Application of self-care based on full-course individualized health education in patients with chronic heart failure and its influencing factors
2019-03-14JingSunZhiWeiZhangYueXianMaWeiLiuChunYingWang
Jing Sun, Zhi-Wei Zhang, Yue-Xian Ma, Wei Liu, Chun-Ying Wang
Abstract
Key words: Full-course individualized health education; Chronic heart failure; Self-care;Influencing factors
INTRODUCTION
Chronic heart failure (CHF) is the end stage of most cardiovascular diseases.As one of the serious public health concerns worldwide, it drastically undermines the quality of life of patients due to its high prevalence, high mortality, and high readmission rate[1].Studies have shown that appropriate self-care behavior among CHF patients helps to maintain physical stability and improve their ability to manage diseases[2].However,the self-care behavior among CHF patients is far from satisfactory, as reflected in low medication compliance, poor knowledge of symptom management, and lack of awareness in diseases.The full-course disease management model refers to a model that efficiently integrates the existing limited resources for disease management[3].Up to now the full-course management model has been applied in the management of patients with chronic disease and/or mental disorders, with good effectiveness.In the present study, based on the full-course disease management model and the individual features of patients, we applied full-course individualized health education (FCIHE)in CHF patients, providing patients with scientific, professional, and tailored health guidance and helping them learn and adopt the concept of self-care behavior, in an attempt to provide new guidance for the development of self-care programs for CHF patients.
MATERIALS AND METHODS
General data
This study is a randomized controlled trial.The CHF patients who were admitted to our center between September 2015 and June 2016 were selected by convenience sampling.Inclusion criteria were:(1) Meeting the diagnostic criteria of CHF released by the American Heart Association[4]; (2) New York Heart Association (NYHA) class II or above; and (3) Being conscious and able to communicate with researchers and participating in the study voluntarily.The exclusion criteria included:(1) Cognition or learning problems; (2) Could not take care of themselves; (3) Serious comorbidities or complications; and (4) Had participated in other self-care-related research.A total of 100 eligible patients with CHF were enrolled according to the inclusion/exclusion criteria, and all of them signed the informed consent forms.These patients were equally divided into the intervention group and control group (50 patients each)using a random number table.The baseline data including cardiac function (evaluated with NYHA classification), hospital stay, and age were matched between these two groups (P> 0.05) (Table 1).
Interventional method
Patients in the control group received routine nursing care including routine nursing during hospitalization, guidance at discharge (including the delivery of a health education manual), and telephone follow-up.The telephone follow-up was performed by a cardiology nurse 2 wk after discharge, and the follow-up content included recent health conditions (e.g., asthma and edema) and routine health guidance (exercise,drug use, and diets).Patients in the intervention group received FCIHE, as described below.
Setting up a research team
The self-care multidisciplinary research team for CHF patients was established,consisting of two cardiology nurses, two cardiologists, one clinical pharmacist, one rehabilitation therapist, and one nutritionist.Among them, two cardiology nurses had long been engaged in cardiac nursing and had been independently responsible for patient management in the cardiology ward, with extensive experience in the nursing and health education of CHF patients.In this study, they were responsible for selfcare guidance throughout the study.Two cardiologists had extensive clinical experience and were responsible for assisting patient management.The clinical pharmacist, rehabilitation therapist, and nutritionist provided professional guidance during the development of the FCIHE plan for each patient.Led by the cardiology nurses, the whole team jointly established disease/health management plans for patients during hospital stay and after discharge, with an attempt to improve patients’ self-care abilities and ultimately improve their quality of life.
