Prostate resection speed:A key factor for training and broad outcomes?
2019-04-16JackDonatiBourneShahdNourEmiliyaAngovaGeorgeDelves
Jack Donati-Bourne,Shahd Nour,Emiliya Angova,George Delves
Abstract
Key words:Prostate;Resection;Trans-urethral resection of prostate;Training;Speed
INTRODUCTION
Trans-urethral resection of prostate (TURP) is one of the most commonly performed operations in urology to treat bladder outflow obstruction (BOO) in men.
Increasing the operative time of TURP surgery is reported to adversely impact patient factors such as fluid shifts,post-operative bleeding and thrombo-embolic events[1]and indeed experts suggest urologists should limit their TURP resection time to 60 min[2].
The operating urologist’s prostate resection speed (PRS) must therefore balance a speed sufficiently high to create an open cavity within the available indicated operative time,without jeopardizing patient safety and increasing risk of iatrogenic injuries.
There is however no defined PRS which a urologist should aim to operate at[1],furthermore studies have demonstrated that greater degrees of prostatic resection have not resulted in significant variations in long-term improvements in BOO symptoms after surgery[3,4].
TURP surgery is also key for endo-urological training in the British National Health Service (NHS),allowing the junior urologist to improve their cystoscopic skills,gain confidence with endoscopic equipment and familiarize themselves with genitourinary anatomy[5].
United Kingdom trainee urologists are currently required to perform at least 120 TURPs to achieve their Certificate of Completion of Training,and therefore in the NHS TURP is often performed by trainees under consultant supervision[6].Many trainees will recall their consultant during their training urging them to increase their PRS[7],however most surgeons would agree that the perception of the passage of time in theatre differs when observing surgery compared to performing it[8].
This study aimed to evaluate whether there was an objective difference in consultantsvstrainees PRS and whether any such differences in PRS affected complication rates and outcomes after TURP.The study also aimed to use the findings to discuss the true merit of urology trainers evaluating their trainees by their PRS.
MATERIALS AND METHODS
Inclusion criteria
The study was undertaken retrospectively and is descriptive.All Bipolar TURPs performed in a single center of 5 urology consultants and 2 United Kingdom nationally appointed urology trainees between 13/04/2016 and 27/06/2017 were included in the study.The dates of the study were selected to allow for a representative number of TURPs to be performed by each surgeon for analysis.
Both trainees were in their third year of a 5-year higher urological training pathway,had performed fewer than 30 TURP operations independently prior to the start of the study and all their operations within the study were undertaken independently with un-scrubbed consultant supervision.The trainees had not received any simulated training prior to the study.
Exclusions
Patients undergoing concomitant operations at the time of TURP (e.g.,circumcision or cystolitholapaxy) or where unexpected intra-operative equipment problems occurred were excluded.
2.11 缩略语文中尽量少用。必须使用时应于首次出现处先叙述其全称,然后括号注出中文缩略语或英文全称及其缩略语,后两者间用“,”分开(如该缩略语已共知,可不注出其英文全称)。缩略语不得移行。
Data collected
Mass of resected prostate tissue in grams,operative time in minutes,occurrence of post-operative complications and outcomes at 3-mo after surgery were obtained from electronic records.
Defined outcomes
Clavien-Dindo Grade II complications or above only were considered significant for the study and therefore included in the analysis.
Patients that were defined as suffering post-operative bleeding complication included any who needed:continuous bladder irrigation and manual washout for 3 d or more post-TURP,and/or;a blood transfusion,and/or;return to theatre for formal bladder washout
Post-operative sepsis events were recorded as those diagnosed and treated by the attending doctor,with or without the subsequent confirmation of a positive blood culture.
A binary rather than qualitative outcome patient evaluation tool was used to record successful versus unsuccessful outcomes at 3-mo after TURP surgery.
For those already catheterized prior to TURP a binary successful outcome was deemed as achieving catheter-free status at 3 mo after surgery.
For non-catheterized patients,binary successful outcome was a subjective patientreported moderate or significant improvement in Lower Urinary Tract Symptoms(LUTS) on direct enquiry at the 3 mo follow up clinic appointment with the operating consultant.Mild or no improvement in patient-reported LUTS at 3 mo after TURP was deemed unsuccessful outcome.
RESULTS
Overview of results
One hundred and fifty seven patients underwent Bipolar TURP surgery during the timeframe of the study.All cases were done electively in the same operating theatre of the hospital.
