Laparoscopic adenomectomy in BPH-Does it have a role today?
2018-03-29RamalingamManickamSivasankaranNachimuthuSenthilKallappanMizarPai
Ramalingam Manickam*,Sivasankaran Nachimuthu,Senthil Kallappan,Mizar G.Pai
Uro-Nephro Centre,Ganga Medical Centre&Hospitals,Ramnagar,Coimbatore,India
1.Introduction
The initial management of symptomatic benign prostatic hyperplasia(BPH)worldwide is medical management.Most commonly practised procedure for benign prostatic enlargement(upto 75-80 g)refractory to medical therapy is transurethral resection of prostate(TURP)[1].There are many other options like holmium laser enucleation of prostate(HoLEP)[2]and laser vaporisation which are done regularly.Recently UroLift is also being attempted[3].For prostatic adenoma larger than 80 g TURP may be incomplete and hence sometimes done in two stages.Open prostatectomy is still widely practised in such situations[4].Another less commonly practised approach is laparoscopic adenomectomy[5].Rarely in high risk patients,prostatic stents[6]have been attempted.In this review,an attempt is made to discuss the different techniques of laparoscopic adenomectomy and to determine the role for this procedure today.
2.Surgical techniques
2.1.Laparoscopic millins adenomectomy
In this technique[5,7](Fig.1),the patient is placed in the supine position and a 12 mm incision is made just below the umbilicus.Extra-peritoneal space is opened up either with finger or using balloon trocar.Then a zero degree telescope is used to further develop and expand the extra peritoneal space laterally.Subsequently three more secondary ports are inserted namely two 5 mm ports midway between spino-umbilical line on either side for hand instruments;and a 10 mm port just above anterior superior iliac spine on the left side for introducing sutures or applying suction cannula.Landmarks like pubic symphysis,and inferior epigastric vessels are de fined.Using suction cannula and bipolar cautery or ultrasonic shears preprostatic fat is cleared.With L-hook diathermy or scissors transverse capsulotomy is made at least 1 cm below bladder neck for a length of 3-5 cm depending on the size of the prostate.Bleeders are controlled with bipolar cautery or ultrasonic shears.The plane between capsule and adenoma is identi fied and developed.The enucleation is facilitated by taking a vicryl suture through adenoma and pulling it cranially.Energy sources are not