Role of infrapatellar fat pad in pathological process of knee osteoarthritis:Future applications in treatment
2019-03-14LiFengJiangJingHuaFangLiDongWu
Li-Feng Jiang, Jing-Hua Fang, Li-Dong Wu
Abstract
Key words: Infrapatellar fat pad; Osteoarthritis; Human mesenchymal stem cells
INTRODUCTION
Traditionally speaking, what we said osteoarthritis (OA) always refer to the large joint OA, such as knee OA (KOA) and hip OA.This disease mainly affected women aged over 65, especially obese people and those with previous injuries[1].OA can be considered as a disease that changes not just cartilage but the entire joint organ,including the subchondral bone, menisci, ligaments, periarticular muscle, capsule,and synovium[2].Although most OA cases are caused by mechanically factors that injury the joint tissues, OA is generally recognized as a multifactorial process such as age, heredity, obesity, and nutritional factors[3,4].Recent studies indicated the increased risk of hand OA in obese patients, leading people to focus on the systemic inflammatory mediators secreted by adipose tissue, such as cytokines, interleukins(ILs), growth factors, and adipokines in knee OA[5].Meanwhile, it was found that weight loss can significantly reduce the knee pain in OA patients[6].And it is worth mentioning that OA has been defined as a local inflammatory disease[7].
The infrapatellar fat pad (IPFP), which is located intra-articularly and extrasynovially in the knee joint, is abundant in adipose tissue[8].Considering the IPFP location and the role of inflammatory mediators in the OA process, few researchers are now paying attention on the effect of IPFP in the physiopathology of OA and its new application prospect in this disease.This review is therefore to provide a brief update on the role of IPFP in the process of OA and the innovative therapeutic strategies using IPFP nowadays.
ANATOMIC AND BIOLOGICAL CHARACTERISTICS OF IPFP
The IPFP was first described by Hoffa as “Hoffas fat pad” and “Hoffas disease” in 1904[9].It is an intra-articular and extrasynovial inclusion, covered by synovial membrane[8,10].On the transverse section, the IPFP is located between the patellar retinacula and patellar tendon anteriorly and the trochlear surface of the femur posteriorly; on the sagittal section, it is located inferiorly to the patella and anteriorly to the femoral condyle and intercondylar notch.The IPFP is composed of adipocytes and adipose connective tissues containing collagen that is embedded in an amorphous ground substance encompassing glycosaminoglycans.It can be divided into two portions, inner and outer tissues[11].The inner tissue is the core of the pad with hard pillow-like adipose tissue with cushioning properties, whereas the outer tissue is a soft adipose tissue surrounding the inner tissue.It was described that the inner tissue may undergo a compressive load and the outer tissue may undergo a tensional load.The IPFP has the space-filling properties in the joint cavity, which implies an essential role in joint function such as secreting synovial fluid[12], promoting lubrication[13], and shock absorption.
The periphery of the IPFP is highly vascularized, but the center is poorly vascularized.The blood of IPFP is supplied by two vertical arteries, which are connected by two to three horizontal arteries[14](Figure 1).The primary blood supply originates from the synovial membrane.The IPFP is also richly innervated and contains lymphatic vessels.Bohnsacket al[15]and Witońskiet al[16]found significant distribution of substance-P (SP) nerves inside the IPFP.As a neurotransmitter, SP is released from primary afferent nerve endings and exists in the central, autonomous,and peripheral nerve systems.Besides pain mediation, SP also plays an important role in chronic inflammatory conditions[17].This neurogenous inflammation is hypothesized to attribute to anterior knee pain.As reported, the nerves of the IPFP are originating from the posterior articular branch of the posterior tibial nerve[18].However, a study aiming at knee joint innervation described the innervations of the IPFP in detail[19].The anteromedial portion of the IPFP is innervated by branches of the saphenous, tibial, and obturator nerves and the nerve to vastus medialis, while the anterolateral portion is supplied by branches from the nerve to vastus lateralis as well as the tibial, recurrent peroneal, and common peroneal nerves.The major component of the IPFP is adipose tissue, which can secrete proinflammatory cytokines and growth factors[20]; therefore, the IPFP could be believed to play a role in joint inflammation.As reported, the IPFP could participate in OA synovial inflammation and the severe inflammation in the IPFP was associated with severe pain in OA[21,22].