Content of the intervention
During hospital stay:On the day of admission, the patient’s disease condition,awareness of disease, family status, education background, and learning ability were evaluated to establish a health record.According to the evaluation results, the research team formulated an in-hospital health education plan for each patient to define the daily health education content; mainly covering the primary disease-related knowledge, disease pathogenesis mechanism, treatment plan and goals, medication guidance, exercise, nutrition guidance, and prevention of acute attack.A clear-cut intervention program was listed in an EXCEL form, allowing the patients to participate in the self-care process while receiving nursing and initially adopt a concept of self-care behavior.After being aware of their disease and its treatment, the patients were expected to understand the importance of self-care and increase their self-care ability and confidence through scientific and professional health guidance.With the guidance of the team members, the patients developed a self-care plan and implemented it.The nursing staff spent 3 d to help patients correct their self-care plan and monitored its implementation.Then, the patient was required to complete selfcare independently, and their daily medication, diet, and exercise plans were modularized and digitized in the form of a daily schedule, which was inspected by the nursing staff the next day in hospital or by family members after discharge.
Continued intervention after discharge:The cardiology nurses managed the whole process.Through the internet-based medical platform, the cardiology nurses answered questions online from 09:00-17:00 h daily.The caregivers assisted in comanaging patients and supervising the patients to perform self-care in a reasonable way.Hospital nursing staff prepared a weekly health education program, with a new theme every week, covering information on medication, exercise, and nutrition.Themessages were delivered to patients through an APP platform or WeChat public account.However, a detailed self-care plan was still developed and implemented by patients themselves.The nursing staff performed weekly telephone follow-up within 3 mo after discharge, and then once every 2 wk after 3-4 mo, and once every month after 5–6 mo, so as to learn the current health status of the patients and provide corresponding health guidance and self-care correction.The research team members met every 2 mo, and patients or their families were encouraged to participate in the meetings; during which the difficulties encountered in the latest interventions were shared and countermeasures proposed.The meeting results and consensus were published online to inform patients who did not participate.
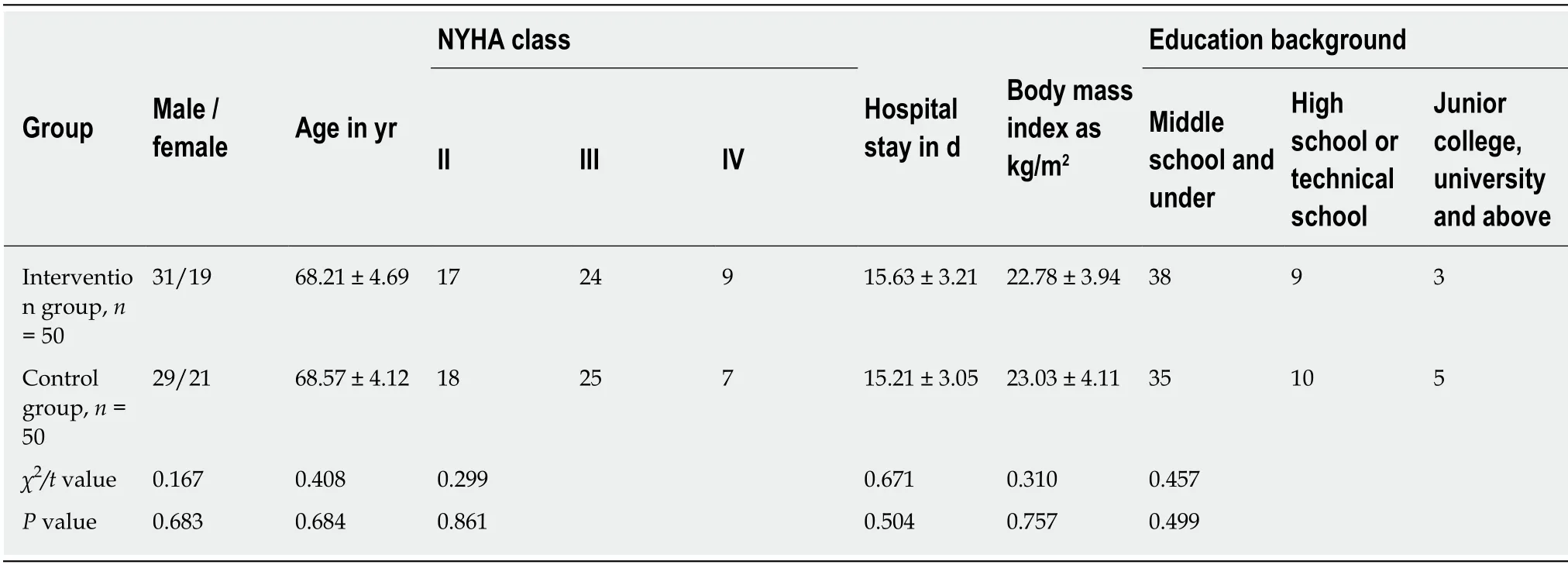
Table 1 Comparison of baseline data between the two groups
Upgraded patient self-care:After a patient had performed self-care for 3 mo, the nursing staff contacted the patient by telephone or WeChat, inquiring and recording the patient’s latest care and recent schedule.The patients were informed that the CHF Patient Club meetings were arranged at the end of the 4th, 5th, and 6thmo after discharge.Five to 10 patients were invited as guests to participate in each meeting, so as to fully mobilize the enthusiasm of patients in self-care.In addition, their experience in self-care and disease control encouraged more new patients to implement self-care.