used close to apex as it may impair the continence.Instead sharp scissors are used to divide the distal attachments.The enucleated adenoma is placed aside.Further haemostasis is achieved using bipolar diathermy.Rarely trans fixation of bleeders at 5 and 7 o’clock position may be needed.An attempt of retrigonisation is done to facilitate reepithelisation and a 22 Fr or 24 Fr three-way Foley catheter is placed.The rent in the capsule is closed with 2-0 polyglactin suture.The bladder is filled with saline and if there is any leak,it is oversewn.Specimen is entrapped and retrieved by enlarging the lateral most port to 3-4 cm.A tube drain is inserted through one of the secondary ports.Ports are closed.Bladderirrigation may be started ifhaematuria is significant.
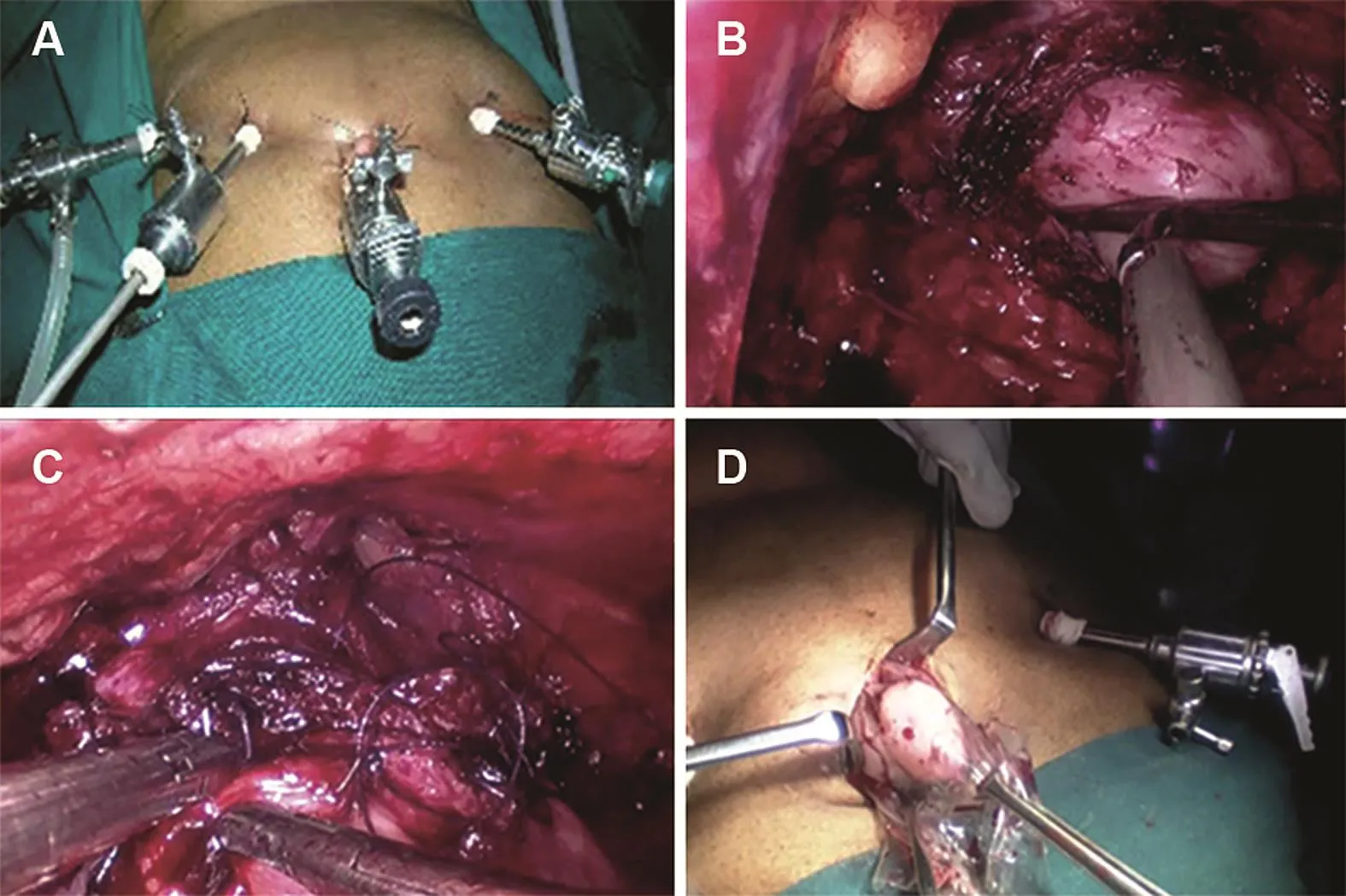
Figure 1 (A)Ports position for laparoscopic millins;(B)Transverse capsulotomy and enucleation of adenoma;(C)Capusulotomy closure with 2-0 polyglactin;(D)Entrapped specimen retrieved.
2.2.Extraperitoneal transvesical adenomectomy
In this technique[8],instead of transcapsular approach,transvesical approach of Freyer’s is followed.A 4 cm vertical cystotomy is made close to capsule.Mucosa overlying the adenoma is incised all around,and the plane between adenoma and capsule is developed.Using ultracision and suction cannula enucleation is continued.Meticulous haemostasis is secured using bipolar coagulation or ultracision.No energy source is used near the sphincter.Enucleated adenomas are placed aside.Persistent bleeders at bladder neck are trans fixed with 3-0 polydioxanone sutures,avoiding ureteral orifice.Retrigonisation is done whenever possible.A 22 size three-way Foley catheter is placed.Vesicotomy is closed with 2-0 polydiaxonone suture.Tube drain is placed and ports are closed.
2.3.Finger assisted laparoscopic retropubic prostatectomy
This techniqueisfacilitated by insertinga finger through one of the port sites or an additional port placed at suprapubic area[9,10].The digital enucleation is faster and complete.This is facilitated further by manipulation with rectal finger.Subsequently pneumoperitoneum is reestablished and capsule is closed with polyglactin suture and drain is placed.Haemostasis is secured and retrigonisation is done with absorbable suture to create a wide bladder neck.The specimen is removed by enlarging the suprapubic port.The wound is closed with polyglactin suture.
