Systemic lupus erythematosus is easily misdiagnosed as subacute combined degeneration
2019-02-28HuiZhangYitaoHeYiGuo
Hui Zhang, Yitao He, Yi Guo
Department of Neurology, The First Affiliated Hospital of Southern University of Science and Technology, 2nd Clinical Medical College of Jinan University, Shenzhen People's Hospital, Shenzhen, Guangdong Province, China
Abstract
Key words:systemic lupus erythematosus; subacute combined degeneration; immune response; cytomegalovirus; laboratory examination; neurological examination; autoimmune disease
INTRODUCTION
Systemic lupus erythematosus (SLE) is a common autoimmune disease leading to chronic systemic inflammation and tissue damage of various organs and systems, and it can cause some neuropsychiatric syndromes (Hermosillo-Romo and Brey, 2002; Rhiannon, 2008; Lefèvre et al., 2012; Kasama et al., 2016).Subacute combined degeneration (SCD) characterized by degenerative process involves posterior and lateral columns of the spinal cord and peripheral nerve due to vitamin B12 deficiency (Luigetti et al., 2014), folate deficiency (Ravakhah et al., 1995) or all normal (Miscusi et al., 2012).A meta-analysis which summarized case reports from April 1999 to May 2008 showed that SLE is commonly accompanied by multiple neuropsychiatric syndromes, such as epilepsy, cognitive disorder, insanity or cerebrovascular occlusion (Unterman et al., 2011).
However, it has not been reported that SLE is accompanied by neurological defect symptoms presenting as SCD.It will be easy to confuse between SLE and SCD.
Here, we reported a rare case of a 37-year-old woman definitely diagnosed with SLE, but accompanied by neurological defect symptoms presenting as SCD.
SUBJECT AND METHODS
Subject
A 37-year-old woman was admitted to Shenzhen People's Hospital because of numbness and weakness of both upper and lower limbs and urinary retention.She described her lower limbs as stepping on cotton.These symptoms had occurred 20 days before hospitalization and aggravated gradually.She signed the written informed consent (Additional file 1).This study was conducted in accordance with theDeclaration of Helsinki.
She lost 5 kg on weight over the previous 1 month before hospitalization.She was treated with oral mecobalamin intermittently for numbness of right sacral nerve during the past month before hospitalization.She denied the past medical histories of hypertension, diabetes, hepatitis and gastrointestinal diseases.
Methods
Neurological examination:Both upper and lower limbs of the patient were weak with grade 4 myodynamia (McCUNN, 1948; YODH, 1962).Bilateral elbow and knee joints were hyplagesic (Scott and Kothari, 2005).Romber's sign, left side Babinski sign and Chaddock's sign were positive.The tendon reflexes of both upper and lower limbs disappeared.Vibration and joint position sense were decreased.The remainder of the neurologic examination was normal.
Significant laboratory results:red cell count was 2.07 × 109/L (normal range:3.5-5.5 × 109/L), lower than normal; hemoglobin was 85 g/L (normal range:110-150 g/L), lower than normal; average red blood cell volume was 80.8 fl (normal range:82-92 fl), lower than normal; mean corpuscular hemoglobin concentration was 314 g/L (normal range:320-360 g/L), lower than normal; serum iron level was 1.9 μM (normal range:5-32 μM), lower than normal; human cytomegalovirus (CMV) pp65 antigen was positive; CMV antibody IgG was 8.64 AU/mL; CMV antibody IgM was 0.33 AU/mL.Serum immunological tests, including serum antinuclear antibodies, anti-double-stranded DNA antibodies, anti-Ro/Sjögren's antibodies and anti-La/Sjögren's antibodies were all positive.Serum vitamin B12level was elevated, which was 1518.5 pg/mL (normal range:180-918 pg/mL), and folate level was lowered, which was 2.98 ng/mL (normal range:3.0-19.87 ng/mL).
