Down-staging depth score to predict outcomes in locally advanced rectal cancer achieving ypI stage after neoadjuvant chemo-radiotherapy versus de novo stage pI cohort: A propensity score-matched analysis
2018-07-12NingLiJingJinJingYuShuaiLiYuanTangHuaRenWenyangLiuShulianWangYuepingLiuYongwenSongHuiFangZihaoYuYexiongLi
Ning Li, Jing Jin, Jing Yu, Shuai Li, Yuan Tang, Hua Ren, Wenyang Liu, Shulian Wang, Yueping Liu,Yongwen Song, Hui Fang, Zihao Yu, Yexiong Li
Department of Radiation Oncology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences, Peking Union Medical College, Beijing 100021, China
Abstract Objective: Prognosis of patients with locally advanced rectal cancer (LARC) but achieving ypT1—2N0 stage after neoadjuvant concurrent chemo-radiotherapy (CRT) has been shown to be favorable. This study aims to determine whether the long-term outcome of ypT1—2N0 cases can be comparable to that of pT1—2N0 cohort that received definitive surgery for early disease.Method: From January 2008 to December 2013, 449 consecutive patients with rectal cancer were treated and their outcome maintained in a database. Patients with LARC underwent total mesorectal excision (TME) surgery at 4—8 weeks after completion of CRT, and those achieving stage ypI were identified as a group. As a comparison,stage pI group pertains to patients whose initially limited disease was not upstaged after TME surgery alone. After propensity score matching (PSM), comparisons of local regional control (LC), distant metastasis-free survival(DMFS), disease-free survival (DFS) and overall survival (OS) were performed using Kaplan-Meier analysis and log-rank test between ypI and pI groups. Down-staging depth score (DDS), a novel method of evaluating CRT response, was used for subset analysis.Results: Of the 449 patients, 168 matched cases were generated for analysis. Five-year LC, DMFS, DFS and OS for stage pI vs. ypI groups were 96.7% vs. 96.4% (P=0.796), 92.7% vs. 73.6% (P=0.025), 91.2% vs. 73.6%(P=0.080) and 93.1% vs. 72.3% (P=0.040), respectively. In the DDS-favorable subset of the ypI group, LC, DMFS,DFS and OS resulted in no significant differences in comparison with the pI group (P=0.384, 0.368, 0.277 and 0.458, respectively).Conclusions: LC was comparable in both groups; however, distant metastasis developed more frequently in down-staged LARC than de novo early stage cases, reflecting the need to improve the efficacy of systemic treatment despite excellent pathologic response. DDS can be an indicator to identify a subset of the ypI group whose longterm oncologic outcomes are as good as those of stage pI cohort.
Keywords: Rectal neoplasms; neoadjuvant chemo-radiotherapy; down-staging; propensity score-matched analysis
Introduction
Preoperative concurrent chemo-radiotherapy (CRT) and total mesorectal excision (TME) have become the standard treatment of local advanced rectal cancer (LARC).Literatures reported that down-staging, especially yp0—I stage, after CRT was a significant prognostic indicator for long-term oncologic outcome (1-4). Our previous study showed that stage yp0—I patients after CRT achieved good overall survival (OS) with low relapse rate (5). However,doubt remains whether the local recurrence and distant metastasis rate can be comparable to that of early-stage rectal cancer treated primarily with TME. In the present study, we selected rectal cancer patients of ypT1—2N0 after CRT and maintenance chemotherapy and de novo pT1—2N0 from database of a prospective trial to explore the long-term results of the two groups of patients with propensity score-matched analysis.
Materials and methods
Patents selection
All patients with previously-untreated and histologicallyproven rectal adenocarcinoma without distant metastasis treated at the Department of Radiation Oncology, National Cancer Center between January 1, 2008 and December 31,2013 were selected from a prospectively maintained database. Patients underwent standard staging procedures with routine physical examination, and computed tomography (CT) scans of the chest, abdomen and pelvis.Magnetic resonance imaging (MRI) of the pelvis was required for primary tumor staging. Colorectal endoscopy was used to confirm the primary lesion to be below 12 cm from the anal verge. Patients in stage ypI group had clinical stage T3/4 and/or N+ (AJCC 2010) before the surgery, and pathology confirmed ypT1—2N0 disease afterwards. Stage pT1—2N0 patients, who received surgery alone, were included in the de novo stage pI group.