Evaluation indicators
Baseline data were collected at admission, and these data were reviewed at the 3rd and 6th mo after discharge, so as to fully learn the physical condition of the patients after the intervention.Meanwhile, disease consultation was provided by cardiologists.All data were collected and verified on site by two investigators, so as to ensure the accuracy and completeness of the information.
Six-minute walking distance:Six-minute walking distance (6MWD) is an important indicator for evaluating cardiac function.A four-stage evaluation method can be used.However, since cardiac function gradually worsens with the progression of HF, it is difficult to observe directly the improvement in cardiac function using this staging method.Therefore, the walking distance was directly used for the evaluation in this study.
Self-care of heart failure index[5]:Self-care of heart failure index is composed of 22 items divided into three subscales:Self-care maintenance (10 items), self-care management (six items), and self-care confidence (six items).Among them, the selfcare maintenance applies the Likert scale (rated as 1 = never or rarely; 2 = sometimes;3 = usually; and 4 = daily or always).The self-care management is mainly used to measure the patient’s ability in symptom recognition and implementation and evaluation of treatment.Symptom recognition has one item, evaluated with a 0–4 scale, reflecting the speed of a patient identifying their symptoms.Treatment implementation has four items, evaluated with a Likert 1–4 scale (rated as 1 = not likely; 2 = somewhat likely; 3 = likely; and 4 = very likely).Evaluation of treatment has one item, evaluated with a Likert 0–5 scale (0 = I did not try anything; 1 = not sure; 2 = somewhat sure; 3 = sure; and 4 = very sure).Self-care confidence contains six items, evaluated with a Likert 1–4 scale (1 = not confident; 2 = somewhat confident; 3= very confident; and 4 = extremely confident).The following format was used to calculate the standard scores of all three subscales:[(actual score – minimum possible score)/(maximum possible score – minimum score)] × 100%.A threshold value of 70 was used to evaluate whether the patients’ self-care behavior met the criteria.Cronbach’s α coefficients for these three subscales were 0.656, 0.736, and 0.869,respectively, and the overall Cronbach’s α coefficient of the scale was 0.853[6].
36-item short form health survey:The 36-item short form health survey (SF-36)questionnaire revised by the Medical College of Zhejiang University was used in the survey.It contained eight subscales, including physical functioning, role limitations due to physical problems, bodily pain, general health perceptions, vitality, social functioning, role-limitations due to emotional problems, and mental health.Scores range from 0 to 100.The higher the score, the better the quality of life of patients.The split-half reliability of the SF-36 was 0.920, and the Cronbach’s α was 0.880.
Analysis of the influencing factors of patient self-care:With patient self-care as a dependent variable and age, cardiac function class, and education background as independent variables, multivariate logistic regression analysis was performed to evaluate the influencing factors of patient self-care.
Statistical analysis
The data were double-checked by two researchers and before inputting into the SPSS 22.0 software (Armonk, NY, United States) for statistical analysis.The numerical data are presented as (n, %) and compared byχ2test, and the measurement data are represented as (mean ± standard deviation) and compared withttest at a test level α= 0.05.P< 0.05 was regarded as statistically significant.The analysis of influencing factors was based on multivariate logistic regression analysis.
