Use of tunnel endoscopy for diagnosis of obscure submucosal esophageal adenocarcinoma:A case report and review of the literature with emphasis on causes of esophageal stenosis
2019-04-20SongLiuNianWangJianYangJiaYaoYangZhaoHongShi
Song Liu,Nian Wang,Jian Yang,Jia-Yao Yang,Zhao-Hong Shi
Abstract
Key words: Esophageal stenosis; Adenocarcinoma of the esophagus; Tunnel endoscopic technique; Case report
INTRODUCTION
Tumors of the esophagus are a severe health problem worldwide with crypticity and high mortality.According to the different pathologic types,tumors of the esophagus have been divided into esophageal squamous cell carcinoma and esophageal adenocarcinoma[1].Esophageal squamous cell carcinoma is the predominant histologic type while esophageal adenocarcinoma remains rare[2].It is generally accepted that pathological examination is the “gold standard” for the diagnosis of esophageal tumors.Moreover,imaging modalities such as endoscopy,endoscopic ultrasonography (EUS),and computed tomography (CT) have been applied to measure the depth of the invasion of the esophageal wall,tumor size,the presence of invasion into adjacent organs,lymph node metastasis,and distant metastasis[3].The high mortality rate has been attributed to the fact that half of patients have a locally-advanced form of the disease at diagnosis[4].Therefore,early pathological diagnosis can effectively improve patient prognosis.
The tunnel endoscopic technique is an innovative and minimally-invasive endoscopic surgical procedure.The first submucosal tunnel endoscopic resection in the world was conducted in China,when it was used to remove submucosal tumors(SMTs) originating from the muscularis propria of the esophagus[5].Nevertheless,biopsy in a submucosal tunnel has not been well studied.We report herein an unusual case involving diagnosis of esophageal stenosis caused by adenocarcinoma through the tunnel endoscopic technique,and review the causes of esophageal stenosis.The patient has signed an informed consent form and data had been anonymized and unidentified.
CASE PRESENTATION
Chief complaints
A 74-year-old male patient visited our hospital complaining of dysphagia which he had experienced for half a year with no clear trigger.
History of present illness
He vomited after eating,bringing up the contents of the stomach.There was no obvious chest pain,hematemesis,or weight loss.He was in good physical condition.
RCS仿真模型如图3所示,图3(a)为空客A320型飞机模型,图3(b)为F-15C型战斗机模型。以目标到接收机的雷达视线方位角为90°、俯仰角为125°为例,4种极化方式的静态RCS数据分别如图4、图5所示,其中,图4为目标是空客A320型飞机的RCS结果,图5为F-15C型战斗机的RCS结果。
Personal and family history
There were no special circumstances in personal and family history.
Physical examination upon admission
On physical examination,he showed no evident positive characteristics.
Laboratory examinations
With regard to laboratory values,only the serum tumor marker CA199 (47.85 U/mL;normal reference range:< 39 U/mL),albumin (35.6 g/L; normal reference range:40-50 g/L),and hemoglobin (124 g/L; normal reference range:130-175 g/L) were moderately changed.Renal function,electrolytes,blood sugar,cholesterol,erythrocyte sedimentation rate,blood coagulation,humoral immune function,antiphospholipid antibody,anti-autoantibody,antineutrophil cytoplasmic antibody,urine,and conventional stool concentration were all within normal limits.
Imaging examinations
Color Doppler ultrasonography revealed chronic cholecystolithiasis.A chest CT scan revealed thickening of the esophageal wall (Figure 1A and B).Barium meal X-ray showed that the lower esophagus presented the beak sign,suggesting achalasia(Figure 1C and D).Regarding condition,no ulceration,prominence lesions,or Barrett's esophagus manifestation was found by endoscopy (Figure 2A-D).In addition,routine gastroscopy was performed at a local hospital,and no tumor cell was detected by pathological examination at esophageal stenosis.EUS was performed to clarify the cause of the narrow esophageal structure.On EUS,esophageal cavity stenosis was visible at a distance of 37 cm from the incisors,along with obvious thickening of the intrinsic muscularis which reached 0.8 cm,and the first to third layer structure was not clear (Figure 2E and F).High-resolution esophageal manometry suggested lower esophageal outflow obstruction (Figure 3).Based on these findings,a tumor that originated from the tunica muscularis esophagi was highly suspected.Therefore,we recommended the patient to undergo a positron emission CT (PET-CT)examination.The PET-CT results from Wuhan Tongji Hospital indicated dilatation of the entire esophagus,stenosis of the esophagus and cardia junction,and increased local metabolism.However,it was difficult to obtain pathological evidence as the esophageal mucosa was only roughened,with no ulceration,erosion,or bleeding.We invited a general thoracic vascular surgeon and a gastrointestinal surgeon to assist in the diagnosis and treatment.Eventually,a multidisciplinary consultation recommended that tunnel endoscopy was performed for biopsy.Therefore,the tunnel endoscopic technique was chose for pathological examination.We created a submucosal tunnel,advanced towards the stenosis of the esophagus,and obtained muscularis tissues (Figure 4).
FINAL DIAGNOSIS
The final diagnosis was adenocarcinoma of the esophagus (Figure 5).
TREATMENT
Regretfully,the patient and family members chose expectant treatment due to the patient’s age and the high costs of surgical treatment.The flow chart of disease diagnosis can be referred to Figure 6.
DISCUSSION
Adenocarcinoma of the esophagus is a malignant tumor arising from the submucosal tissue of the esophagus or from the glands of the cardia.However,because early disease is asymptomatic in most patients,timely diagnosis of esophageal adenocarcinoma (especially arising from the submucosa) is relatively difficult.Even when treated by radical surgery combined with radiotherapy and chemotherapy,the 5-year survival rate remains low[6,7].Thus,early diagnosis and treatment of esophageal tumors are of great significance.
Esophageal strictures can result from a wide variety of benign and malignant conditions.Meanwhile,dysphagia is the most common symptom which urges patients to seek medical treatment.Benign esophageal strictures can occur following peptic strictures[8],eosinophilic esophagitis[9],achalasia[10],pill-injury esophageal strictures[11],caustic strictures[12],anastomotic strictures[13],Crohn's disease-associated esophageal stricture[14],IgG4-related esophagitis[15],radiation-induced esophageal strictures[16],esophageal intramural pseudodiverticulosis[17],or epidermolysis bullosa[18](Table 1).It is generally known that a malignant esophageal stricture refers to esophageal cancer.Some esophageal strictures can be treated by drug therapy such as with proton pump inhibitors or steroids[9,11,15,17],while others can be refractory to most optical endoscopic therapies such as dilation[15,16,18],stent placement[13],or peroral endoscopic myotomy.
In the present case,the mucosa of the esophageal stenosis was only rough,with no obvious ulceration or erosion.It could well be that mucosal biopsies failed to achieve real results.Meanwhile,the stenosis of the esophagus was too narrow for a conventional endoscope to pass,let alone the large probe required for EUS.Therefore,it could not perform EUS guided fine needle aspiration for biopsy and we chose to use small probe endoscopic ultrasonography to clarify the cause of the esophageal stricture.