DUAL ROLE OF IPFP IN KOA
The IPFP itself can not only secrete large amounts of inflammatory cytokines,adipokines, and growth factors, but also respond to the local inflammatory environment in the joint.A cross-talk between the IPFP and the joint exists (Figure 2).Many scholars believe that the IPFP plays an important role in KOA, but these results are not completely consistent[23].
Positive effect of IPFP in KOA
Since the IPFP is located between articular cartilage and bone surface, it may reduce the knee load and protect the knee joint under physiological conditions or in the early stage of KOA[24].It has been reported that the IPFP can improve the distribution of joint fluid in joints by increasing synovial area and reduce the friction during exercise[25].In 2014, Panet al[24]conducted a cohort study of 1100 community populations.They found that the maximum area of female IPFP was negatively correlated with the degree of medial tibial plateau and femoral cartilage damage, and the WOMAC score of knee pain at rest through multivariate analysis.For every 1 cm2increase in the area of the IPFP, the score of female knee pain at rest decreased by 0.86 points after 2.6 years.However, the maximum area of female IPFP had nothing to do with the degree of cartilage damage of the lateral tibial plateau and the WOMAC score when walking or going up and down stairs.The above association is not seen in men.It can be seen that the IPFP is at least associated with pain symptoms in women with KOA and has protective effects on cartilage.
Hanet al[26]conducted a cross-sectional survey of 977 community populations in 2014.The result showed that the area of the IPFP was significantly positively correlated with age, height, and articular cartilage volume.However, the area of the IPFP had nothing to do with body mass index (BMI), although BMI was recognized as a risk factor for KOA.They also found that the area of the IPFP was negatively correlated with osteophytes and subchondral bone marrow edema, and these two indicators were associated with anterior knee pain and cartilage degradation, and were the most common lesions of the subchondral bone in KOA.In addition, some researchers have found that the volume of the IPFP was positively correlated with age though it was not related to the BMI of healthy people and patients with KOA,indicating that changes in body metabolism do not necessarily affect the IPFP, and that the IPFP might not be an inflammatory factor in the early stages of KOA[27].Therefore, the IPFP may play a protective role in the early stages of KOA.
The IPFP may protect the knee joint by secreting protective biochemical factors.Some researchers have found that lipid-mediated lipoxygen A4 levels in IPFP-derived fat-regulating mediators were higher in healthy people, which can prevent cartilage degradation in the knee[28,29].In addition, leptin secreted by the IPFP can promote the production of articular cartilage proteoglycan and type II collagen, stimulate the synthesis of insulin-like growth factor-1 and transforming growth factor-β, enhance chondrocyte proliferation, and thus protect against the pathogenesis of KOA[30-34].What’s more, IPFP-derived mesenchymal stem cells (MSCs) have a greater chondroitin effect than bone marrow-derived MSCs, and it can also block the secretion of proinflammatory mediators in synovial and chondrocytes of OA patients[35,36].A randomized controlled trial in 2015 also showed that mixed transplantation of the IPFP and type I collagen scaffold in the animal model of meniscus injury has better meniscus repair than simple type I collagen scaffold transplantation, which can relieve the formation of KOA to a certain extent[37].
Another important reason may be that the IPFP has the effect of relieving shock,since abnormal biomechanical load plays an important role in the occurrence and development of KOA[38].Meanwhile, the IPFP may also increase the stability of the knee joint, like the patellar ligament, so as to prevent the occurrence of KOA.
Negative effect of IPFP in KOA
The IPFP is in close contact with the synovial layer and articular cartilage, producing cytokines locally in the joint cavity[39].In patients with KOA, the IPFP can secrete higher levels of inflammatory factors and adipokines than subcutaneous fat, such as IL-6, lipase, adiponectin, and visfatin, which can promote the pathological process of KOA[40].