RESULTS
6MWD at different time points
6MWD was not significantly different between the two groups at admission (P>0.05).Three and 6 mo after discharge, however, 6MWD was significantly increased,and it was significantly longer in the intervention than control group (P< 0.05) (Table 2).
Self-care behavior scores at different time points
The scores for self-care behavior showed no significant difference at admission between these two groups (P> 0.05).However, at 3 and 6 mo after discharge, the total scores of self-care maintenance, management, confidence, and behavior of the intervention group were significantly higher than those of the control group (P< 0.05)(Table 3).
SF-36 scores at different time points
There were no significant differences in the SF-36 scores at admission (P> 0.05).However, at 3 and 6 mo after discharge, the scores of all eight subscales, including physical functioning, role limitations due to physical problems, bodily pain, general health perceptions, vitality, social functioning, role-limitations due to emotional problems, and mental health were significantly higher in the intervention than control group (P< 0.05) (Table 4).
Influencing factors of patient self-care
As shown by logistic regression analysis, the influencing factors of self-care mainly included age, cardiac function class, and education background [odds ratio >1; allP<0.05] (Table 5).
DISCUSSION
Connotation and advantages of FCIHE
FCIHE at the nursing level is designed to offer dynamic monitoring of the disease condition and the healthcare needs of patients and then provide tailored health guidance according to their actual situation.In our current study, individualized selfcare education covering medication, exercise, and nutrition was provided during hospital stay according to the patients’ treatment protocol, disease awareness, and management status.After the patients were discharged, continued guidance on disease/health management was offered by cardiology nurses, so as to help thepatients learn their disease conditions, establish a self-care concept, and better carry out self-management of CHF.

Table 2 Comparison of 6-min walking distance between the two groups at different time points
Along with the improved living standards and changed lifestyles in China, the prevalence of CHF has declined but remains high, which brings a heavy burden to patients, their families, and society.Due to impaired heart function, the patients have decreased exercise endurance and are more susceptible to symptoms such as fatigue,palpitation, and dyspnea, which seriously affect the patients’ activities.The daily activities of patients with severely impaired heart function are restrained, markedly undermining their quality of life[7].With the application of FCIHE in our study, a multidisciplinary research team with members including cardiologists and cardiology nurses, clinical pharmacists, nutritionists, and rehabilitation therapists was established, and a comprehensive and scientific health education program was developed.In addition, comprehensive evaluation was immediately performed at admission, along with in-hospital intervention and continuous intervention after discharge.The individualization and continuity of health education was guaranteed,which, to a certain extent, ensured the seamless transition from hospital to family.
FCIHE helps to improve cardiac function in CHF patients
In the present study, 6MWD at admission was not significantly different between the two groups (P> 0.05); however, at 3 and 6 mo after discharge, 6MWD was significantly longer than at admission, and it was significantly longer in the intervention than control group, suggesting FCIHE improved NYHA class.6MWD is mainly used to evaluate cardiac function in patients with moderate to severe cardiopulmonary diseases.It is not only a key observation indicator in clinical trials but also an important predictor of survival rate.It can adequately reflect the actual status of cardiac function.In our current study, FCIHE offered full-time dynamic individualized health guidance, which increased the patients’ knowledge and awareness of their disease and improved self-care behavior; as a result, their NYHA class was improved.Many other studies[8-14]have also demonstrated that good selfmanagement can improve cardiac function and quality of life.