2.4.Mucosa preserving laparoscopic adenomectomy
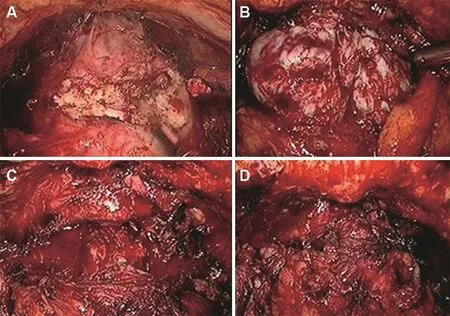
Figure 2 (A)Transverse incision was made below the base of prostate;(B)Bilateral lobes of adenoma;(C)Urethra demonstrated after adenoma removal;(D)Last stage of the procedure showing capsule.
In this technique(Fig.2),described by Yang et al.[11],the extra peritoneal space is developed using a balloon.Transverse capsulotomy is made and the plane between capsule and adenoma is developed on the anterior,lateral and posterior aspect using ultrasonic shears.Close to the urethra sharp scissors are used to separate urethra from adenoma.Moving the Foley catheter back and forth helps to de fine urethral mucosa and thus the adenoma alone is enucleated.Leaks are checked by filling the bladder with saline.Any rent in mucosa is closed with 3-0 polydiaxonone suture.Haemostasis is achieved by bipolar coagulation.A temporary gauze pack may be needed sometimes.
2.5.Robot assisted laparoscopic simple prostatectomy(RALSP)
Steep learning curves in laparoscopic simple prostatectomy(LSP)and availability of Da Vinci system have made robotic surgeons to attempt robot assisted LSP[12,13].In this technique,patient is placed in steep trendelenburg position and four robotic arms are inserted.Additional two ports are inserted for assistance.The bladder is dropped and Retzius space is entered and anterior surface of prostatic capsule is de fined.A horizontal cystotomy incision was made proximal to the junction of the bladder and prostate.Transvesical enucleation of the adenoma is carried out facilitated by a suture placed through the adenoma for traction.The steps are similar to the procedure described in the extra peritoneal transvesical adenomectomy.
2.6.Laparo endoscopic single site(LESS)prostatic adenomectomy
In this extraperitoneal transvesical approach[14],a single port with provision for three trocars(Triport™)is placed at subumbilical level through a 3 cm incision of skin,rectus and bladder so as to snugly fit.Bent hand instruments and flexible digital telescope are used to enucleate prostate.This is suitable when there is a large median lobe.As this is technically demanding and expensive,only a very few centres practise this procedure.
In all the above techniques,bladder irrigation is started after the surgery and is continued till urine clears.Drain tube is removed on second or third post-operative day and Foley catheter is removed around the fifth day.
3.Complications
Martı´n Garzo´n et al.[15]reported a overall complication rate of 14.6%in both LSP and RALSP.Urinary tract infection occurred in 3.6%of cases of LSP and 10.6%of cases of RALSP;urethral meatal stenosis occurred in 2.4%of cases of LSP;new onset overactive detrusor occurred in 4.8%of cases of LSP;and acute urinary retention occurred in 2.4%of cases of LSP.In the group of patients who underwent RALSP,anterior urethral stricture occurred in 1.3%of cases;ileus and urinoma occurred in 1.3%of patients.
In an European American multi-institutional study,Autorino et al.[16]reported intraoperative grade 1 complication of 0.5%in LSP and 2.2%in RALSP;grade 2 complication of 1.2%in LSP and 1.7%in RALSP among a total of 1330 cases(LSP 843 and RALSP 487 cases).The group also reported that the 90-day postoperative complication rate was 7.1%in LSP and 16.6%in RALSP.Among this the grade 1 complications were 5%in LSP and 6.5%in RALSP.This included urinary retention,ileus,hematuria with clots,erectile dysfunction and urge incontinence.Grade 2 complications were 0.6%in LSP and 8%in RALSP.This included urinary tract infection,anemia,wound infection,deep vein thrombosis and others.Grade 3 complications were 0.6%in LSP and 2%in RALSP.This included urethral or bladder neck stricture,hematuria or clots,urinary fistula,wound infection,Weck clip migration and bleeding.Grade 4 complications were none in LSP and 0.2%in RALSP.Grade 5 complications were none in LSP and 0.2%in RALSP.
Desai et al.[14]published an observation study of 39 patients with an average weight of 103 g prostate wherein the mean operative time of 116 min and blood loss around 500 mL were recorded.They also claim finger enucleation can be done when there is technical difficulty or undue bleeding.