The following patients were excluded from analysis:(1) 23 had concomitant operations (14 cystolitholapaxy,3 urethral dilatation,2 optical urethrotomy,2 circumcision,2 bladder biopsy);(2) 5 inadequate electronic records/results for analysis;and (3) 3 intra-operative equipment problems that prolonged operative time,
Consultant B had supervised Trainee 1 and 2 undertaking TURPs but personally performed only 1 TURP during the study timeframe and therefore their patient were not included in analysis.
All cases performed by trainees were performed under consultant supervision,scrubbed or unscrubbed in theatre.125 patients were included for analysis.The breakdown of operations performed is illustrated in Figure 1.
Results for individual operating surgeons including caseload,PRS,Clavien-Dindo Grade II or above complication rate and binary successful outcome rates are illustrated in Table 1.
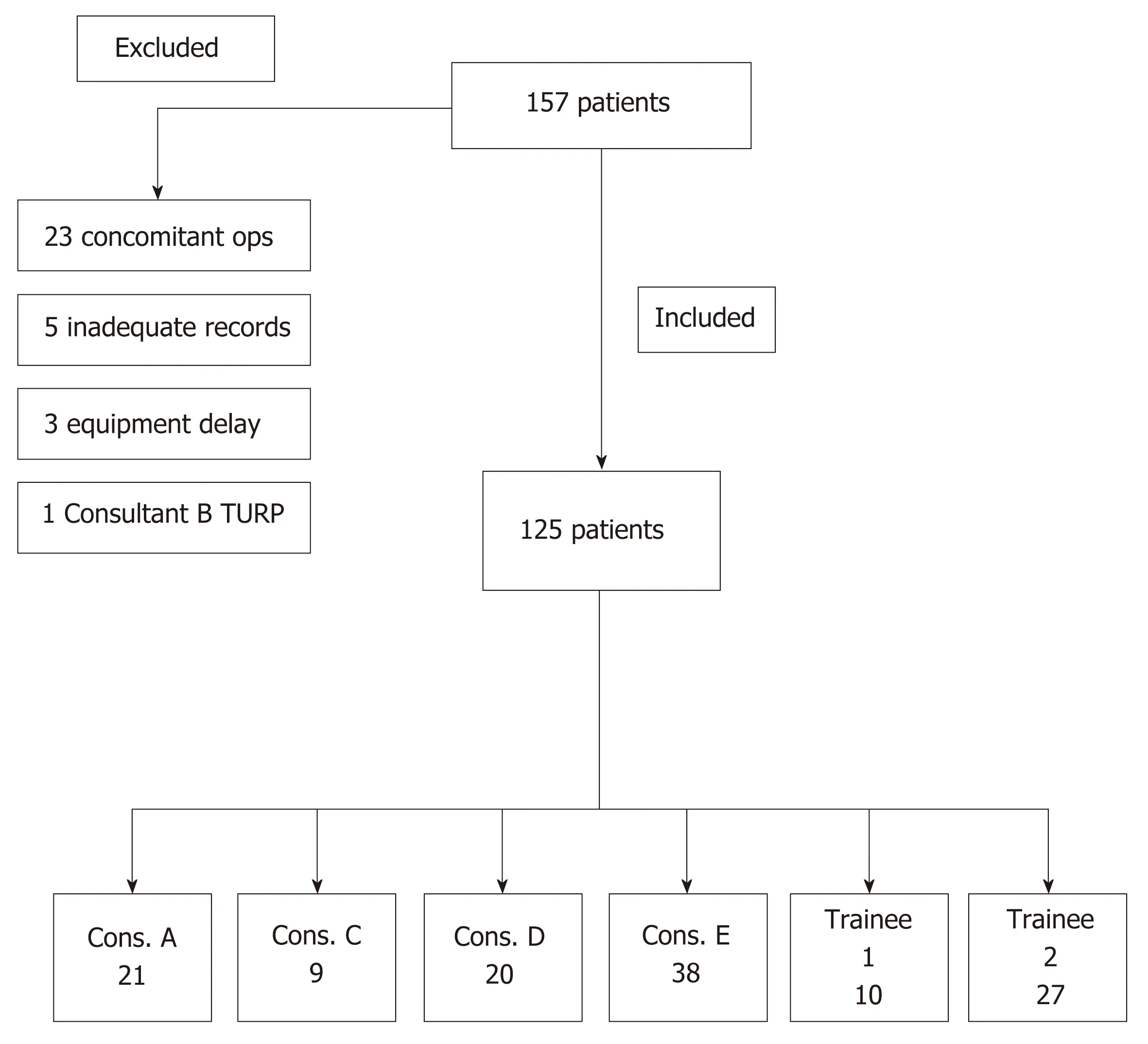
Figure1 Patient inclusion pathway.TURP:Trans-urethral resection of prostate.
