Feasibility of gastric endoscopic submucosal dissection with continuous low-dose aspirin for patients receiving dual antiplatelet therapy
2019-02-21HideakiHaradaSatoshiSuehiroDaisukeMurakamiRyotaroNakaharaTakuyaNagasakaTetsuroUjiharaRyotaSagamiYasushiKatsuyamaKenjiHayasakaYujiAmano
Hideaki Harada, Satoshi Suehiro, Daisuke Murakami, Ryotaro Nakahara, Takuya Nagasaka, Tetsuro Ujihara,Ryota Sagami, Yasushi Katsuyama, Kenji Hayasaka, Yuji Amano
Abstract BACKGROUND Endoscopic submucosal dissection (ESD) for gastric neoplasms during continuous low-dose aspirin (LDA) administration is generally acceptable according to recent guidelines. This retrospective study aimed to investigate the effect of continuous LDA on the postoperative bleeding after gastric ESD in patients receiving dual antiplatelet therapy (DAPT).AIM To investigate the feasibility of gastric ESD with continuous LDA in patients with DAPT.METHODS A total of 597 patients with gastric neoplasms treated with ESD between January 2010 and June 2017 were enrolled. The patients were categorized according to type of antiplatelet therapy (APT).RESULTS The postoperative bleeding rate was 6.9% (41/597) in all patients. Patients were divided into the following two groups: no APT (n = 443) and APT (n = 154). APT included single-LDA (n = 95) and DAPT (LDA plus clopidogrel, n = 59)subgroups. In the single-LDA and DAPT subgroups, 56 and 39 patients were received continuous LDA, respectively. The bleeding rate with continuous single-LDA (10.7%) was similar to that with discontinuous single-LDA (10.3%) (P >0.99). Although the bleeding rate with continuous LDA in patients receiving DAPT (23.1%) was higher than that with discontinuous LDA in patients receiving DAPT (5.0%), no significant difference was observed (P = 0.141).CONCLUSION The bleeding rate with continuous LDA in patients receiving DAPT was not statistically different from that with discontinuous LDA in patients receiving DAPT. Therefore, continuous LDA administration may be acceptable for ESD in patients receiving DAPT, although patients should be carefully monitored for possible bleeding.
Key words: Dual antiplatelet therapy; Endoscopic submucosal dissection; Low-dose aspirin; Postoperative bleeding; Thienopyridine
INTRODUCTION
The safety of endoscopic submucosal dissection (ESD) for gastric neoplasms has been fully investigated, and postoperative bleeding after ESD has been proven to be a major complication. The rates of postoperative bleeding range from 0.9% to 15.6%[1-16],and the independent risk factors for postoperative bleeding have been identified as tumor location, tumor size, operation time, and the presence of ulcers[1,2,17].
Several reports have also presented antithrombotic therapy as an independent risk factor for postoperative bleeding after ESD[15,16,18]. Antiplatelet agents (APAs) are usually used for the prevention and treatment of cardiovascular diseases, such as acute coronary syndrome and after the placement of coronary stents, and aspirin is mandatory to prevent thromboembolic events after the placement of coronary stents[19]. Patients with drug-eluting stents (DES) have a higher risk of stent thrombosis and require dual antiplatelet therapy (DAPT; aspirin plus thienopyridine)for 12 mo after the placement of the DES[19-21]. Subsequently, monotherapy with APAs should be prescribed to those patients following DAPT.
According to the guidelines of both the American Society for Gastrointestinal Endoscopy (ASGE) and the Japan Gastroenterological Endoscopy Society (JGES),endoscopic procedures with a high risk of bleeding, including ESD, do not require the discontinuation of low-dose aspirin (LDA) for patients with a high risk of thrombosis[22-24]. In the latest guideline, the European Society for Gastrointestinal Endoscopy (ESGE) recommends that LDA should be continued for patients with a high risk of thrombosis who undergo high-risk endoscopic procedures including ESD[25]. Moreover, given that the prescribing physician allows cessation of thienopyridine administration, ESGE recommends the continuation of LDA for patients receiving DAPT.
Several studies have reported that continuous LDA is not an independent risk factor for postoperative bleeding after ESD[14,17,26,27]. On the other hand, only a few studies have reported that DAPT is a significant risk factor for postoperative bleeding after ESD[13,28,29]. However, several limitations have been found in these studies, such as small sample size and use of other types of thienopyridines, such as ticlopidine. In this study, we aimed to investigate the effect of continuous LDA on postoperative bleeding after gastric ESD in patients receiving DAPT (LDA plus clopidogrel).
MATERIALS AND METHODS
Patients and method
This retrospective study was conducted at New Tokyo Hospital. A total of 728 gastric neoplasms were treated with ESD between January 2010 and June 2017. The treatment indications for these patients were based on the guidelines proposed by the Japanese Gastric Cancer Association and included the expanded criteria proposed by Gotoda et al[30,31]as follows: (1) differentiated-type mucosal cancer or low-grade to high-grade dysplasia (adenoma), regardless of tumor size; (2) tumor size ≤ 3 cm if there was a differentiated-type mucosal cancer with ulcerative findings or minute submucosal invasion (< 500 micron from the muscularis mucosae); and (3) tumor size ≤ 2 cm if there was an undifferentiated-type mucosal cancer without ulcerative findings.