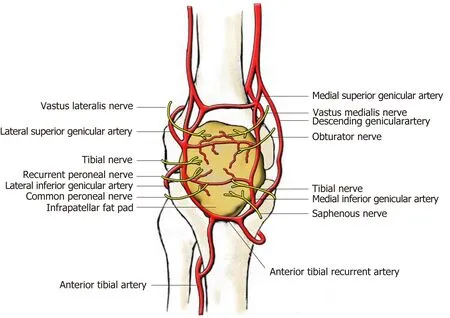
Figure 1 Blood and nerve supply of the infrapatellar fat pad (view from the front).
Obesity state, indeed, is described as a chronic active inflammatory condition[41], as manifested by increased levels of the inflammatory markers C-reactive protein and IL-6 in the systemic circulation of obese individuals.Obesity has been demonstrated as an important risk factor for the incidence of OA, not only because of mechanically overweight load but also metabolic effects.KOA is the most common OA[42].Increased weight in women could elevate the risk for KOA[43], while weight loss may reduce the risk for developing symptomatic KOA among adults[44]and reducing BMI could bring healthy benefits[45].The overload of obese people allows an easy understanding for the mechanical pathogenesis of OA.However, the metabolic factor was observed in the development of OA in non-weight-bearing joints, such as hand OA in overweight or high BMI people.Adipokines secreted by adipose tissue may be involved in the development of OA[5,46].In 2014, Ballegaardet al[22]found that KOOS pain scores in obese patients with KOA were significantly positively correlated with magnetic resonance imaging (MRI) inflammatory signal variables in the IPFP, so inflammatory IPFP in obese patients with KOA may cause knee pain.A cross-sectional study by Cowan in 2015 also showed that patellofemoral arthritis patients had greater IPFP volume on MRI compared with healthy knees, and the volume of IPFP was also positively correlated with KOOS pain scores[47].The reduction of joint space in patients with KOA can lead to inflammation of the IPFP, which can increase the secretion of synovial inflammatory factors on the surface of femoral condyle while causing swelling of the patellar ligament[48,49].