FCIHE helps to improve self-care behavior
In this study, the scores of self-care behavior at admission showed no significant difference between these two groups (P> 0.05).Three and 6 mo after discharge,however, the scores of self-care maintenance, management, confidence, and behavior in the intervention group were significantly higher than those in the control group (allP< 0.05).This suggested that patients’ self-care behavior score increased over time,and FCIHE improved self-care behavior by providing guidance on self-care.Tavazziet al[15]had similar findings[15-17].Analysis of the changes in self-care maintenance,management, and confidence and behavior scores is more conducive to overall evaluation of patients’ self-care behavior, and change in self-care behavior is closely associated with the content of FCIHE.Gielenet al[18]reported that most of the traditional self-care guidance for CHF patients focuses on health education at discharge, with uniform and non-tailored content, which is solely delivered by medical staff and passively received by patients.Thus, the effectiveness of health education is limited[18-20].During FCIHE, comprehensive evaluation is performed at admission, followed by the creation of a health archive.A personalized health education program during hospitalization was formulated according to the patients’treatment plan and self-care status, with an attempt to enable the patients to be aware of their disease condition and self-care status, understand the importance of self-care,and establish a concept of self-care[21-23].After discharge, the cardiology nurses provided continuous guidance through internet medical platforms and telephone follow-up; during which the importance of self-care was reiterated and scientific and reasonable guidance was provided.In addition, patients were urged to take self-care measures through telephone follow-up[24].The main caregivers were included in the collaborative patient management, which was more comprehensive and efficient and improved the patients’ self-care behavior and ability and confidence in diseasemanagement.
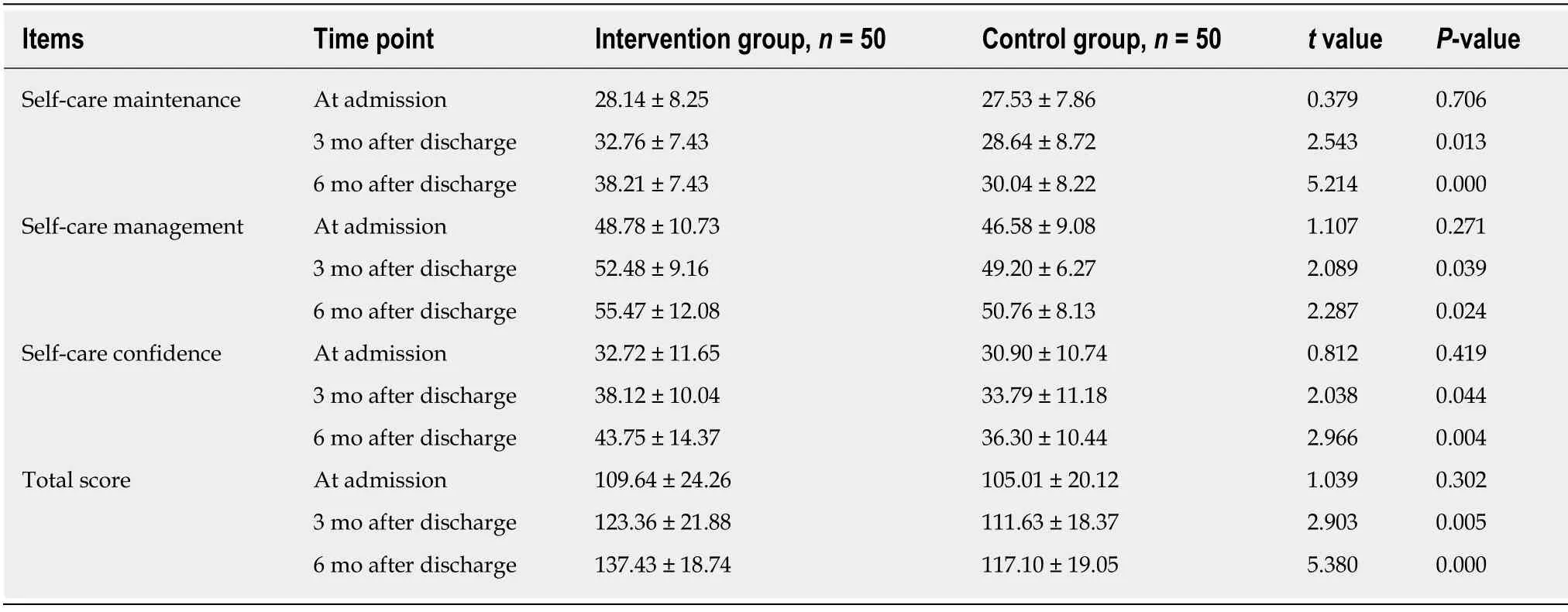
Table 3 Comparison of self-care behavior scores between the two groups at different time points
FCIHE helps to improve quality of life
As shown in our study, there was no significant difference in the SF-36 score between these two groups at admission (P> 0.05).Three and 6 mo after discharge, the quality of life score was also significantly higher in the intervention than in the control group.The SF-36 scores accurately reflect the quality of life from eight subscales including physical functioning, role limitations due to physical problems, bodily pain, general health perceptions, vitality, social functioning, role-limitations due to emotional problems, and mental health.As shown by the SF-36 scores, FCIHE significantly improved the quality of life of our patients, which might be explained by the fact that patients in the intervention group gradually changed from passive nursing to active self-care after implementation of FCIHE, which accurately covered the patients’ daily drug use, diet, and exercise behavior and played an active role in regulating body status and controlling disease conditions[25-27].In addition, Seganet al[28]reported that FCIHE established a progressive closed-loop nursing mode of self-care – guided care– self-care, which helped patients to optimize continuously their care measures during self-care and thus markedly improved their quality of life[28,29].