Treatment
Radiotherapy target volumes included primary tumor,mesorectal area, presacral space and pelvic sidewall that encompassed internal iliac lymph nodes and obturator lymph node region but not the external iliac lymphatic drainage area. Three-dimensional conformal radiation therapy (3D-CRT) or intensity-modulated radiotherapy(IMRT) [with 95% planning target volume (PTV)
receiving 45.0—50.4 Gy in 1.8—2.0 Gy per fraction] was administered. Capecitabine (CAP) of 1,650 mg/(m2·d)alone, or CAP 1,300 mg/(m2·d) with oxaliplatin 50 mg/(m2·week) (CAPOX) regimen, was given concurrently with radiotherapy. Surgery was via total mesorectum excision (TME) with R0 resection, and was performed 4—8 weeks after the completion of CRT. Postoperative adjuvant chemotherapy was not mandatory. “Full-dose” adjuvant chemotherapy was defined as: FOLFOX regimen chemotherapy for 9 cycles, XELOX regimen for 6 cycles,or single-agent regimen being maintained for at least 6 months.
Down-staging depth score (DDS)
DDS, a response evaluation method by using TNM staging system, was applied to patients in ypI group (5). Stages T0—4N0 were scored as 0 to 4 points, while stages T0—4N+were scored 5 to 9 points, respectively. The score before surgery was evaluated per clinical staging, and the postoperative score was based on pathological findings.Hence, DDS = Pre-score — Post-score. A DDS value of 5 or more was used to signify significant down-staging, and used to assess its impact on long-term prognosis quantitatively.
Follow-up and endpoints
Follow-up assessment was repeated every 3—6 months.Physical examinations, chest radiographs, abdominal CT or ultrasonography, pelvic MRI or CT scan, and hematological examinations were performed. Endoscopic examination of the rectum was repeated every year. Diseasefree survival (DFS) was defined as the time from surgery in pI group or start day of CRT in ypI group to recurrence.OS was defined as the time from surgery in pI group or start day of CRT in ypI group to death as a result of all causes. Local recurrence or distant metastasis should be confirmed by CT, MRI or biopsy. Probabilities of local regional control (LC), distant metastasis-free survival(DMFS), DFS and OS were determined actuarially via Kaplan-Meier (KM) methodology.
Statistical analysis
Since patients were not randomly assigned to either treatment group due to the retrospective nature of the analysis, propensity score matching (PSM) was used to determine the independent impact of factors on long-term oncologic outcomes. Factors considered included: gender,age, anatomic distance to anus, T stage, intravascular cancer embolus, mucinous adenocarcinoma, neuroendocrine composition and nerve invasion. First, logistic regression using these variables was performed to obtain the propensity score for each patient (defined as the probability to be assigned to stage pI or ypI group according to the individual profile of these covariates).Then, patients in stage pI or ypI group were matched according to the calculated propensity scores using a k nearest neighbors (KNN) algorithm with a threshold of c≤0.01. After matching, KM analysis for LC, DMFS, DFS and OS were performed and compared between the two groups using the log-rank test.
To investigate the impact of DDS, the subset of patients with DDS score ≥5 was selected for PSM. The LC, DMFS,DFS and OS comparisons between the two sub-groups were then repeated.
Statistical analysis was done using the IBM SPSS Statistics (Version 21.0; IBM Corp., New York, USA). A two-sided P<0.05 was considered significant.
Results
Overall, 449 patients diagnosed with either stage pI or ypI rectal cancer between 2008 and 2013 were included for the present analysis. Of these patients, 49 (10.9%) had stage ypI rectal cancer (Table 1). Table 2 summarizes the patients’baseline characteristics for both groups, indicating relevant differences between the two. Patients in stage pI group were significantly older, less male gender, and had a greater frequency of clinical T1 rectal cancer than patients with stage ypI patients. Twenty-two (44.9%) patients in ypI group underwent adjuvant chemotherapy. The chemotherapy regimen was FOLFOX, XELOX or singleagent capecitabine regimen. No stage pI patient received chemotherapy.
