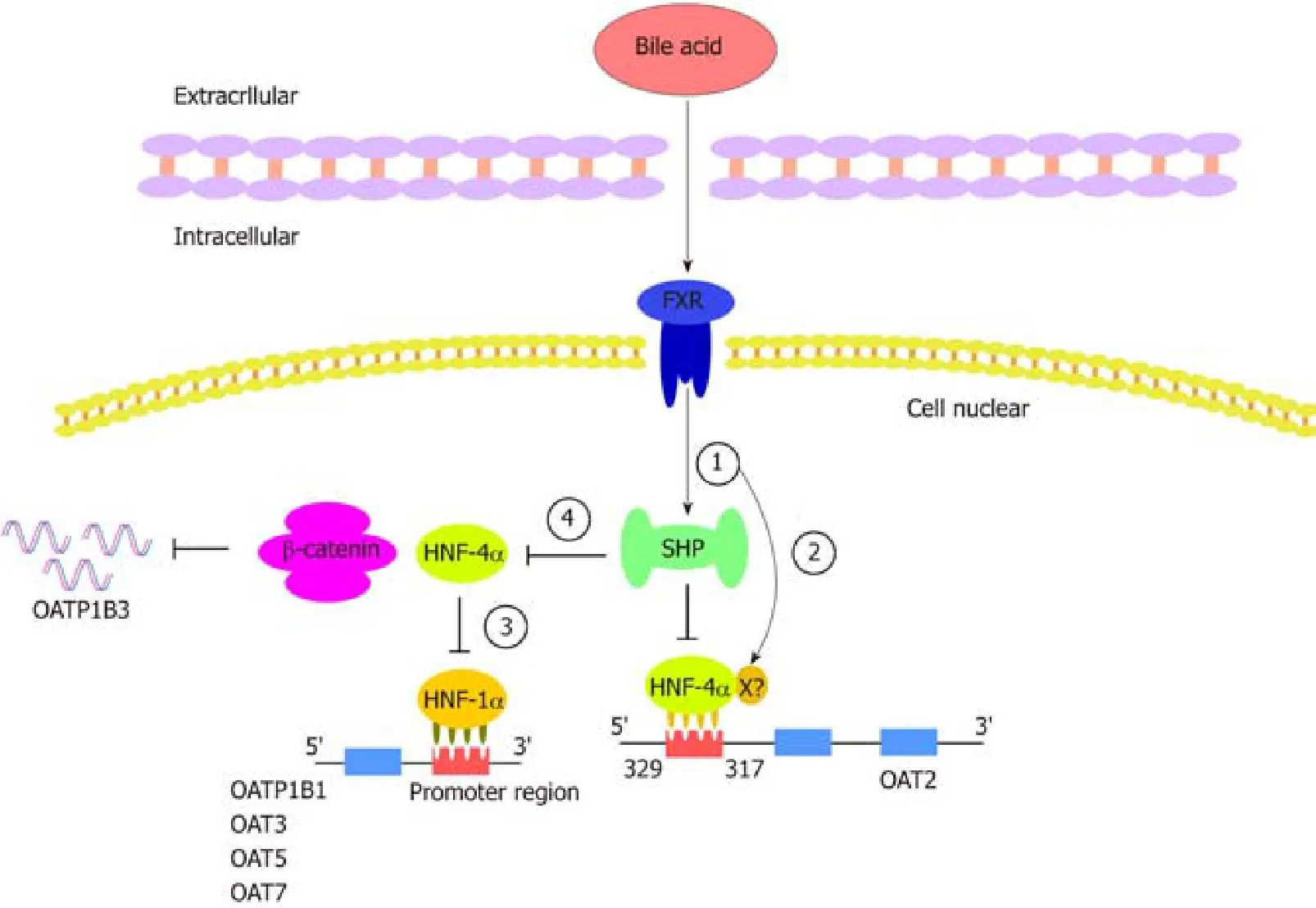
Figure 3 Hepatocyte nuclear factor regulates organic anion transporters and organic anion transporter polypeptides through a mechanism composed of a series of cascade reactions.