Influencing factors of self-care
Age, cardiac function, and education level affected the implementation of self-care among our patients, directly or indirectly.Although it has been reported that age is not a useful factor for predicting self-care behavior, our current study found that age was an influential factor[30,31].In fact, old patients with CHF usually have a longer disease course, and HF itself has certain specific symptoms.These patients often experience repeated and painful dyspnea and edema at night, which reminds patients to follow strictly medication instructions and control their diet properly, which helps to optimize their self-care behavior.A higher NYHA functional class is associated with more severe disease, which leads to more stringent restrictions on physical activities[32,33].Slightly increased activity may cause dyspnea and fatigue, which also limits the patients’ normal self-care behavior.CHF patients with higher education level typically have higher income and are more able to follow the dietary plan and take drugs on time[34,35].Self-care is a long process and patients often need time to learn it, and patients with higher education level are more likely to receive information on scientific diet and exercise, as well as related treatment plans, and they can understand the importance of treatment adherence.As a result, patients with high education background can benefit more from self-care.
In conclusion, CHF is the end stage of most heart diseases, with poor prognosis and high mortality.Scientific and rational treatment and self-care are the key factors to improve quality of life and prognosis.Currently, self-care among CHF patients is far from satisfactory.Poor knowledge of symptom recognition and treatment and lack of confidence in treatment have restricted the implementation of self-care.FCIHE offers professional, scientific, and multifaceted self-care guidance through tailored health education during hospitalization and continuous follow-up after discharge, which is conducive with optimizing patient self-care behavior, increasing their confidence in disease treatment, and improving quality of life.FCIHE has the following advantages.(1) The full-course dynamic management helps the medical staff to learn the patient’smedical condition and self-care needs in a more comprehensive and real-time manner.According to the real situation of the patients, the health guidance programs can be adjusted timeously; (2) the full-course participation of medical staff in the health education of patients helps to establish a good doctor–patient relationship and thus increase adherence to treatment and care protocols; and (3) participation of multidisciplinary teams can facilitate healthcare professional development and increase their ability to serve patients.However, our study had some limitations.All the cases selected were from the same hospital, and the intervention duration was short (only 6 mo after discharge).Therefore, the effectiveness of the intervention needs to be verified further in multicenter, long-term studies.