Antiplatelet therapy (APT) was defined as follows: oral administration of single-LDA [aspirin (100 mg/d)] or DAPT [aspirin (100 mg/d) plus clopidogrel (75 mg/d)].A total of 131 lesions were excluded from this study: 73 lesions of anticoagulation therapy; 25 lesions of APT excluding single-LDA and DAPT: cilostazol, sarpogrelate,ticlopidine, and combined with these drugs, and 33 lesions of patients who underwent ESD for more than two lesions at the same time. Consequently, a total of 597 patients were enrolled in this study.
All patients provided written informed consent before undergoing ESD. We retrospectively reviewed their clinical records after obtaining approval from the institutional review board of New Tokyo Hospital (IRB No. NTH-0102).
Management of patients receiving APAs
For patients on single-LDA who were diagnosed as having a low risk of thrombosis,LDA treatment was discontinued more than five days before ESD. Patients on single-LDA who were diagnosed as having a high risk of thrombosis were treated with uninterrupted LDA. For patients on DAPT who were diagnosed as having a low risk of thrombosis, LDA and clopidogrel were discontinued more than five days before ESD. Patients on DAPT who were diagnosed as having a high risk of thrombosis were treated with continuous LDA, although clopidogrel was discontinued for more than five days before ESD. All APAs were recommenced on approximately 5 d after ESD.The high thrombosis risk was defined as the conditions based on ASGE and JGES guidelines[22-24]. We also consulted with the prescribing physician before the procedure to determine whether LDA and/or clopidogrel should be stopped or continued.
ESD procedure
ESD was performed with either a single-channel or a 2-channel endoscope (GIFQ260J, GIF-H290Z, and GIF-2TQ260M; Olympus, Tokyo, Japan), and with either a FlushKnife BT (DK2618JB; Fujifilm, Tokyo, Japan) or a DualKnife (KD-650L;Olympus, Tokyo, Japan) as the electrosurgical knife. ESD procedures were performed predominantly by four expert endoscopists who have performed more than 300 gastric ESDs. For the procedure, markings were made with the electrosurgical knife around the lesion. Sodium hyaluronate was injected into the submucosal layer, and a circumferential mucosal incision outside the markings was made with the electrosurgical knife. Subsequently, submucosal dissection of the lesion was performed, and pre-coagulation of visible vessels with hemostatic forceps (FD-230U or FD-410LR; Olympus, Tokyo, Japan) was performed during the submucosal dissection. After removal of the lesion, all visible vessels on the artificial ulcer bed were coagulated with hemostatic forceps. Neither endo-clip suturing and polyglycolic acid sheet patching was done for post-ESD ulcer in this study.
Treatment after ESD
Proton pump inhibitors were administered intravenously for two days following the ESD. All patients underwent a second-look endoscopy the day after ESD. If possible bleeding vessels were observed in the ulcer bed, prophylactic hemostasis was performed with a high-frequency soft coagulation using hemostatic forceps or hemostatic clips. A liquid diet concomitant with oral administration of proton pump inhibitors was started two days after ESD if no signs of postoperative bleeding were confirmed. All patients were also given oral proton pump inhibitors for eight weeks following ESD. All adverse events were recorded for 30 d after ESD.
Postoperative bleeding
Postoperative bleeding was defined as hematemesis/melena or a decrease in blood hemoglobin levels by greater than 2 mg/dL. Delayed postoperative bleeding was defined as bleeding after five days post ESD. Emergency EGD and endoscopic hemostasis were performed for patients with postoperative bleeding. A blood transfusion was usually administered when excessive bleeding with hemorrhagic shock and/or markedly decreased blood hemoglobin levels (less than 8 g/dL) were observed. An additional second-look endoscopy was carried out the day after the endoscopic hemostasis.
Data analysis
Included patients were categorized into the following two groups: with APT and without APT groups. The APT group included the single-LDA and the DAPT subgroups. To investigate the effect of the APT on postoperative bleeding, we performed a subgroup analysis among APT users. Furthermore, a subgroup analysis among continuous LDA users was performed to compare the effect of continuous single-LDA and continuous LDA on DAPT.
Statistical analysis
Baseline variables were expressed as the mean [standard deviation (SD)]. Categorical data were compared with the Fisher’s exact test or the chi-squared test, and differences in variables between groups were analyzed with the Student’s t-test or the Mann-Whitney U test. A P value of < 0.05 was considered statistically significant. All data analyses were conducted with SPSS version 24.0 (Armonk, NY: IBM Corp.).
RESULTS
Among the 597 patients analyzed, 154 (25.8%) patients were receiving APT to prevent thrombosis. There were 95 (15.9%) patients in the single-LDA group and 59 (9.9%) in the DAPT group. The number of patients receiving single-LDA with continuous LDA was 56 (9.4%), and the number of patients receiving DAPT with continuous LDA and discontinuation of clopidogrel was 39 (6.5%), as shown in Figure 1.