In addition, some studies hold the opposite view that leptin exerts a proinflammatory role, even though leptin secreted by the IPFP has a protective effect on joints.Leptin level was higher in synovial fluid and serum of OA patients compared with controls[50,51]and had a positive correlation with severity of OA[52].Anin vitrostudy showed that leptin could increase matrix metallopreteinase (MMP)production in human osteoarthritic cartilage and correlated with MMP-1 and MMP-3 in OA synovial fluid[53].Leptin could also increase the gene expression of a disintegrin and metalloproteinase with thrombospondin motifs (ADAMTS)-4 and -5[33]and production of NO, PGE2, IL-6, and IL-8[54].Therefore, inflammatory IPFP may also have a negative effect in the pathogenesis of KOA.
ROLE OF IPFP IN ANTERIOR KNEE PAIN
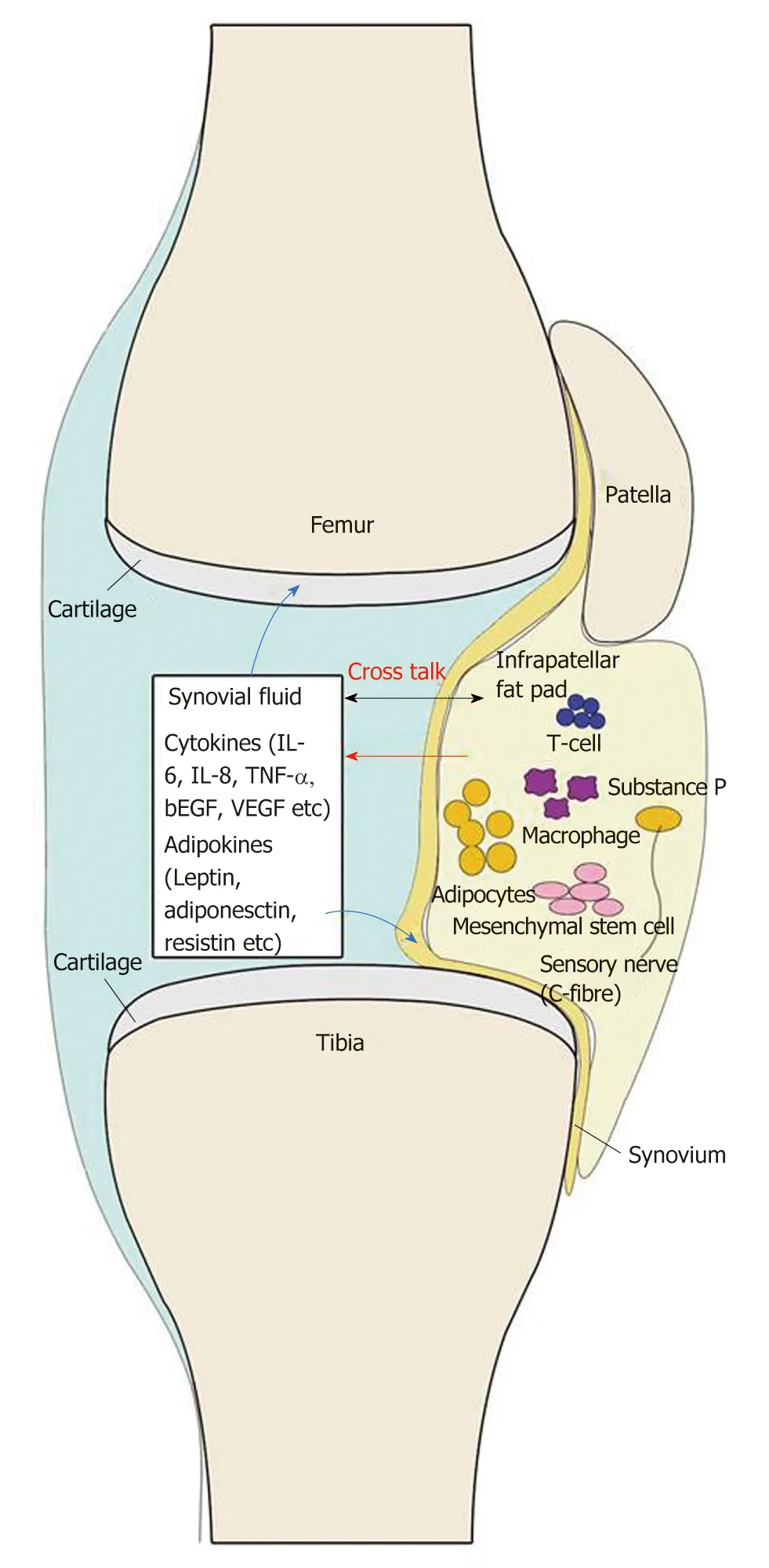
Figure 2 Current view of the infrapatellar fat pad and its interaction with other joint tissues.
In patients with KOA, anterior knee pain is a very important complaint of patients,and it is also a problem that patients want to solve urgently.Benjaminet al[55]and Eivaziet al[56]had proposed the conception of an “enthesis organ”, including the structures like ligament, tendon, or joint capsule attached to bone.The IPFP is one of the most important components of the enthesis organ in the anterior knee region.It is always considered as a potential pathogenic factor of knee pain, especially anterior knee pain.The IPFP pressure varies when the knee motions[57]and hyperpression would induce chronic hyperplasia of the IPFP[58].However, the mechanical hypertrophy or swelling is not the main cause of anterior knee pain.Inflammation is the onset of any pain.The inflammatory mediators increased in the IPFP in patients with anterior knee pain[59].On the other hand, chronic hypertrophy of the IPFP and concomitant soft tissue impingement lead to ischemia, induce the abnormal distribution of SP, and ultimately result in chronic neurogenic tissue inflammation[60,61].Zhanget al[62]showed that the signal intensity change of the IPFP on MRI was closely related to the fluctuation of knee pain symptoms in patients with KOA.However, excision of the IPFP did not improve knee joint function, range of motion, or symptoms of anterior knee pain in patients with KOA, and the exact relationship between the IPFP and knee pain before KOA has not been elucidated[63].