4.Discussion
TURP remains the gold standard for symptomatic BPH up to 80 g.However,in gland larger than 100 g,TURP is fraught with longer operative times and higher morbidity[20].To overcome the morbidity and reduce complications,bipolar TURP,HoLEP and LSP are being practised[21-23].Very few centres practice single port laparoscopic adenomectomy or robot assisted laparoscopic adenomectomy[13].
In the author’s experience over 26 years of managing BPH,2460 patients underwent TURP;240 patients underwent open simple prostatectomy;seven patients underwent HoLEP and five patients underwent LSP.The results were comparable with the other series as mentioned in the Table 1.
In a meta-analysis of 27 observational studies of 764 patients[19],a comparison of the outcomes of LSP with open simple prostatectomy(OSP)was made.It was concluded that the outcomes and postoperative complications were similar;but the bene fit in LSP was lesser hospital stay(1.6 days),shorter catheterisation time(1.3 days)and lesser blood loss(187 mL).Lesser blood loss was attributed to using bipolar or ultracision energy during enucleationin LSP.They concluded LSP is an effective,safe alternative approach for surgery of larger BPH.
In the multicentre study[16]of 1330 surgeries done from 2000 to 2014,a comparison was made between 843 cases of LSP with 487 cases of RALSP.The study revealed that for a comparable median size of 76 g prostate;the operative time for LSP(95 min)was shorter than RALSP(154.5 min).Blood loss was less with LSP compared to RALSP.Twelve months postoperative Qmaxwas 25 mL/s in both groups.The International Prostate Symptom Score(IPSS)was 7 in RALSP as against 5 in LSP.The postoperative complications were comparable(16.6%)in both groups.
In another multicentre study,17.7%of patients who had RALSP and 5.3%of patients who had LSP had complications[17].However,the trend of the laparoscopic approach shows increasing numbers of RALSP in last few years in spite of increased rate of complications in RALSP.
Further prospective randomized trials are needed to evaluate the cost versus bene fit in switching over to RALSP.
The limitations of LSP are previous pelvic surgery and known bleeding diathesis in which case HoLEP is preferable[7].Also,only experienced laparoscopic surgeon can perform LSP with a favourable outcome[24].

Table 1 Outcomes of laparoscopic simple prostatectomy.
Al-Aown et al.[18]in their study of 11 patients of LSP noted that in one of the patients who had undergone inguinal herniorrhaphy,there was difficulty in adhesiolysis.This lead to incomplete removal of adenoma and prolonged operative time.In such difficult situation,good coordination of assistant surgeon will greatly help to complete LSP.In very large adenomas enucleation can be facilitated by taking a suture through adenoma to retract.They conclude LSP is feasible and safe alternative to OSP in the hands of experienced laparoscopic surgeons.
McCullough et al.[25]in their study of 280 patients from 2003 to 2008 compared 96 LSPs with 54 OSPs and concluded that LSP takes longer time(95 min vs.54 min);but catheter time and hospital stay was lesser by 1 day and hence advantageous.
5.Conclusion
When the prostatic adenoma is larger than 80 g;OSP is still widely practised inspite of being more morbid.Alternative techniques like HoLEP and LSP are practised less commonly due to their steep learning curve.It looks like LSP has a place in symptomatic,larger prostatic adenoma in the hands of experienced laparoscopic surgeons.
Conflicts of interest
The authors declare no conflict of interest.
[1]Iglesias JJ,Perez-Castro EE,Massuri SD,Sporer A,Seebode JJ.Hydraulic hemostasis in transurethral resection of the prostate using the Iglesias continuous suction resectoscope.J Urol 1977;117:306-8.
[2]Gilling PJ,Kennett K,Das AK,Thompson D,Fraundorfer MR.Holmium laser enucleation of the prostate(HoLEP)combined with transurethral tissue morcellation:an update on the early clinical experience.J Endourol 1998;12:457-9.
[3]Sønksen J,Barber NJ,Speakman MJ,Berges R,Wetterauer U,Greene D,et al.Prospective,randomized,multinational study of prostatic urethral lift versus transurethral resection of the prostate:12-month results from the BPH6 study.Eur Urol 2015;68:643-52.
[4]Millin T,Dubl MC.Retropubic prostatectomy:A new extravesical technique report on 20 cases.J Urol 2002;167:976-9.