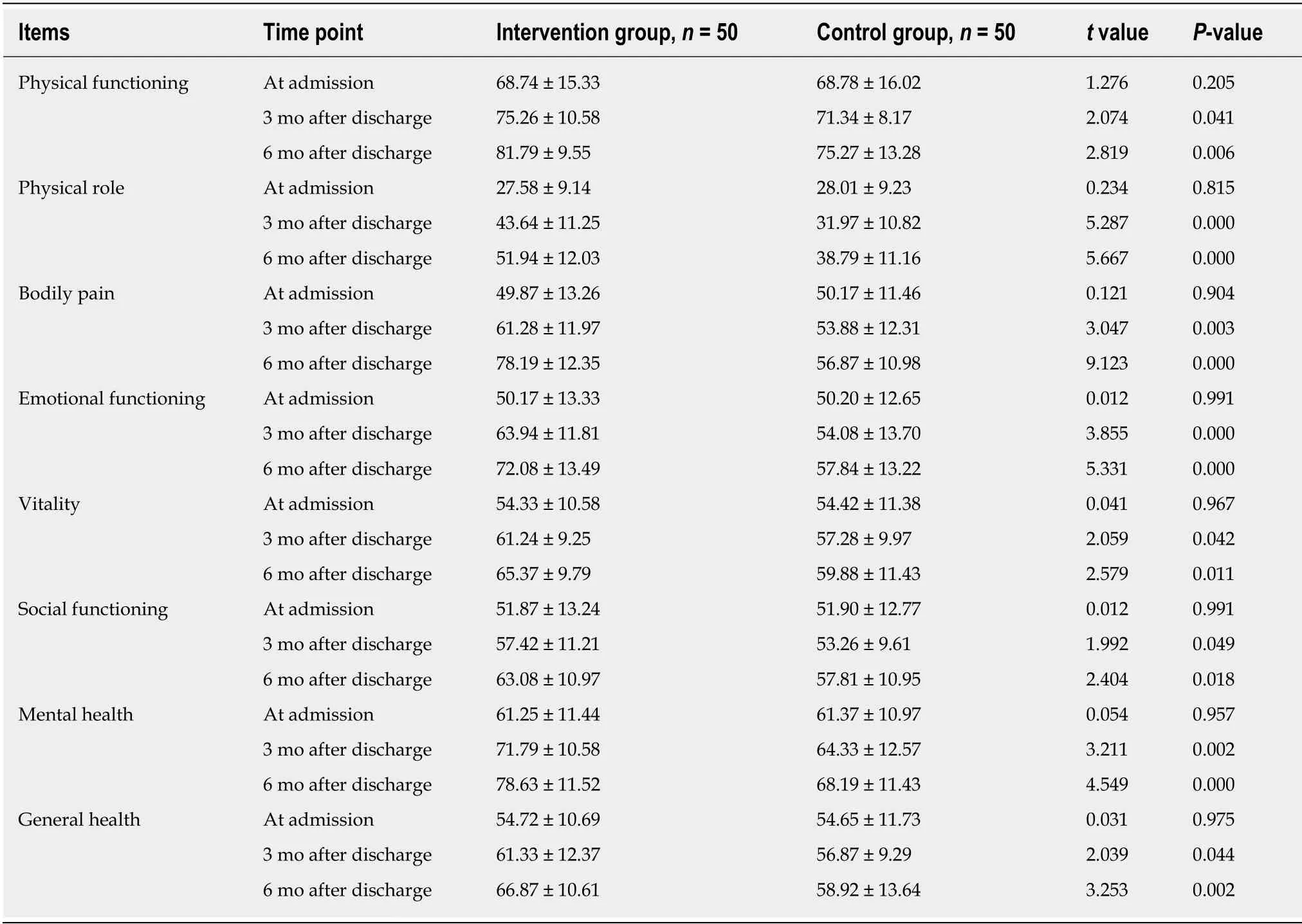
Table 4 Comparison of SF-36 scores between the two groups

Table 5 lnfluencing factors of self-care behaviors
ARTICLE HIGHLIGHTS
Research background
Chronic heart failure (CHF) disease, as a chronic disease, has certain progressive characteristics.Although conventional medication alone can delay the progression of the disease, it often fails to achieve full recovery.Therefore, the current clinical practice is that it can be treated with drugs,but it cannot be cured.This also shows that the addition of scientific nursing intervention on the basis of treatment has important auxiliary significance.The self-care based on full-course individualized health education is a comprehensive nursing measure born in this context.It can make scientific, professional, and individualized health guidance for the patients throughout the whole process, so that patients can form a positive self-care behavior concept, develop a sense of self-care and enables themselves to delay further the disease progression through daily intervention, thus contributing to the improvement of life quality.