FUTURE APPLICATION OF IPFP IN TISSUE ENGINEERING
Human MSCs have been identified to be multipotent and can be isolated from a large number of adult tissues such as bone marrow, adipose tissue, and umbilical cord blood.MSCs[64,65].They have tissue-regenerative properties that exert potent immunomodulatory, antiapoptotic, antifibrotic, and anti-inflammatory effects[35,66,67].MSCs from the IPFP have been proved to possess significant chondrogenic potential and could provide a clinically feasible source of chondroprogenitor cells[68,69].MSCs from the IPFP are found to be therapeutic for a one-step surgical procedure to regenerate cartilage tissue[70]and improve symptoms of KOA by intra-articular injection[71].The extraction procedure of MSCs derived from bone marrow, however,is invasive[72].In this respect, MSCs isolated from adipose tissue is less invasive and MSCs derived from intra-articular joint tissues are more phenotypically similar to chondrocytes[73].In the presence of chondrogenic media, fat pad-derived MSCs produce Types I, II, and VI collagen.Type VI collagen, which also presents in articular cartilage, plays an important role in the interaction between chondrocytes and the extracellular matrix[74].Furthermore, Luoet al[69,75]demonstrated that IPFP-derived stem cells could produce a structure and spatial composition mimicking those of native articular cartilage[75].Prabhakaret al[76]isolated progenitor cells from the IPFP,expanded, and then seeded them onto a mechanically stable biodegradable polymer film.After culturing the cells for 28 d, they found the self-assembled tissue rich in sulfated glycosaminoglycan and collagen which had the potential to be implanted into defect sites as a potential treatment for cartilage defect regeneration.Therefore,benefiting from its location, minimal invasiveness, and chondrogenic potential, the IPFP could be used for treating OAviarepairing damaged cartilage.
DISCUSSION
In this review, we discuss the role of the IPFP in the disease process of KOA and its application prospect in the treatment of this disease.OA has been regarded as a degenerative joint disease with alteration of articular cartilage.Inflammation is recognized as contributing to the symptoms and progression of OA.Obesity is nowadays considered as a chronic low-grade inflammatory status which is related to the release of inflammatory mediators by adipose tissue.The IPFP is indeed a form of adipose tissue and enlarges with age[27].Due to its close location with articular cartilage and the synovium, it can be speculated with much relationship with OA and synovitis.
Adipocytes, preadipocytes, macrophages, fibroblasts, and other cells in the IPFP release inflammatory mediators such as adipokines and cytokines growth factors that influence cartilage degeneration and synovitis.With the characteristics of minimal invasiveness and multipotentiality, MSCs are now being isolated from the IPFP to provide novel therapies for KOA.
However, further studies should be performed to investigate the precise role of the IPFP in KOA.The role of adipokines in pain should be investigated.In addition,whether adipokines exert their effect on nociceptors in joints remain to be studied.Besides the effect of mediators released by the IPFP on cartilage, tissues such as the synovium and bone marrow are also involved in KOA, so it is also pertinent to explore the effect of mediators on these tissues.
In conclusion, we consider that the IPFP plays an important role in the physiopathology of KOA.Further attention should be focused on the IPFP to explore its new application in KOA.
ACKNOWLEDGEMENTS
Many thanks to Guodong Peng for providing help of the pictures.
杂志排行

World Journal of Clinical Cases的其它文章
- Application of Newcastle disease virus in the treatment of colorectal cancer
- Reduced microRNA-451 expression in eutopic endometrium contributes to the pathogenesis of endometriosis
- Application of self-care based on full-course individualized health education in patients with chronic heart failure and its influencing factors
- Predicting surgical site infections using a novel nomogram in patients with hepatocelluar carcinoma undergoing hepatectomy
- Serological investigation of lgG and lgE antibodies against food antigens in patients with inflammatory bowel disease
- lncidence of infectious complications is associated with a high mortality in patients with hepatitis B virus-related acute-on-chronic liver failure