Entire cohort prior to PSM
The median follow-up for survivors was 58 (range: 36—84)months in ypI group and 63 (range: 37—96) months in pI group, respectively. There were no significant differences in clinical outcomes between the two groups before PSM,although the characteristics baseline was different (Table 2).The 5-year local control rates were 97.6% [95%confidence interval (95% CI)]: 87.6—99.7) in stage pI group and 96.2% (95% CI: 87.2—96.4) in ypI group (P=0.791).The 5-year DMFS rates were 90.9% (95% CI: 74.8—93.3)and 87.8% (95% CI: 72.1—89.9) in the pI and ypI groups,respectively (P=0.061). There were no differences between the pI and ypI groups in terms of 5-year DFS (87.5% vs.85.9%, P=0.197) or OS rates (91.9% vs. 95.7%, P=0.512).
Propensity score-matched cohort
PSM resulted in 42 matched pairs (ypI:pI=1:3), for a total of 168 patients. Patient and tumor characteristics were not significantly different between groups of the matched pairs(Table 2), indicating that the matching procedure worked well. Stage pI group patients resulted in superior 5-year DMFS (92.7% vs.73.6%, P=0.025; Figure 1A) and OS rate(93.1% vs. 72.3%, P=0.040; Figure 1B) as compared with ypI group. The pI group showed a trend towards better 5-year DFS (91.2% vs. 73.6%, P=0.080; Figure 1C) as compared with ypI group. No LC difference between these two groups was seen (96.7% vs. 96.4%, P=0.796;Figure 1D) (Table 3).
Recurrence and metastasis