Research motivation
At present, there is no unified comprehensive nursing intervention for long-term service of patients with CHF.Although some reports have introduced some nursing interventions, the pertinence and self-participation are not strong, and it is difficult to significantly improve the actual condition of patients.The motivation of this study is to support better the patient's clinical treatment process through self-care based on full-course individualized health education and integrate the nursing intervention into the clinical treatment process, so as to exert more obvious therapeutic effects, help control the condition, and improve the state of life of the patients.
Research objectives
The goal of this study is to explore the application of a new type of nursing intervention - selfcare based on full-course individualized health education - in patients with CHF in order to extend this nursing intervention to the clinical treatment of hospitals at all levels.At present, the core concept of initial nursing intervention has been formed.If it is expanded and promoted in depth, it can make a positive contribution to the prognosis and survival of patients with CHF.
Research methods
A total of 100 patients with CHF in the Cardiology Department were selected for the study.The patients in the control group received the existing CHF routine nursing in our hospital.The patients in the intervention group received the self-care based on full-course individualized health education.After 6 mo of follow-up, 6-min walking distance, self-care behavior score, and SF-36 score were compared, and the influencing factors of patient self-care were analyzed.
Research results
The study found that after applying the self-care based on full-course individualized health education, the patient's 6-min walking distance was longer, and the self-care behavior score and SF-36 score were better.At the same time, logistic regression analysis found that the factors affecting patients' self-care mainly include age, cardiac function classification, and education level.Therefore, the clinical application of self-care based on full-course individualized health education can better improve the overall life quality and clinical prognosis of patients.At the same time, scientific interventions based on age, cardiac function classification, and cultural level are targeted to promote better the patient's self-care effect.However, how to implement it in detail is one of the problems to be solved in the future.
Research conclusions
The new findings of this study are mainly that the self-care based on full-course individualized health education can better assist clinical treatment and can achieve therapeutic effects similar to treatment by intervening in the overall behavior of patients.The new theory proposed in this study is mainly the construction and content exploration of self-care based on full-course individualized health education, which is expected to provide more clearly theoretical ideas for future nursing interventions.The appropriate summary of the current knowledge provided by this study is that self-care based on full-course individualized health education has an important role and has a positive impact on patients.The original insight is that the self-care based on fullcourse individualized health education can achieve a certain level of nursing intervention, which may be similar to conventional care, or better.The new hypothesis is that the self-care based on full-course individualized health education may be a new type of care for patients with CHF.The new method proposed in this study is mainly the formulation and implementation of the self-care based on full-course individualized health education.The new phenomenon found in this study was that the effect of self-care based on full-course individualized health education was better than expected, and it also contributed to the improvement of patients' quality of life.The hypothesis confirmed through experiments in this study is that the self-care based on fullcourse individualized health education has a better clinical prognosis for patients.The implications of this study for clinical practice in the future is that the content of self-care based on full-course individualized health education can be further optimized or expanded, so as to enrich better the theoretical knowledge system and ultimately better serve CHF patients.
Research perspectives
From this study, we can learn that the self-care based on full-course individualized health education is conducive to the patient's condition symptom control and quality of life.A limitation of the study is that the sample size is relatively small.Future research directions include attempts to expand sample size, conduct multi-center research, and further extend follow-up time while expanding the care content system.The best method for the future research is to conduct a stratified study of large sample sizes or a simultaneous study of multi-level medical institutions to obtain more accurate results and conclusions.
杂志排行

World Journal of Clinical Cases的其它文章
- Role of infrapatellar fat pad in pathological process of knee osteoarthritis:Future applications in treatment
- Application of Newcastle disease virus in the treatment of colorectal cancer
- Reduced microRNA-451 expression in eutopic endometrium contributes to the pathogenesis of endometriosis
- Predicting surgical site infections using a novel nomogram in patients with hepatocelluar carcinoma undergoing hepatectomy
- Serological investigation of lgG and lgE antibodies against food antigens in patients with inflammatory bowel disease
- lncidence of infectious complications is associated with a high mortality in patients with hepatitis B virus-related acute-on-chronic liver failure