The clinical relevance of drug transporters depends on their distribution in human tissues, their vector orientation, and the therapeutic indices and individual differences in the PK and pharmacodynamic properties of the substrate drugs.It has been shown that gene polymorphisms inOATsaffect the PKs of substrate drugs.For example,some single nucleotide polymorphisms of the gene encoding OATP1B1 on sinus membranes are associated with changes in the uptake and excretion of organic anionic compounds.This discovery indicates that these transporters have important clinical significance[136-140].OATs play a very important role in drug absorption,distribution, metabolism, and excretion, and changes in these transporters in the liver and/or kidney may affect the rate of drug metabolism, excretion, and drug residence time and half-life[141].Studies have shown that pravastatin is a highly effective lipidlowering drug that targets the liver, where it inhibits hydroxy methylglutaryl coenzyme A and cholesterol synthesis.Pravastatin is weakly soluble and can be transported into cells by OATP1B1, where it exerts its pharmacological effects before being discharged into the bile by multidrug resistance-associated protein (MRP2) and bile salt export pump on the bile duct-side membrane and then to the duodenum.Then, it is reabsorbed in the intestine where it is integrated into the intestinal-hepatic circulation, improving its bioavailability and pharmacological effects[142,143].In addition, OAT3 is critical to the elimination of liver-derived phase II metabolites,particularly those that undergo glucuronidation.Bushet al[6]analyzed the pathways of OAT3-KO using the robust metabolomics data from mice, which indicated that OAT3 plays a central role in the movement of metabolites through the “gut-liver-kidney”axis, participating in the absorption, metabolism, and excretion of endogenous metabolites, particularly the gut microbial metabolites, bile acids, and nutrients that have undergone modification by phase 2 liver drug metabolizing enzymes involved in sulfation and glucuronidation reactions.A large number of these metabolites may be involved in “metabolite signaling” and signalingviaG protein-coupled receptors throughout the body[6](Figure 2).
Liver cancer is one of the most common causes of cancer death worldwide.Although surgery is a common treatment, the removal of these tumors is not always feasible and it is necessary to use alternative therapies for this disease.Systemic chemotherapy is the most common option for the treatment of advanced disease[50].Unfortunately, pharmacological approaches are very ineffective because of resistance to antitumor drugs and/or development of chemical resistance during treatment,despite the number of drugs available to treat these tumors.The reduced therapeutic efficacy of anticancer drugs may be caused by changes in the expression and/or activity of the transporters involved in drug uptake, which have been identified as mechanisms of chemoresistance 1a (MOC-1a)[144].OATP1B1 is considered an OAT belonging to the MOC-1a group that plays an important role in the uptake of anionic antitumor drugs in the liver, such as irinotecan[145], paclitaxel[146], and cytostatic cisplatin-conjugated bile acid derivatives[147].Due to the abundant expression of OATs in liver cancer and their high activity in transporting many anticancer drugs, they can be considered important therapeutic targets in the design of anticancer drugs.In the liver tissues of patients with nonalcoholic fatty liver, HCC, inflammatory cholestasis,PBC, or chronic hepatitis, the expression of OATP1B is usually reduced[148].Inhibition of OATP1B function may also result in elevated levels of bilirubin and affect liver function.However, the combined use of substrates of OATP1B used as drugs may result in unexpected toxicity and fatal consequences[149,150].These findings suggest that OATPs can be important targets for anticancer therapy in three ways:(1) OATPmediated hormone expression, formation of hormone conjugates, or uptake of growth-promoting chemicals can be prevented with OATP inhibitors; (2) New anticancer drugs can be designed as substrates of OATP to increase their uptake by OATP-expressing cancer cells; and (3) Allosteric stimulators can enhance the uptake of anticancer drugs.Since OATs may determine the extent of distribution of some drugs to target sites and nontarget sites, the transport capacity of liver transporters can be used to enhance the distribution of drugs to target sites and facilitate the intracellular accumulation of various compounds in the liver.OATs might be important with respect to the discovery of novel cancer agents.
CONCLUSION
As our understanding of organic anions increases, the mechanisms of OAT and OATP regulation in the liver will be further elucidated.How to effectively target transporters to improve the distribution of drugs in the liver and reduce the adverse reactions of the delivered drugs are urgent problems that need to be resolved.It has been confirmed that many drugs are substrates of OATs and OATPs, and hepaticspecific expression of these transporters can mediate the uptake of specific substrates.Then, these drugs are discharged into bile and finally enter the intestinal tract,facilitating the targeted therapy with clinical drugs, improving their efficacy, and reducing their adverse reactions.Although the application of transporters in clinical practice is not imminent, these studies may help establish the target therapy of cancer or increase drug bioavailability.It is believed that with further research on these transporters and liver cancer and other liver diseases, targeted therapy with OATs and OATPs is expected to be an ideal and effective new way to treat and improve the survival rate of patients with liver disease.
杂志排行

World Journal of Clinical Cases的其它文章
- Value of early diagnosis of sepsis complicated with acute kidney injury by renal contrast-enhanced ultrasound
- Value of elastography point quantification in improving the diagnostic accuracy of early diabetic kidney disease
- Resection of recurrent third branchial cleft fistulas assisted by flexible pharyngotomy
- Therapeutic efficacy of acupuncture combined with neuromuscular joint facilitation in treatment of hemiplegic shoulder pain
- Comparison of intra-articular injection of parecoxib vs oral administration of celecoxib for the clinical efficacy in the treatment of early knee osteoarthritis
- Celiomesenteric trunk:New classification based on multidetector computed tomography angiographic findings and probable embryological mechanisms