Gastroscopy (FUJINON, made in Japan) showed chronic nonatrophic gastritis, asthecolonoscopy (FUJINON, made in Japan) showed colorectal ulcers, erosions, and chronic colitis.Electromyography and nerve conduction examination (Alpine BioMed ApS, made in Denmark) provided evidence of demyelinating polyneuropathy around the upper and lower extremities.Magnetic resonance imaging (SIEMENS MAGNETOM skyra 3.0T, made in Germany) of the brain and spinal cord showed no obvious abnormalities (Figures 1 and 2).
RESULTS
The patient's physical signs involved peripheral nerve, and posterior and lateral columns of the spinal cord.Blood test showed anemia and low folate level.Vitamin B12level in this patient was elevated, which occurred possibly because of intermittent intake of oral mecobalamin.The clinical symptoms of this patient were improved after treatment with folate (Beijing Xinhui Pharmaceutical Company, China) and vitamin B12 (Eisai Pharmaceutical Company, China).Therefore, this patient was initially diagnosed with SCD.However, she had recurrent fever and joint pain in the limbs during hospitalization.Furthermore, related immune antibodies were positive and the MRI of spinal cord was normal.Thus, the patient was finally diagnosed with SLE.The patient received oral medication of immunotherapy (methylprednisolone 65 mg/day for 3 weeks, followed by gradual dose reduction, and cyclophosphamide 0.4 g per week), mecobalamin (1500 μg/day, Eisai Pharmaceutical Company) and folate (15 mg/day, Beijing Xinhui Pharmaceutical Company).Her neurological symptoms began to improve 1 month later and she returned to work 6 months later.
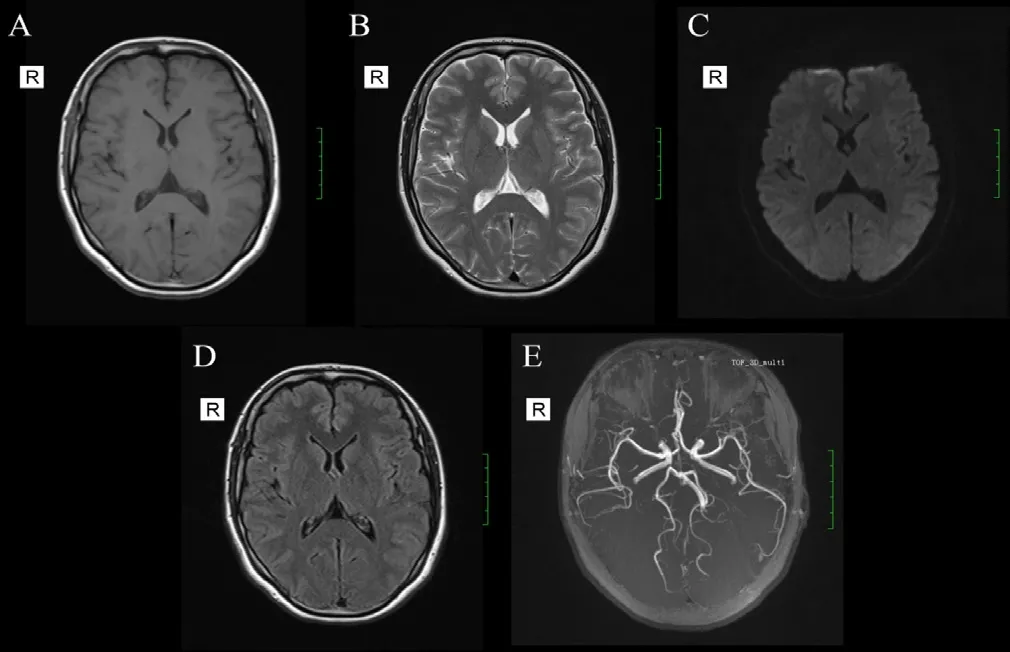
Figure 1:Magnetic resonance imaging (plain scan and angiography) of the brain (A-E) was normal in this case.