The mean PRS of trainees was 0.34 g/min (range 0.31 to 0.36) and this was lower than the mean PRS of 0.41 g/min (range 0.23 to 0.59) for consultants.
Binary successful outcomes
Mean rates of binary outcome as successful were comparable for trainees at 86.5%(range 80–93) and consultants at 90.5% (range 82–100).
Complications
Details of Clavien-Dindo II or above complications are listed in Table 2.No relationship was observed between increasing PRS and rate of significant postoperative complications.The trainees’ patients did not suffer any significant complications as defined by the study.No fatalities were recorded during the study.Two patients had to be taken back to theatre for a formal bladder washout under general anaesthesia,six suffered post-operative sepsis,one received a blood transfusion and three required prolonged ward-based bladder irrigation and washouts.
Observed relationships
No relationship was observed between PRS and rate of binary successful outcome at 3 mo.PRS was not observed to be related to number of TURPs performed.PRS increased with increasing experience for Trainees 1 and 2 when comparing the first half of their TURPs (mean 0.28 g/min,range 0.26-0.29) to their latter half (mean 0.41,range 0.33–0.48) (Table 3).
For Trainee 1 the mean PRS in the first half of cases was 0.29 g/min and this increased to 0.33 g/min in their latter half,whilst for Trainee 2 the mean PRS was 0.26 g/min in their first half increasing to 0.48 g/min in their latter half.
DISCUSSION
The study is descriptive and the authors discuss the findings of the first 14 mo of the study accordingly.In the study’s hospital the urology Consultants had higher mean PRS than Trainees during TURP and therefore most probably correctly identified the PRS of their trainee was slower than theirs.The consultants mean PRS of 0.41 g/minis however lower than PRS figures approximating 0.6g/minute quoted in other TURP series[9,10].
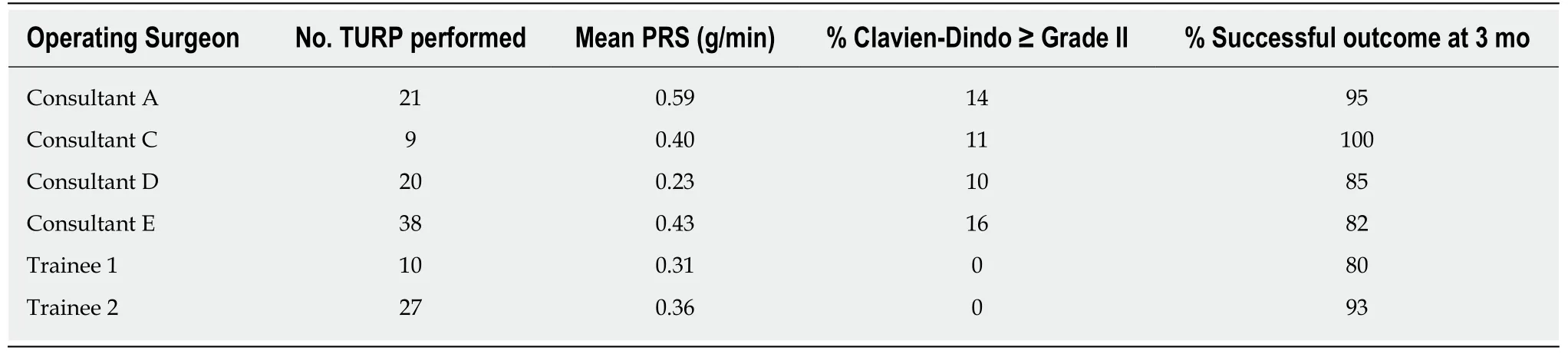
Table1 Surgeon caseload,prostate resection speed and complication rate and binary successful outcome
Urology trainees will encounter a learning curve during their TURP training.A retrospective review of more than 4000 TURPs performed by a single surgeon over 25 years concluded only 81 operations were needed before the surgeon's skill reaches a plateau in TURP[11].The United Kingdom requirement of 120 TURPs for Completion Certificate of Training in urology hence appears sufficient number to be deemed competent at performing TURP independently.