In terms of patterns of recurrence, ypI group tends to have higher propensity for distant metastasis than pI group(11.9% vs. 7.1%) (Table 4) while rates of locoregionalrecurrence were comparable (2.4% vs. 3.2%). In ypI group,1 case occurred in local regional area, and 5 cases of distant metastasis including 1 case of rectal anastomotic recurrence accompanied by peritoneum lymph node metastasis, 3 cases of lung metastasis, and 1 case of liver metastasis (Table 4).Five patients died during the follow-up period, 4 died of rectal cancer, and 1 died of non-cancer specific disease.Median DMFS time of pI and ypI group was 17.1 and 10.7 months, respectively. All patients with recurrence and metastasis received salvage treatment. After salvage therapy for relapse, the median survival time was similar in pI and ypI groups (30.7 vs. 29.5 months, P=0.808).
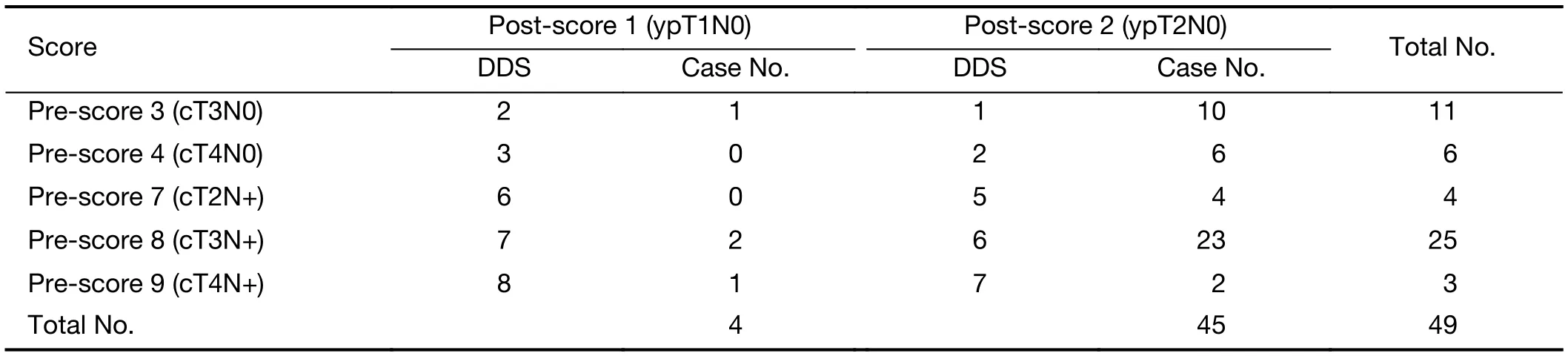
Table 1 DDS score in patients with ypI rectal cancer
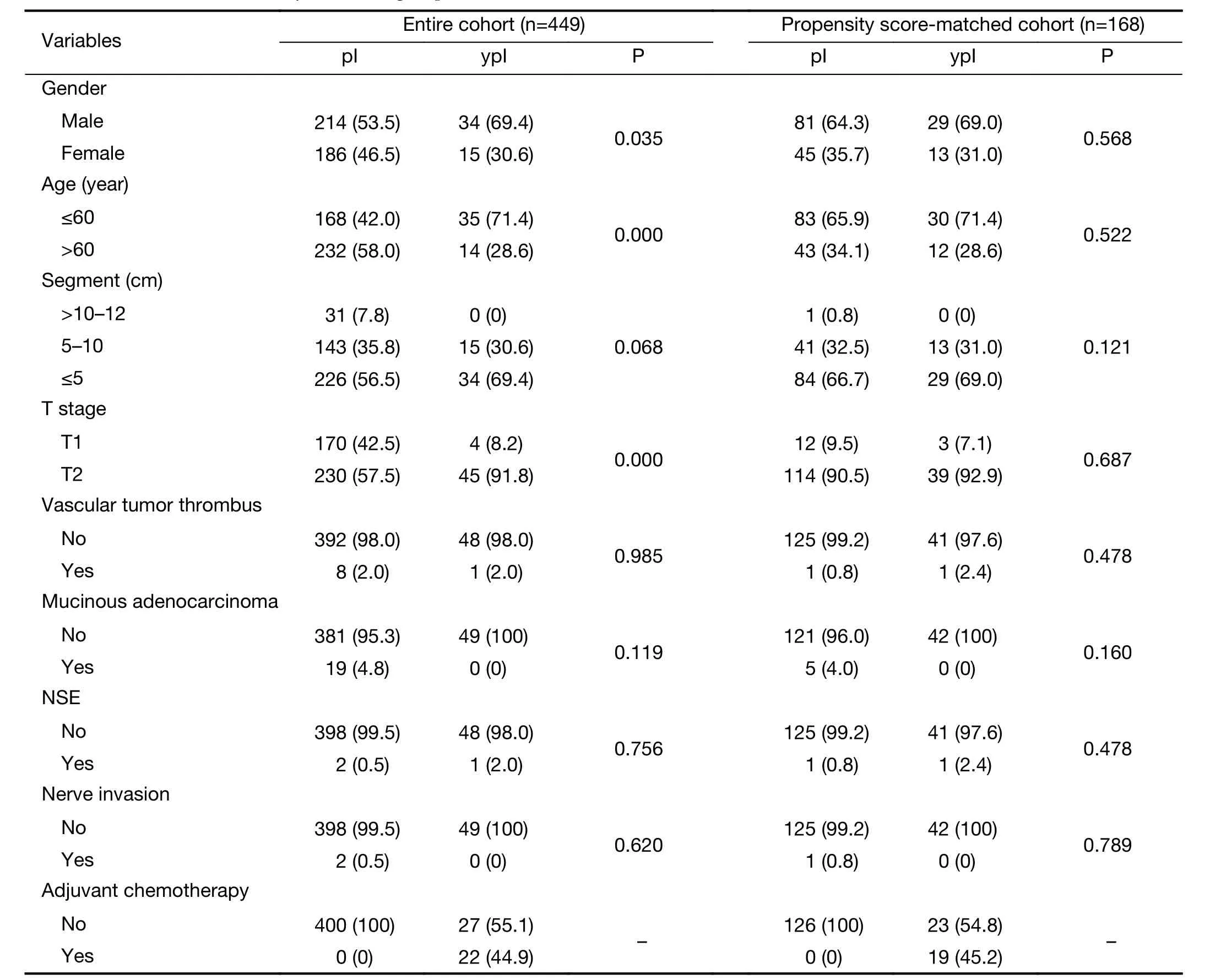
Table 2 Patient characteristics by treatment group before and after PSM
DDS favor cohort
In the ypI group, patients with DDS≥5 were selected and PSM was performed again according to sex, age and T stage. It resulted in 18 matched (ypI:pI=1:3) pairs, for a total of 72 patients. Patient and tumor characteristics were not significantly different between the two groups after PSM (Table 5). Of the DDS-favorable patients, there were 2, 13 and 3 with clinical stage IIIa, IIIb and IIIc,respectively. The 5-year clinical outcomes of ypI and pI groups in terms of LC (100% vs. 95.8%, P=0.384), DMFS(100% vs. 94.4%, P=0.368), DFS (100% vs. 92.2%,P=0.277) and OS (100% vs. 95.0%, P=0.458) were all similar.