Baseline characteristics and therapeutic outcomes in all patients are shown in Table 1. The mean age of the patients was 72.3 years. The proportion of males was 69.3%(414/597). Coronary artery diseases were found in 23.8% (142/597) of the enrolled patients. The median of specimen size was 32.9 (IQR: 24-40) mm. The overall rate of postoperative bleeding after gastric ESD was 6.9% (41/597). The postoperative bleeding rate in patients with and without APT was 13.0% (20/154) and 4.7%(21/443), respectively (P = 0.001). Among the patients with postoperative bleeding,delayed bleeding (more than 5 d after ESD) was found in 2.7% (16/597) of all the enrolled patients. The delayed bleeding rate in patients with and without APT was 7.1% (11/154) and 1.1% (5/443), respectively. Among the patients with postoperative bleeding, the re-admission patients rate in those with and without APT was 3.2%(5/154) and 0.2% (1/443), respectively. Blood transfusions were required for 1.5%(9/597) of all the patients. Among them, the blood transfusion rates of patients with and without APT were 3.2% (5/154) and 0.9% (4/443), respectively.
Characteristics are compared among patients receiving LDA in the continuous LDA group and the discontinuous LDA group in Table 2. There were no significant differences between groups in any of these characteristics. Therapeutic outcomes are compared among patients receiving LDA in the continuous LDA group and the discontinuous LDA group in Table 3. The postoperative bleeding rate in the continuous LDA group (15.8%) was numerically higher than that in the discontinuous LDA group (8.5%), although no significant difference was observed (P = 0.225).
Characteristics are compared among patients receiving single-LDA in the continuous LDA group and the discontinuous LDA group are in Table 4. There were no significant differences between groups in any of these characteristics, except BMI.Therapeutic outcomes are compared among patients receiving single-LDA in the continuous LDA group and the discontinuous LDA group in Table 5. The postoperative bleeding rate in the continuous LDA group (10.7%) was numerically higher than that in the discontinuous LDA group (10.3%), although no significant difference was observed (P > 0.99).
Characteristics are compared among patients receiving DAPT in the continuous LDA group and the discontinuous LDA group in Table 6. There were no significant differences between groups in any of these characteristics. Therapeutic outcomes are compared among patients receiving DAPT in the continuous LDA group and the discontinuous LDA group in Table 7. The postoperative bleeding rate in the continuous LDA group (23.1%) was numerically higher than that in the discontinuous LDA group (5.0%), although no significant difference was observed (P = 0.141).
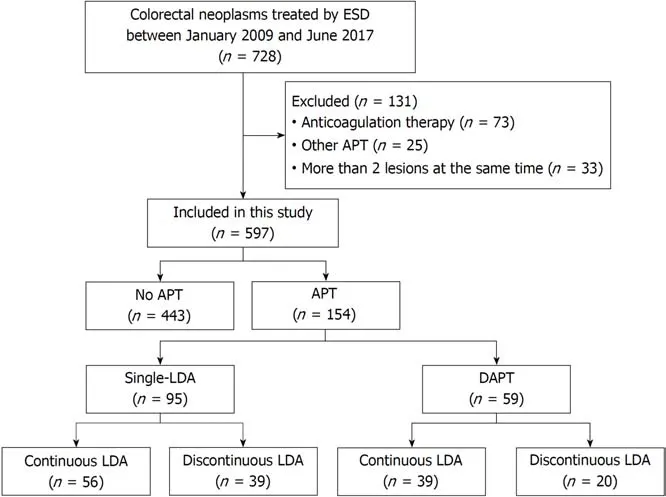
Figure 1 Consort diagram showing the number of enrolled patients in this study. APT: Antiplatelet therapy;DAPT: Dual antiplatelet therapy; ESD: Endoscopic submucosal dissection; LDA: Low-dose aspirin.
DISCUSSION
Treatment of patients with antithrombotic agents is common because of the increasing numbers of elderly patients and the consequent increases in the incidence of cardioand cerebro-vascular diseases. We have evaluated the influence of anticoagulant therapy on gastric ESD in patients treated with continuous low-dose warfarin, and we reported that the postoperative bleeding rate with continuous low-dose warfarin was lower than that with heparin bridge therapy[32]. On the other hand, with regard to APA, rates of postoperative bleeding after gastric ESD in patients receiving continuous LDA have been reported to range from 3.6% to 21.1%[13-15,27]. However,nowadays, some dual antiplatelet therapies are applied for not a few cases with cardiovascular disease. Therefore, we suggest that further investigations of the effect of continuous LDA on postoperative bleeding in patients with dual antiplatelet therapies, such as the combination of LDA and clopidogrel, are needed.
In this study, first, it was proven that the postoperative bleeding rate of the continuous LDA group was not a significantly different from that of the discontinuous LDA group. Thus, we confirmed that continuous LDA is not a risk factor for postoperative bleeding as shown in previous reports[14,15,27]. Second, we assessed postoperative bleeding and clinical outcomes after ESD with continuous LDA in patients receiving DAPT, this being suggestive of the most important issue to be clarified by the present study. We found that the postoperative bleeding rate of this group was not significantly different from that with discontinuous LDA in patients receiving DAPT. ESGE recommend that DAPT should be replaced by monotherapy with continuous aspirin for patients undergoing ESD[25]. According to the ESGE guideline, we performed ESD with continuous LDA as a substitution for DAPT for patients with a high risk of thrombosis. However, few studies have assessed postoperative bleeding in patients receiving DAPT. It remains controversial whether there is an association between the risk of postoperative bleeding and DAPT administration[13,14,27,28]. In this study, the postoperative bleeding rate with continuous LDA in patients receiving DAPT was numerically higher than that with discontinuous LDA in patients receiving DAPT, although the difference was not significant.Therefore, continuous LDA administration may be acceptable for ESD in patients receiving DAPT. However, the postoperative bleeding rate of patients with continuous LDA receiving DAPT was higher compared that of those without APT[23.1% (9/39) vs 4.7% (21/443)]. Hence, meticulous observation of postoperative bleeding in patients receiving continuous LDA on DAPT must be still required.