The key factor that increases a urologist’s PRS is increasing experience[11,12]as confidence handling cystoscopic equipment,achieving haemostasis and familiarity with anatomy improve.The trainees demonstrated an increase in PRS when comparing the first and latter halves of their cases,hence trainers need not focus primarily on speed as they can expect a natural acquisition of PRS in their trainees that will be achieved as their experience increases.
Furthermore the traditional notion of TURP surgery being a highly time sensitive operation,whereby sufficient prostate must be resected whilst minimizing the timeassociated risk of TUR syndrome,has been challenged with bipolar TURP[2].Simultaneous tissue coagulation during bipolar resection improves visualization thus increasing time proportionally spent resecting,and the substitution of glycine with normal saline as irrigation fluid reduces risk of TUR syndrome[13].The authors accept that the findings of the study may differ with the use of monopolar TURP.
Other factors that may impact PRS by affecting bleeding include whether or not the patient is pre-operatively on finasteride,the presence of a catheter prior to surgery and intra-operative hypertension[14].These factors were not controlled in our study and were not assessed as the authors deemed these to be beyond the scope of the study.The consultants however did not allocate cases to trainees based on these factors and no pre-operative case selection was undertaken.
The study’s binary successful outcome tool arguably does not facilitate an in-depth qualitative outcome analysis and therefore is considered a study limitation.Achieving catheter-free status after TURP however is one of the main preoccupations in patients with a catheter prior to surgery,and hence the authors believe that success in catheter removal is a highly relevant outcome.Likewise achieving a subjectively reported moderate or significant improvement in LUTS at 3-mo after surgery can be considered a valid tool for broadly deeming whether TURP was successful or not.
As such mean binary successful outcome rates were comparable for consultants(90.5%) and trainees (86.5%) and no relationship between PRS and successful outcome at 3-mo was demonstrable.For example Consultant C and E had the two closest PRS values (0.40 g/minvs0.43 g/min) yet one of the greatest differences in successful outcome rates (100%vs82%).
To the authors’ knowledge no study in the literature directly compares PRS with symptomatic outcome after TURP,however the relationship between mass of prostate resected and post-operative LUTS improvement is weak.In a prospective trial by Hakenberget al[4]the Qmax,IPSS and residual urine of 138 patients were documented prior to TURP and re-evaluated 3 and 6 mo after surgery,and the resected tissue weight (RTW) was recorded for each.No statistically significant relationship was found between RTW and IPSS change.Trainers therefore should not primarily focus on trainee’s PRS during TURP training based on symptomatic outcome alone.
Clavien-Dindo Grade I complications were not considered and present another study limitation.
PRS however had no observable relationship with rates of Clavien-Dindo Grade II complications or above after TURP.For example Consultants C and D had closest complication rates (11%vs10%) but significantly different PRS (0.40 g/minvs0.23g/min).
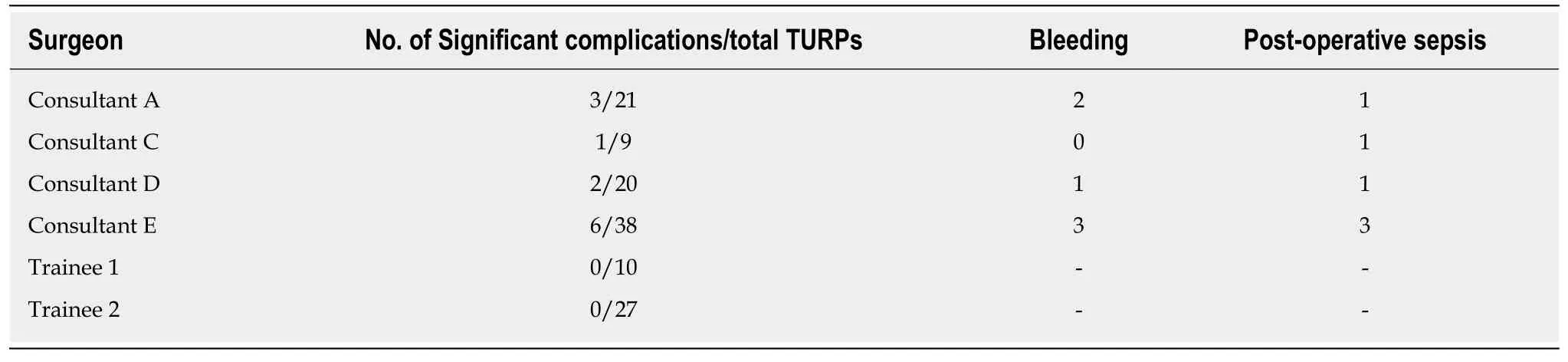
Table2 Breakdown of Clavien Dindo grade 2 post-trans-urethral Resection of Prostate complications per surgeon
The patients operated on by trainees did not experience Clavien-Dindo Grade II or above complications,however this may be due to pre-operative case selection –higher-risk patients more likely to suffer complications were preemptively operated on by consultants.