Figure 1 Long-term outcomes of stage pI and ypI group after propensity score-matching. (A) DMFS, distant metastasis-free survival (P=0.025); (B) OS, overall survival (P=0.040); (C) DFS,disease-free survival (P=0.080); (D) LC, local regional control(P=0.796).
Discussion
The present study compared the long-term prognosis of ypI rectal cancer and early rectal cancer treated with de novo surgery that resulted in pI status. The data were derived from a prospective phase II study in our single center that safeguarded the study integrity and ensured adequate follow-up rate. The results showed that the prognosis of stage ypI rectal cancer was good, with 5-year DFS and OS rates reaching 85.9% and 95.7%, respectively.However, actuarial survival analysis after PSM indicated that the distant metastasis rate of ypI group at 5 years was 26.4%, which was significant higher than 7.3% of pI stage rectal cancer (P=0.025). In DDS subgroup analysis, ypI group patients with DDS score ≥5 achieved very good outcomes of LC, DMFS, DFS and OS, which were comparable with early stage pI rectal cancer.
Approximately 40%—60% LARC patients could achieve down-staging after neoadjuvant CRT, which translates into long-term favorable oncologic outcomes (3,6,7). Our previous study showed that stage yp0—I patients attained 96% OS, with low relapse rate of 7%. Although it is widely acknowledged that the postoperative pathologic stages using TNM terminologies between neoadjuvant (i.e. “yp”)and de novo (i.e. “p”) settings are different in terms of their respective clinical meanings (8-10), few studies have specifically compared outcome differences in early stage rectal cancer between post-CRT patients and those undergoing TME surgery. Several studies demonstrated that, in comparison with the patients in stage pI, those in ypI group had several risk factors for poor oncologic outcomes such as higher carcinoembryonic antigen (CEA)level, more advanced T stage, and poorer histological differentiation (11,12). However, the patients in ypI group did not exhibit a higher disease progression rate or cancerrelated death than those in pI group. Reerink et al. also showed that the prognoses for patients with initially unresectable rectal tumor down-staged to pT2 and those with primary resectable cancer with the same T classification are similar (9). In the study by Du et al.,patients with early-stage rectal cancer were selected to undergo radical surgery as a control group, and the results demonstrated that post-CRT early stage rectal cancer has no significant different in prognosis (13). Unlike previously reported results, the present study indicated that, although the prognosis of patients with ypI stage LARC was good,the probability of distant metastasis was higher than that of de novo early-stage rectal cancer. This observation camefrom PSM, a method which could help reduce the selection bias between two study cohorts, making the results closer to that of a randomized controlled study. It thus suggests that, in some cases LARC are still prone to distant metastasis even with high LC after neoadjuvant CRT.Therefore, how to screen for patients with rectal cancer of different biological behaviors based on molecular phenotypes or clinical features has become an avidlypursued research topic.