Figure 1 X-ray and thoracic computed tomography imaging of the patient.
Subcutaneous emphysema,pneumothorax,and secondary infection are common complications of endoscopic resection[19-21].As there was no serous layer of the esophagus,resection of the muscularis propria of the esophagus would be more prone to concurrent subcutaneous emphysema,pneumothorax,and secondary infection than the gastric muscularis propria.When the tunnel endoscopic technique is used to excise SMTs,the lesion mucosal surface remains intact and the mucosa of the tunnel opening is closed with a titanium clip,avoiding leakage of gas and digestive fluid into the chest and abdominal cavity,thus reducing the risk of secondary infection.Moreover,the tunnel endoscopic technique allows clear visualization of bleeding foci in the tunnel,reducing bleeding during the operation and postoperative delayed bleeding.
CONCLUSION
In conclusion,this was an unusual case of esophageal stenosis caused by adenocarcinoma and diagnosed by the tunnel endoscopic technique.As a method of diagnosis and treatment,the tunnel endoscopic technique would be a less complicated and less risky choice.We would like to emphasize the role of tunnel endoscopy in diagnostic treatment.Further,we analyzed the common causes of esophageal stenosis,hoping to provide some information which will help with clinical work.

Table 1 Analysis of causes of esophageal stenosis

Figure 2 Upper gastrointestinal endoscopy and endoscopic ultrasonography of the patient.