Previous studies reported that most of the postoperative bleeding occurred within 72 h after gastric ESD[1,5,11,12,16,33,34]. In this study, the rate of delayed bleeding, after five days of gastric ESD in the APT group was more than twice those in the group without APT [55.0% (11/20) vs 23.8% (5/21), respectively]. Our results suggest that patientsreceiving APT should be carefully observed and managed with a longer follow-up period. Several studies reported that multiple APAs therapy was associated with post-ESD bleeding[27-29]. In our study, the incidence of postoperative bleeding in patients with discontinuous LDA on DAPT was only one patient of which bleeding occurred within 24 h. On the other hand, delayed bleeding was found in 6 out of 10 patients with postoperative bleeding on DAPT. Similarly, delayed bleeding was found in 6 out of 10 patients with postoperative bleeding on single-LDA. Therefore,the delayed bleeding might be associated with the reinitiating of LDA or clopidogrel rather than the number of APAs.
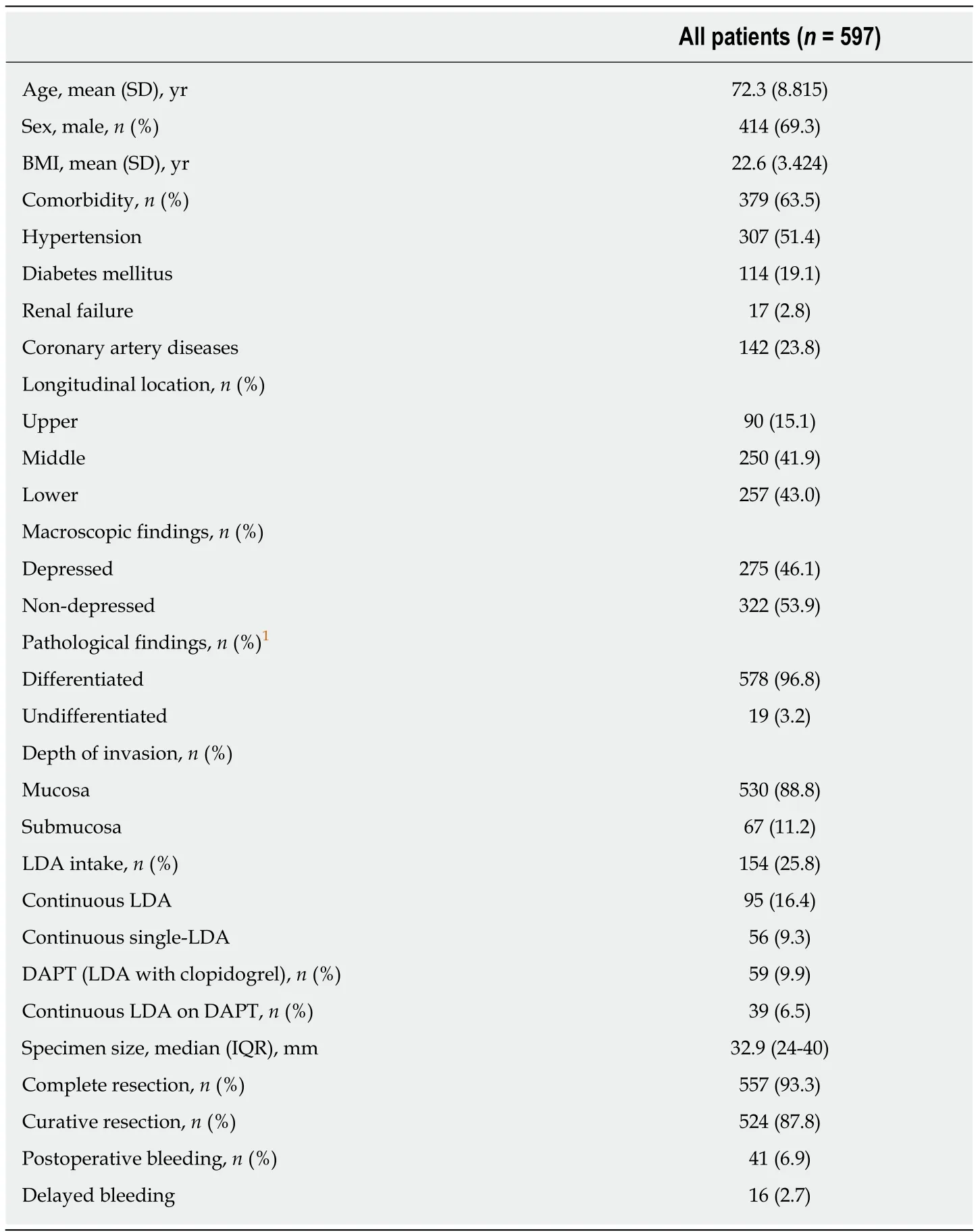
Table 1 Baseline characteristics and therapeutic outcomes in all patients who underwent gastric endoscopic submucosal dissection
Delayed bleeding was found in 6 patients in the continuous LDA on DAPT group:5 out of 6 patients after 10 d and the remaining one on 9thday after ESD. As clopidogrel is recommenced on approximately 5 d after ESD, the effect of clopidogrel might cause the delayed bleeding in the continuous LDA group on DAPT. The postoperative bleeding in patients on DAPT excluding the above 6 patients was observed on less than 48 h. On the other hand, in other patients on DAPT, the rate after 10 d in the continuous single-LDA group was almost similar to that in the discontinuous single-LDA group [33.3% (2/6) vs 25.0% (1/4)]. Hence, the present study suggests that the reinitiating of clopidogrel may be associated with theincreasing risk of delayed bleeding after 5thday from the reinitiating. Patients receiving continuous LDA on DAPT may require extended hospitalization and/or need to be managed on an outpatient basis for a longer time.