Table 3 Long-term outcome of stage pI and ypI group before and after PSM
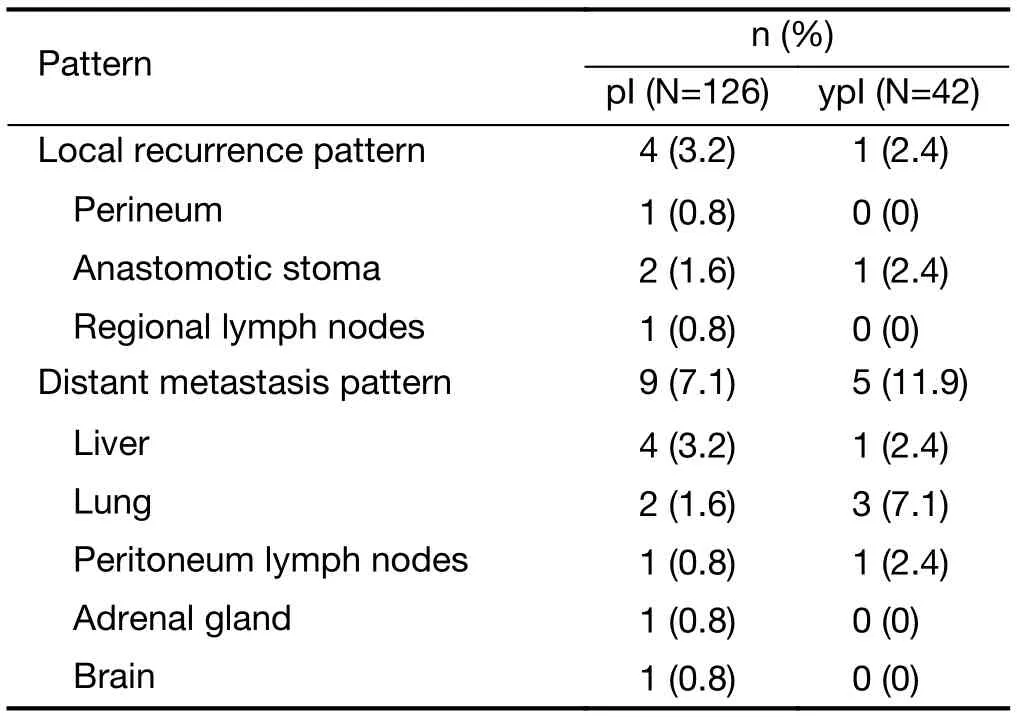
Table 4 Patterns of recurrence
In recent years, studies of metastatic colorectal cancer using cytotoxic chemotherapy and targeted agents have revealed that the depth of down-staging impacted prognosis, and parameters such as early tumor shrinkage(ETS) and depth of response (DpR) could effectively evaluate response and predict long-term survival (14-16).ETS was defined as tumor shrinkage of 10% to 30% or more at the first evaluation after treatment. DpR was defined as the percentage of tumor shrinkage when the lesion’s maximum diameter or volume reached the lowest value as compared to the baseline tumor size. Heinemann et al. assumed that DpR, which may be associated with specific anti-proliferative agents, as a clinical response evaluation index could predict PFS and OS and provide a basis for subsequent treatment strategy (17). de Campos-Lobato et al. found that down-staging did not significantly improve the LC, DFS and OS for stage cII rectal cancer,whereas it yielded good outcome in patients with stage cIII LARC. It thus suggested that the predictive value of downstaging for patients with more advanced pretreatment stage may be better (18). Neoadjuvant rectal (NAR) scoring system, reported in George’s literature, was based on three indicators: pre-treatment clinical T stage, postoperative pathologic T and N stage, and one by using the nomogram
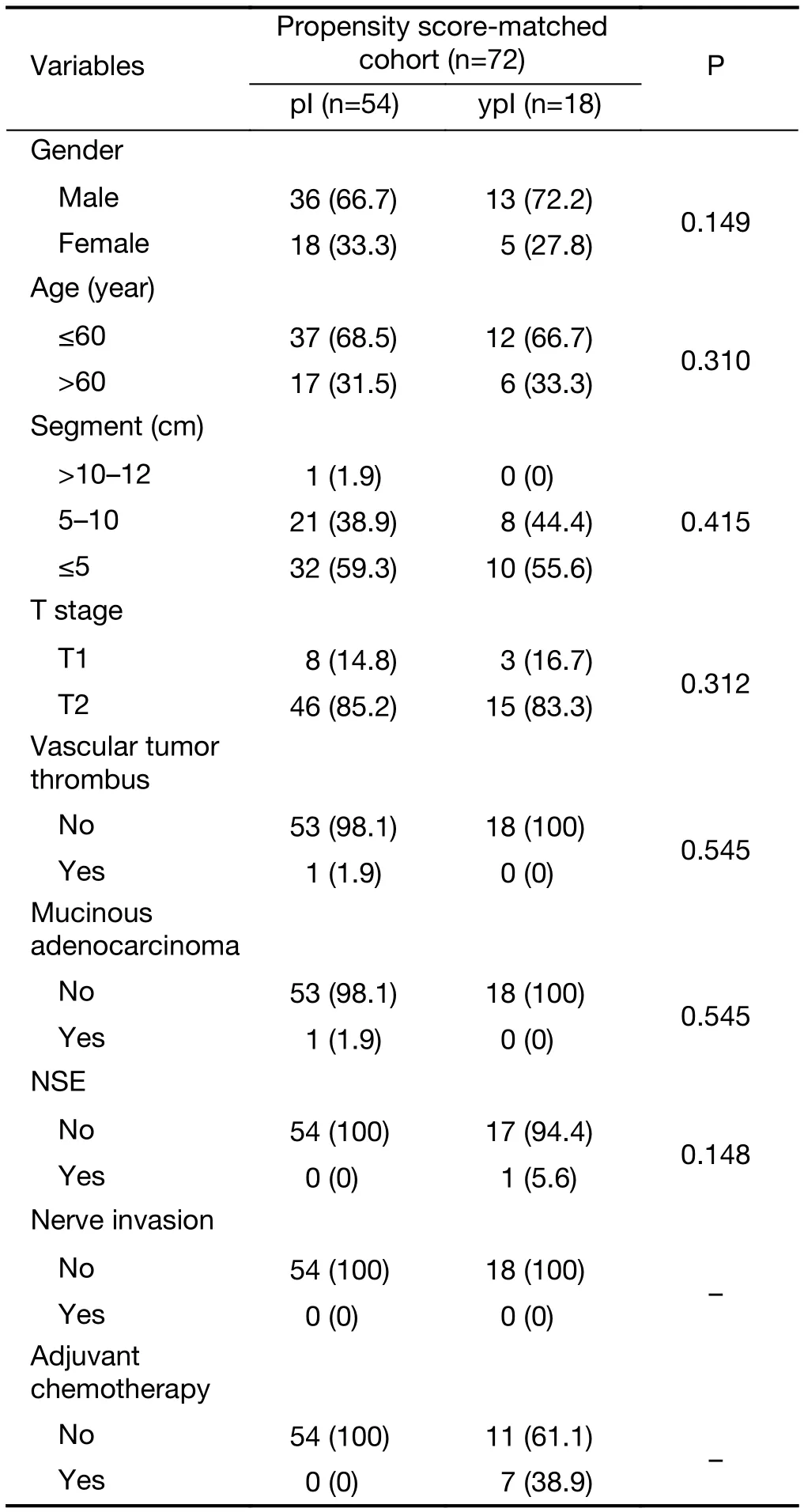
Table 5 DDS favorable patient characteristics after PSM