Figure 3 High-resolution esophageal manometry.
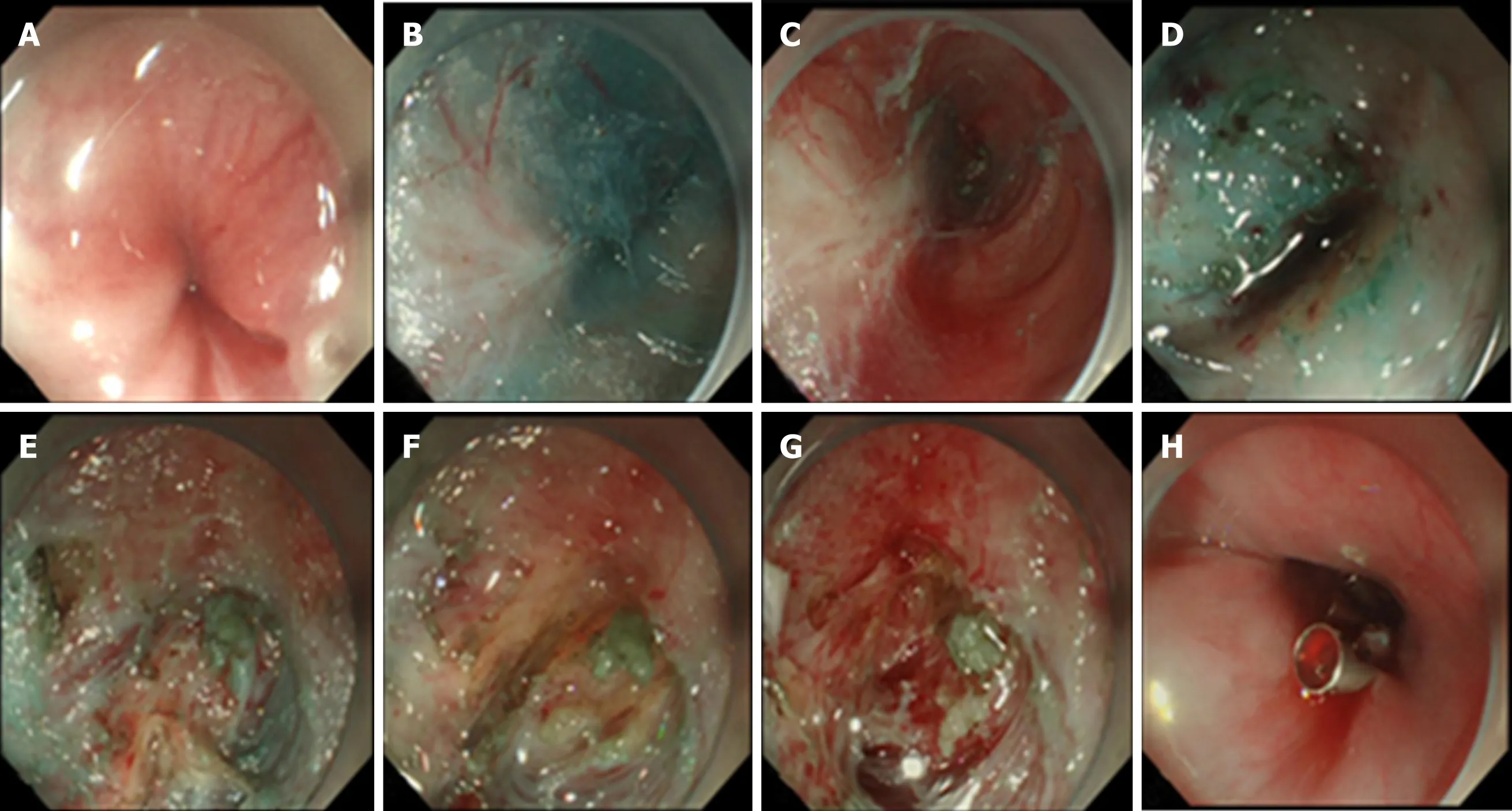
Figure 4 Case illustration of endoscopic biopsy through a tunnel.
猜你喜欢
杂志排行

World Journal of Clinical Cases的其它文章
- Clinical presentation and early predictors for poor outcomes in pediatric myocarditis:A retrospective study
- Safety of an improved patent ductus arteriosus occluder for transcatheter closure of perimembranous ventricular septal defects with abnormally attached tricuspid chordae tendineae
- Adiponectin gene polymorphisms and risk of gestational diabetes mellitus:A meta-analysis
- Maternal serum level of resistin is associated with risk for gestational diabetes mellitus:A meta-analysis
- Docetaxel,cisplatin,and 5-fluorouracil compared with epirubicin,cisplatin,and 5-fluorouracil regimen for advanced gastric cancer:A systematic review and meta-analysis
- Sustained complete response to erlotinib in squamous cell carcinoma of the head and neck:A case report