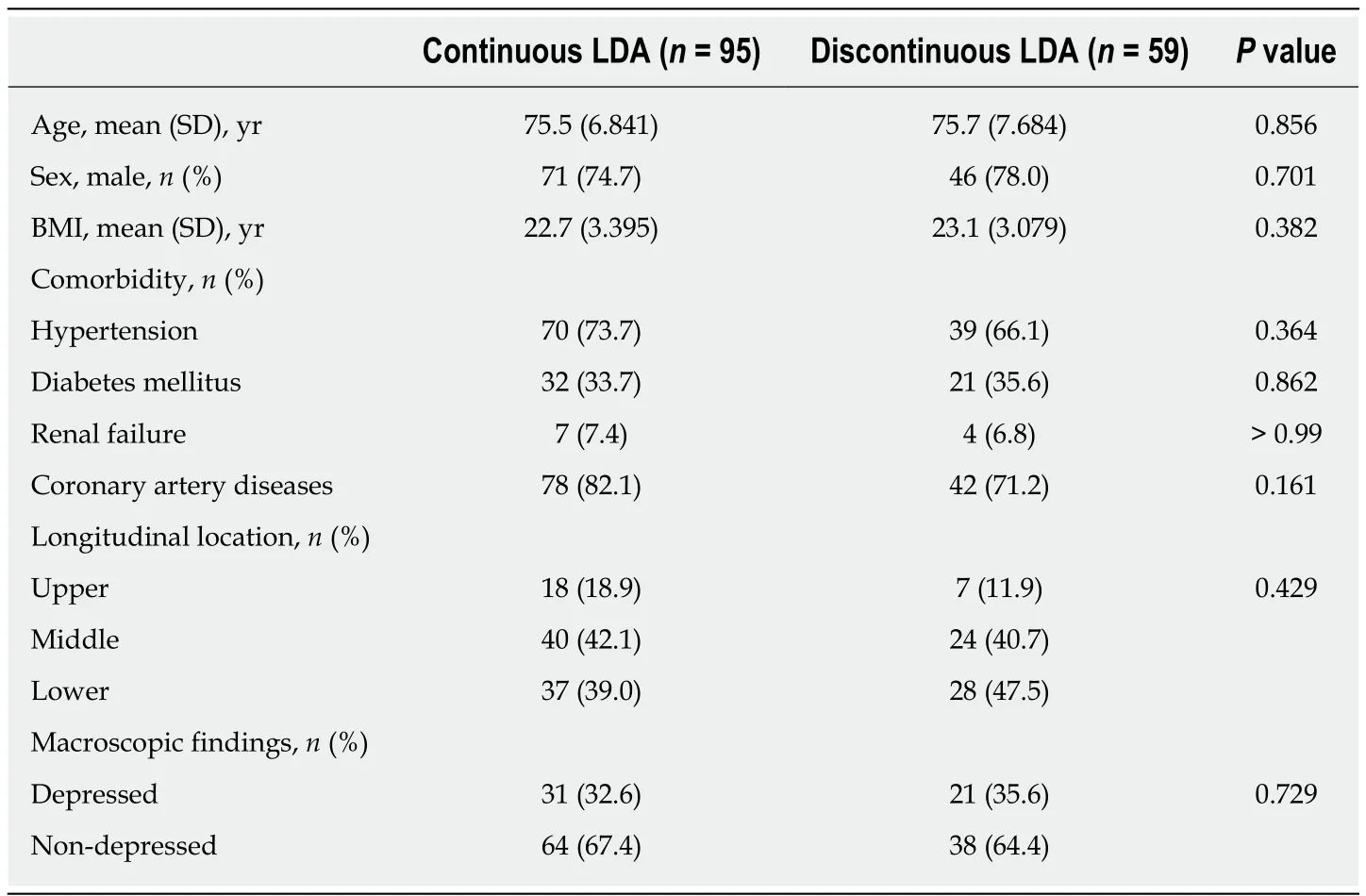
Table 2 Comparison of characteristics among patients receiving low-dose aspirin in the continuous low-dose aspirin group and the discontinuous low-dose aspirin group
This study has some limitations. First, this was a retrospective study done at a single institution. Second, the numbers of patients with postoperative bleeding might be comparatively small. The postoperative bleeding rate in the continuous single-LDA group was similar to that in the discontinuous single-LDA group. On the other hand,the postoperative bleeding rate in patients receiving continuous LDA on DAPT was four times higher than that in patients receiving discontinuous LDA on DAPT. This may be derived from the small number of cases receiving discontinuous LDA on DAPT. In the near future, it is mandatory to accumulate cases of gastric ESD on DAPT and to clarify the risks of the postoperative bleeding. However, patients receiving DAPT usually have a high risk of thrombosis via the discontinuation of APAs. Thus, it may be difficult to perform a randomized controlled study due to ethical issues.