DDS, down-staging depth score; PSM, propensity score matching; NSE, neuron-specific enolase.formula published by Valentini (19,20). Several studies reported that the down-staging depth was associated with prognosis (19,21). It was used to analyze the results in NSABP R-04 study, with the conclusion that NAR could be used to predict OS (P<0.001) with relative ease.Therefore, the author illustrated that NAR could be a new effective prognostic factor, as well as pCR and tumor regression grade (TRG) classification. Our previous study concluded that DDS, an indicator of staging dynamic changes, was associated with DMFS, DFS and OS, and that the ability to predict prognosis was superior to pCR and TRG grades (5). In our study, DDS method is similar to the NAR scoring system, but is simpler to obtain, and the preoperative N-staging was considered. With the considerations of ETS, DpR, NAR and the results of this study, the changes of tumor extent at specific time points could provide more information about the lesion’s biological behavior and treatment sensitivity, thereby setting a new trend in evaluating response. Recent imaging studies have also focused on the evaluation of prognostic values based on dynamic changes of tumor dimensions(22,23). Therefore, predictive indicators based on response should take into account the overall depth of remission before and after treatment. Simply relying on qualitative evaluation of pre- or post-treatment tumor status may not be comprehensive or accurate enough to provide prognostication. The results of our study also found that DDS was an effective prognostic indicator, enabling accurate selection of patients with good long-term outcomes. The LC, DMFS, DFS and OS of DDS-favorable patients were comparable to those of early rectal cancer cohort.