No trend was observed between operative time and complication rates – these occurred in cases with mean operative time of 47.5 min (range 34-67),compared to mean operating time for all cases of 47.1 minutes (range 5-116).
The mean PRS for cases suffering complications (0.49 g/min) was greater than mean PRS for all cases (0.39 g/min).This suggests a slower PRS is less likely to yield complications in bipolar TURP,however it is also possible that the urologist who deemed a patient as medically high-risk chose to resect faster in an attempt to minimize operative time.The findings therefore do not suggest trainers should urge their urological trainees to increase their PRS based on rates of post-operative complications alone.
The limitations of the study include its descriptive nature and lack of in-depth qualitative analysis in patient outcomes,the exclusion of Clavien-Dindo I complications and the comparably small numbers of operations performed by Consultants B and C and Trainee 1.
The authors propose further studies compare PRS objectively with changes in IPSS before and after TURP,as well as with other post-operative factors such as length of in-patient stay and incidence of Clavien-Dindo Grade I complications.
In conclusion,the authors propose based on this descriptive study that trainers in urology teaching how to perform TURP surgery should focus primarily on adequate patient selection,sound surgical techniques and optimizing post-operative care,rather than the PRS of their up-and-coming budding urologists.

Table3 Mean prostate resection speed for trainees for first half vs second half of trans-urethral resection of prostates performed
ARTICLE HIGHLIGHTS
Research background
Trans-urethral resection of prostate (TURP) is one of the most commonly performed operations in urology to treat bladder outflow obstruction (BOO) in men as well as a key endo-urological training tool in the British National Health Service (NHS) for training junior urologists.The working hypothesis is that prostate resection speed (PRS) in the context of bipolar TURP surgery,is not a key factor in major complication rates or broad patient outcomes at 3 mo after surgery,and therefore supervising consultants should not focus primarily on resection speed when teaching TURP.
Research motivation
The study was motivated to identify whether resection speed during TURP training should be a key factor.
Research objectives
The main objective was to identify whether TURP resection speed affected significant complication and broad outcomes at 3 mo.The study found that resection speed did not correlate with significant complication and broad outcomes at 3 mo.The authors propose that PRS should not be a key factor during TURP training.
Research methods
Participants included:all Bipolar TURPs undertaken between 13/04/2016 and 27/06/2017.Exclusions:patients undergoing concomitant operations or where intra-operative equipment problems occurred.Patients identifiedviaoperative logbooks and case notes retrieved electronically.
Research results
The study found that PRS did not correlate with significant complication and broad outcomes at 3 mo.The authors propose a similar study with increased power and qualitative assessment of symptomatic improvement in relation to PRS.
Research conclusions
PRS did not correlate with significant complication and broad outcomes at 3 mo.The authors conclude that PRS should not be a key factor during TURP training as increasing experience will lead to natural acquisition of speed.PRS is not a cardinal factor in bipolar TURP surgery for significant complication rates or broad outcomes 3 mo after surgery.In the era of monopolar TURP resection,PRS was highly relevant due to risks of TURP syndrome.In bipolar surgery the use of saline as irrigation fluid minimises this risk.Therefore the authors propose a paradigm shift in training whereby less focus is placed on PRS and greater emphasis on sound safe surgical technique.
Research perspectives
The authors propose a paradigm shift in training whereby less focus is placed on PRS and greater emphasis on sound safe surgical technique.The authors propose a similar study with increased power and qualitative assessment of post-operative symptomatic improvement in relation to PRS.Prospective high-powered study with IPSS evaluation pre- and post-TURP and correlation with PRS.
ACKNOWLEDGEMENTS
The authors wish to thank Mr Waliul Islam,Mr Shashank Kulkarni,Mr Sikander Khwaja,Mr Anthony Noah and Miss Jyoti Shah.