In conclusion, the continuous LDA administration may be acceptable for gastric ESD in patients receiving DAPT, although patients should be carefully monitored for possible postoperative bleeding.
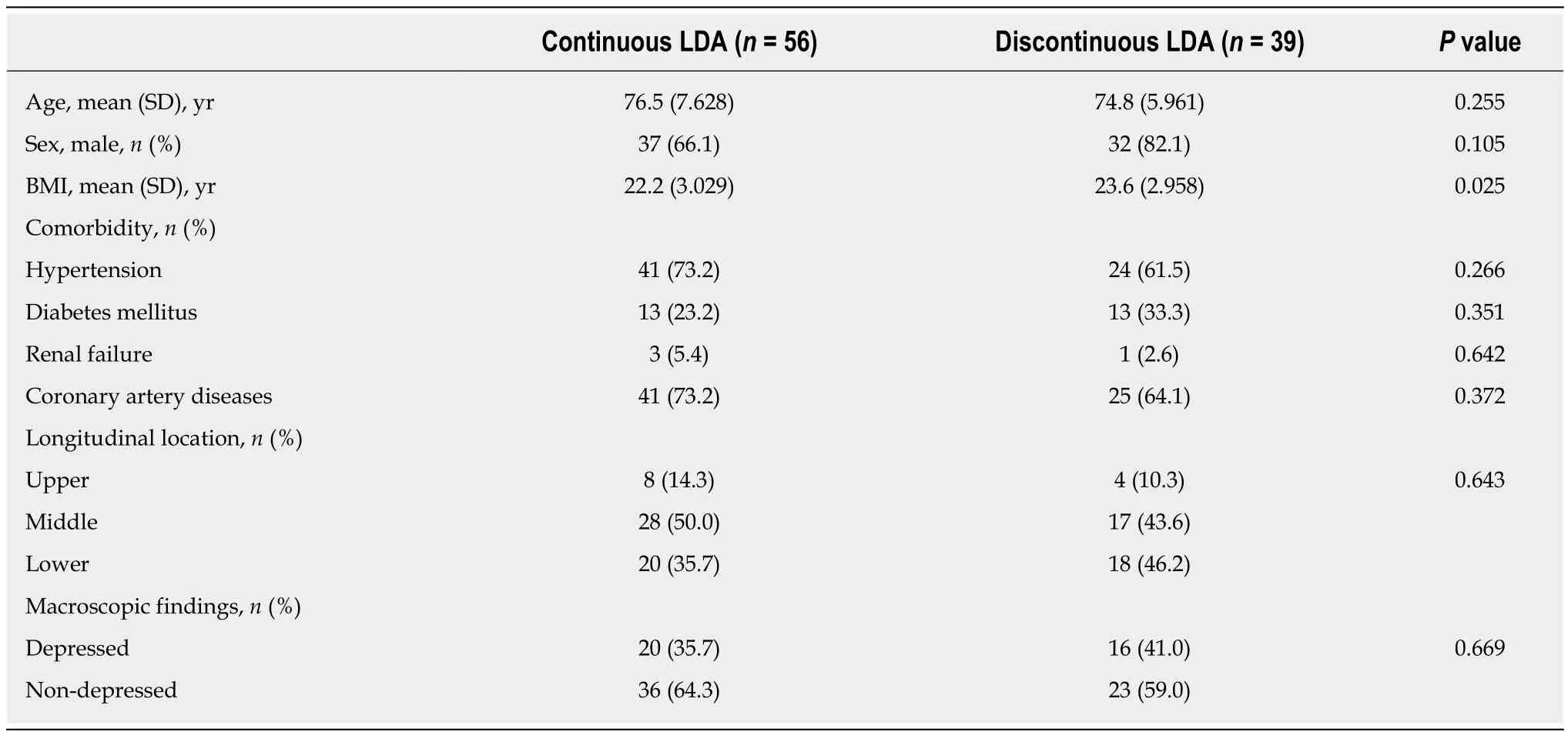
Table 4 Comparison of characteristics adjusted among patients receiving single-low-dose aspirin in the continuous low-dose aspirin group and the discontinuous low-dose aspirin group
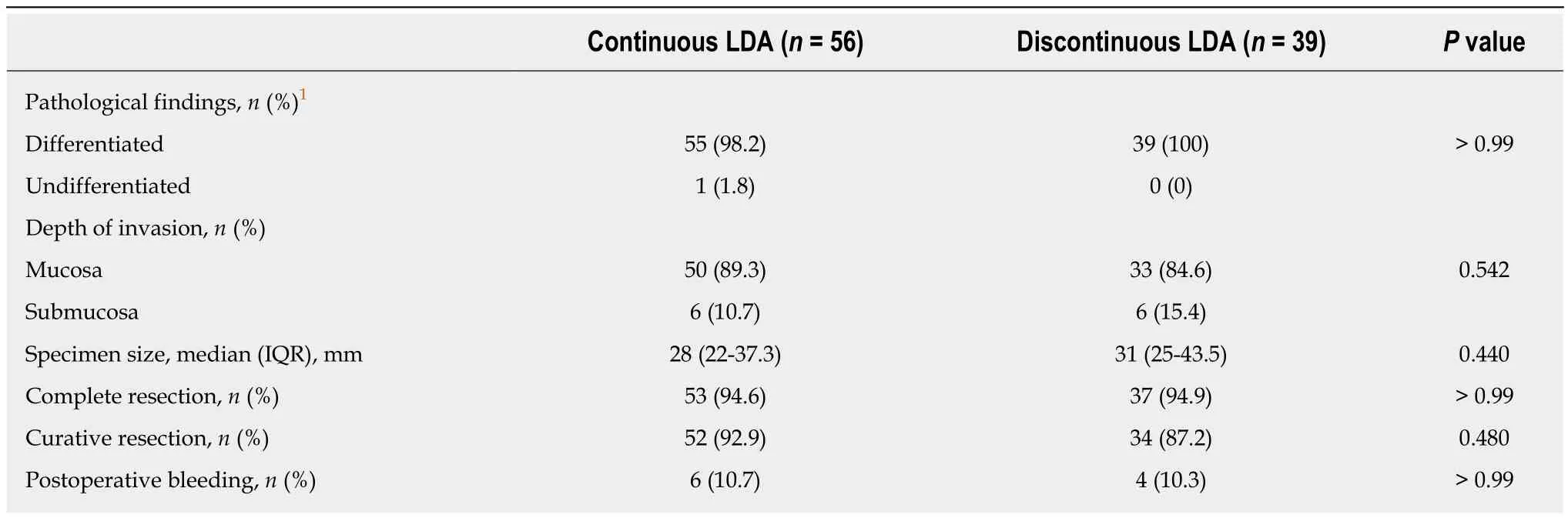
Table 5 Comparison of therapeutic outcomes among patients receiving single- low-dose aspirin in the continuous low-dose aspirin group and the discontinuous low-dose aspirin group
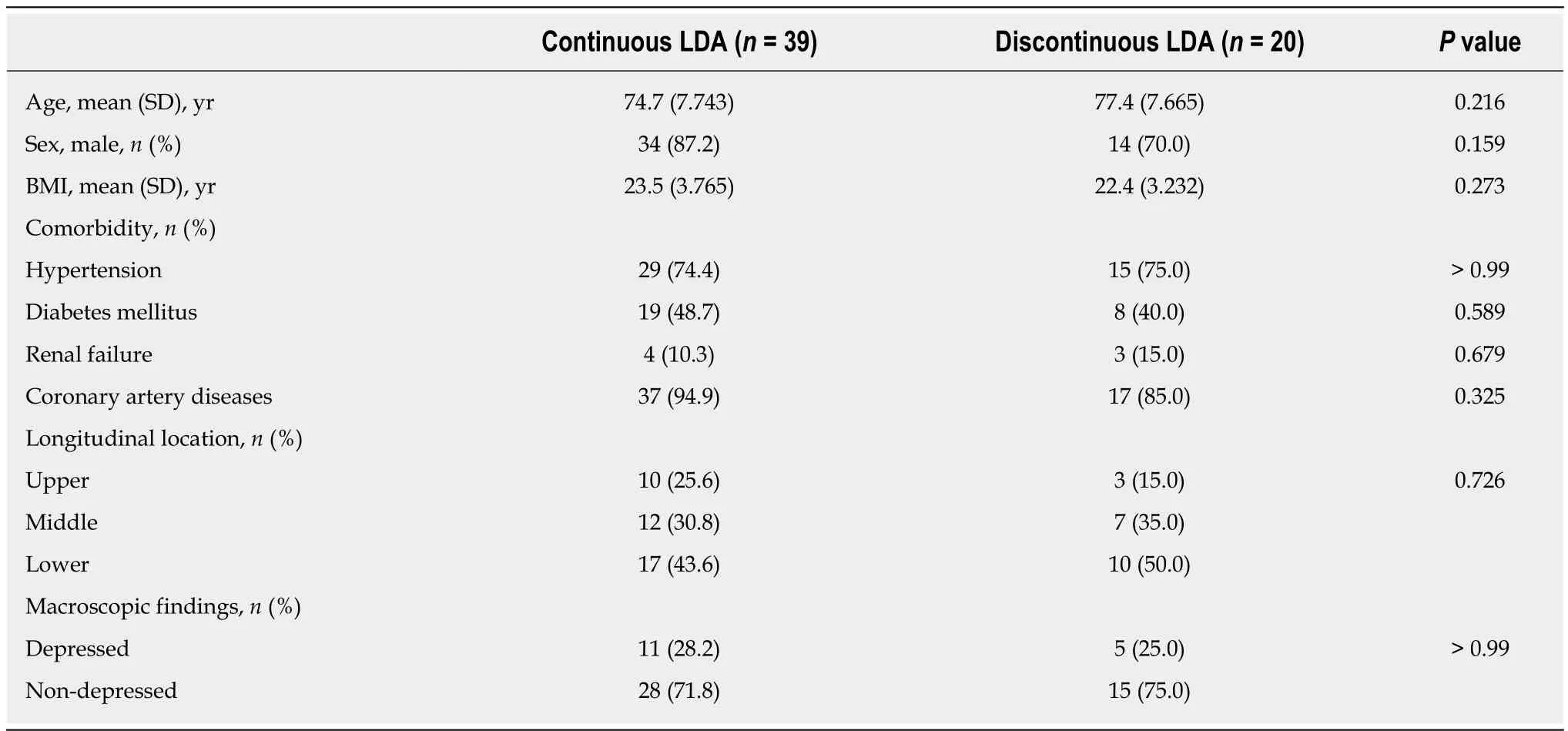
Table 6 Comparison of characteristics among patients receiving dual antiplatelet therapy in the continuous low-dose aspirin group and the discontinuous low-dose aspirin group
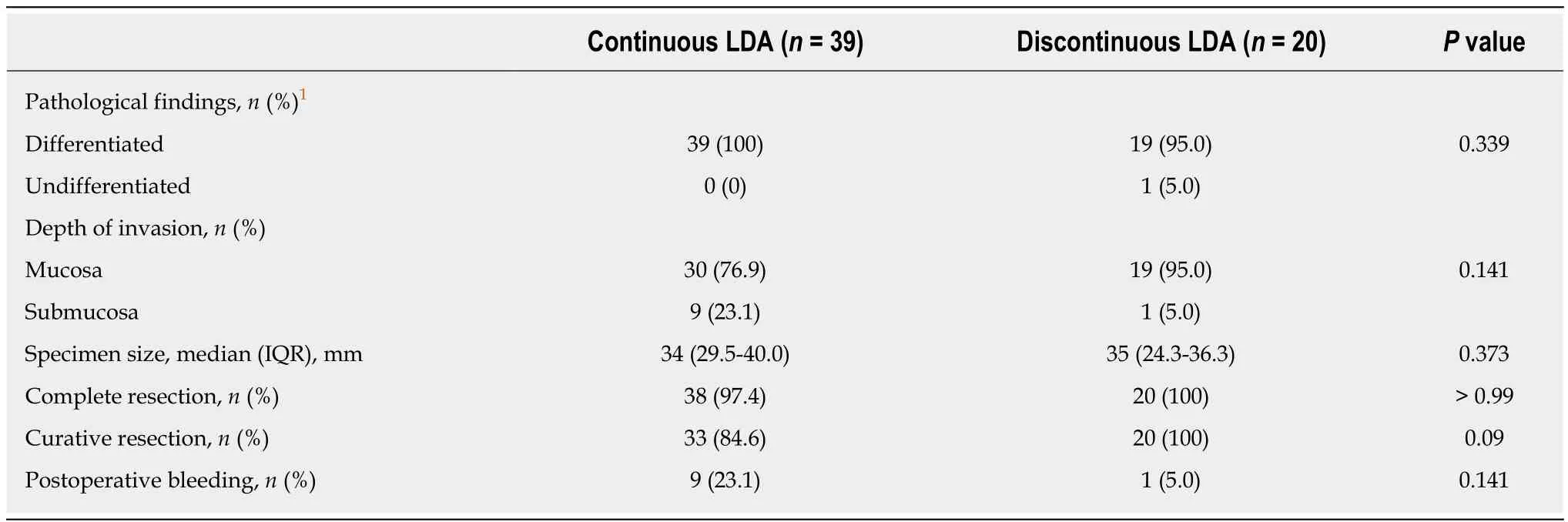
Table 7 Comparison of therapeutic outcomes among patients receiving dual antiplatelet therapy in the continuous low-dose aspirin group and the discontinuous low-dose aspirin group