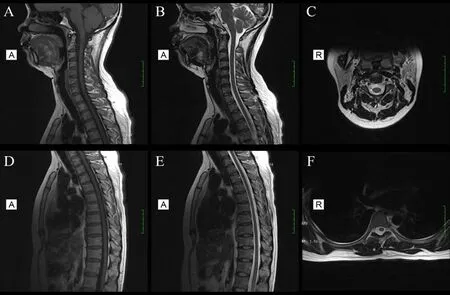
Figure 2:Magnetic resonance imaging (axial and sagittal) of the cervical spinal cord (A-C) and thoracic spinal cord (D-F) was normal in this case.
DISCUSSION
Yoda et al.(2006) reported that human CMV pp65 antigen, a sensitive indicator for early diagnosis and detection of active CMV infection, was closely related to SLE.There is evidence that CMV can lead to demyelination of the peripheral nerve (Visser et al., 1996; Lunn and Hughes, 2011), spinal cord (Kanzaki and Yabuki, 1994; De Fino et al., 2016), and white matter (Zivadinov et al., 2006; Daida et al., 2016) by inducing immune response.Vanheusden et al.(2017) found that CMV infection can aggravate autoimmune-mediated inflammatory diseases in the central nervous system and increase demyelination, especially multiple sclerosis.Related CMV tests were all positive in this patient.So it was speculated that the neurological defect symptoms and signs of this patient may result from nerve damage caused by CMV.A previous study showed that common immune mechanism existed between neuromyelitisoptica spectrum disorder and SCD (Ishii et al., 2013).It might be the immune pathogenesis that causes some cases of SLE having the clinical manifestations of SCD.
In conclusion, SLE is an autoimmune disease that is accompanied by nervous system defect symptoms presenting as SCD.When a young patient featured numbness and weakness of limbs, feeling of stepping on cotton, recurrent fever and joint pain in the limbs, we must be vigilant for SLE and its secondary damage on nervous system, and immune-related antibody examinations should be performed to avoid misdiagnosis.
Additional file
Additional file 1:Informed Consent Form (in Chinese).
Author contributions
Systemic lupus erythematosus diagnosis, therapy, and efficacy evaluation:all authors; data collection and manuscript writing:HZ; manuscript revision:YH; approval of final manuscript:YG.
Conflicts of interest
The authors declared that they have no conflicts of interest to this work.
Financial support
This work was supported by the Medical Research Foundation of Guangdong Province of China (No.A2018176; to YH) and a grant from San Ming Cultivating Funding Project of Shenzhen People's Hospital (No.SYLY201711; to YH).
Institutional review board statement
The study protocol was conducted in accordance with theDeclaration of Helsinki.The patient signed the written informed consent.
Declaration of patient consent
The authors certify that they have obtained this patient' consent form.In the form the patient has given her consent for her images and other clinical information to be reported in the journal.The patient understand that her name and initial will not be published and due efforts will be made to conceal her identity.
Reporting statement
This study followed the Recommendations for the Conduct, Reporting, Editing and Publication of Scholarly Work in Medical Journals developed by the International Committee of Medical Journal Editors.
Biostatistics statement
This study does not need any statistical analysis.
Copyright license agreement
The Copyright License Agreement has been signed by all authors before publication.
Data sharing statement
Individual participant data that underlie the results reported in this article, after deidentification (text and figures), will be available upon request.Data will be available immediately following publication, No end date; for anyone who wishes to access the data.In order to gain access, data requestors will need to sign a data access agreement.Proposals should be directed to heyitaovv@126.com.
Plagiarism check
Checked twice by iThenticate.
Peer review
Externally peer reviewed.
Open access statement
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
杂志排行
Asia Pacific Journal of Clinical Trials:Nervous System Diseases的其它文章
- A central pattern generator in the spinal cord for the central control of micturition:an opportunity for first-in-class drug treatments
- Information for Authors-Asia Pacific Journal of Clinical Trials:Nervous System Diseases
- Effects of galvanic vestibular stimulation versus cervical proprioception training on pain, pressure pain sensitivity, and joint position sense in patients with chronic neck pain:study protocol for a randomized controlled trial
- A reminder incentive system promotes the functional recovery of stroke patients with hemiplegia:a large-sample, single-blind, randomized controlled trial