The conclusion in this paper was derived from observation based on prospectively maintained database,and PSM method was used to compare two cohorts to reduce potential bias. The goal of the present study is to determine the prognostic parameters for LARC after neoadjuvant CRT in order to guide subsequent treatment strategy. The MERCURY study had shown good correlation between post-treatment MRI disease status and tumor histopathology, resulting in specific diagnostic guideline (24). MRI has an accuracy of 88% in staging rectal disease after neoadjuvant treatment, therefore could accurately determine the pathological regression extent and dictate the following surgical treatment, even accurately selecting cases suitable for watch-and-wait strategy based on results of the present study.
This study does have its limitations. Firstly, the number of patients was limited, especially in the neoadjuvant treatment group. As all cases were selected from a phase II database and the proportion of down-staging was not high,the number of stage ypI cohort was relatively small.Therefore, despite the use of PSM method, the restrictive number of cases might still affect the long-term survival and DDS analysis results. Secondly, we did not include the analysis of postoperative chemotherapy for LARC patients due to its inconsistent effects. Previous studies have reported that the value of chemotherapy after neoadjuvant CRT remains uncertain. PSM analysis from study of Park et al. concerning 1,016 ypT0—2N0 stage patients from 10 centers showed that adjuvant chemotherapy was not associated with improvement in 5-year RFS (P=0.62) (25).In addition, since all patients in pI group did not receive adjuvant chemotherapy, we did not take into account the influence of adjuvant chemotherapy when analyzing with PSM methodology.
Conclusions
Local control was comparable in both de novo pI stage cohort and LARC group achieving ypI stage. However,distant metastasis was more frequent in down-staged LARC patients as compared to early-stage cases. The overall prognosis of patients with sufficient down-staging of tumor extent was relatively good. Furthermore, the clinical stage after concurrent chemoradiation can achieve a high rate of correlation with postoperative pathology.Therefore, this study provides support for appropriate use of prognostic factors in patients with LARC in order to guide further treatment strategy after neoadjuvant chemoradiation.
Acknowledgements
This work is supported by Natural Science Foundation of China (No. 81773241); Chinese Academy of Medical Sciences Innovation Fund for Medical Sciences (No. 2017-I2M-1-006).
Footnote
Conflicts of Interest: The authors have no conflicts of interest to declare.
杂志排行

Chinese Journal of Cancer Research的其它文章
- Incidence and mortality of stomach cancer in China, 2014
- Incidence and mortality of laryngeal cancer in China, 2008–2012
- Effectiveness and safety of different amifostine regimens:Preliminary results of a phase II multicenter randomized controlled trial
- Combined peripheral natural killer cell and circulating tumor cell enumeration enhance prognostic efficiency in patients with metastatic triple-negative breast cancer
- Treatment patterns for adjuvant docetaxel-based chemotherapy in early-stage breast cancer in China: A pooled retrospective analysis of four observational studies
- Presence of circulating tumor cells is associated with metabolicrelated variables in postoperative patients with early-stage breast cancer