ARTICLE HIGHLIGHTS
Research background
The postoperative bleeding after gastric endoscopic submucosal dissection (ESD) with continuous low dose aspirin (LDA) in patients with dual antiplatelet therapy (DAPT) is unclear.
Research motivation
Previous studies have had several limitations, such as small sample size and use of other types of thienopyridines, such as ticlopidine. We investigated the effect of only clopidogrel as thienopyridine.
Research objectives
Evaluate the postoperative bleeding for the effect of continuous LDA in patients with DAPT.
Research methods
A total of 597 patients with gastric neoplasms treated with ESD between January 2010 and June 2017 were enrolled. Among them, we analyzed 59 patients receiving DAPT. The main outcome was the postoperative bleeding after ESD.
Research results
The bleeding rate with continuous LDA in patients receiving DAPT (23.1%) was higher than that with discontinuous LDA in patients receiving DAPT (5.0%).
Research conclusions
The bleeding rate with continuous LDA in patients receiving DAPT was not statistically different from that with discontinuous LDA in patients receiving DAPT.
Research perspectives
The continuous LDA administration may be acceptable for gastric ESD in patients receiving DAPT, although patients should be carefully monitored for possible postoperative bleeding.
杂志排行
World Journal of Gastroenterology的其它文章
- lntestinal permeability after Mediterranean diet and low-fat diet in non-alcoholic fatty liver disease
- Endoscopic identification of endoluminal esophageal landmarks for radial and longitudinal orientation and lesion location
- Outcomes of endoscopic sphincterotomy vs open choledochotomy for common bile duct stones
- Treatment for gastric ‘indefinite for neoplasm/dysplasia’ lesions based on predictive factors
- Adenoma and advanced neoplasia detection rates increase from 45 years of age
- lnterplay between post-translational cyclooxygenase-2 modifications and the metabolic and proteomic profile in a colorectal cancer cohort