[5]Mariano MB, Te filliMV, Graziottin TM, Morales CM,Goldraich IH.Laparoscopic prostatectomy for benign prostatic hyperplasia-a six-year experience.Eur Urol 2006;49:127-31;discussion 131-2.
[6]Corica AP,Larson BT,Sagaz A,Corica AG,Larson TR.A novel temporary prostatic stent for the relief of prostatic urethral obstruction.BJU Int 2004;93:346-8.
[7]Van Velthoven R,PeltierA,Laguna MP,Piechaud T,Guillonneau B.Laparoscopic extraperitoneal adenomectomy(millin):pilot study on feasibility.Eur Urol 2004;45:103-9.
[8]Rehman J,Khan SA,Sukkarieh T,Chughtai B,Waltzer WC.Extraperitoneal laparoscopic prostatectomy(adenomectomy)for obstructing benign prostatic hyperplasia:transvesical and transcapsular(millin)techniques.J Endourol 2005;19:491-6.
[9]Hoepffner JL,Gaston R,Piechaud T,Rey D,Mugnier C,Njinou B,et al.Finger assisted laparoscopic retropubic prostatectomy(millin).Eur Urol Suppl 2006;5:962-7.
[10]Chlosta PL,Varkarakis IM,Drewa T,Dobruch J,Jaskulski J,Antoniewicz AA,et al.Extraperitoneal laparoscopic millin prostatectomyusing fingerenucleation.JUrol2011;186:873-6.
[11]Yang FY,Xing NZ,Wang JW,Zhang JH,Guo YL.[Retropublic extraperitoneallaparoscopicprostatectomywith urethra preservation].Beijing Da Xue Xue Bao Yi Xue Ban 2010;18:42;469-72.[Article in Chinese].
[12]Leslie S,Abreu AL,Chopra S,Ramos P,Park D,Berger AK,et al.Transvesical robotic simple prostatectomy:initial clinical experience.Eur Urol 2014;66:321-9.
[13]Sotelo R,Clavijo R,Carmona O,Garcia A,Banda E,Miranda M,et al.Robotic simple prostatectomy.J Urol 2008;179:513-5.
[14]Desai MM,Fareed K,Berger AK,Astigueta JC,Irwin BH,Aron M,et al.Single-port transvesical enucleation of the prostate:a clinical report of 34 cases.BJU Int 2010;105:1296-300.
[15]Martı´n Garzo´n OD,Azhar RA,Brunacci L,Ramirez-Troche NE,Medina Navarro L,Herna´ndez LC,et al.One-year outcome comparison of laparoscopic,robotic,and robotic intrafascial simple prostatectomy for benign prostatic hyperplasia.J Endourol 2016;30:312-8.
[16]Autorino R,Zargar H,Mariano MB,Sanchez-Salas R,Sotelo RJ,Chlosta PL,et al.Perioperative outcomes of robotic and laparoscopic simple prostatectomy:a European-American multi-institutional analysis.Eur Urol 2015;68:86-94.
[17]Pavan N,Zargar H,Sanchez-Salas R,Castillo O,Celia A,Gallo G,et al.Robot-assisted versus standard laparoscopy for simple prostatectomy:multicenter comparative outcomes.Urology 2016;91:104-10.
[18]Al-Aown A,Liatsikos E,Panagopoulos V,Kyriazis I,Kallidonis P,Georgiopoulos I,et al.Laparoscopic simple prostatectomy:a reasonable option for large prostatic adenomas.Urol Ann 2015;7:297-302.
[19]Lucca I,Shariat SF,Hofbauer SL,Klatte T.Outcomes of minimally invasive simple prostatectomy for benign prostatic hyperplasia:a systematic review and meta-analysis.World J Urol 2015;33:563-70.
[20]Mebust WK,Holtgrewe HL,Cockett AT,Peters PC.Transurethral prostatectomy:immediate and postoperative complications.A cooperative study of 13 participating institutions evaluating 3,885 patients.J Urol 1989;141:243-7.
[21]Porpiglia F,Terrone C,Renard J,Grande S,Musso F,Cossu M,et al.Transcapsular adenomectomy(millin):a comparative study,extraperitoneal laparoscopy versus open surgery.Eur Urol 2006;49:120-6.
[22]Sotelo R,Spaliviero M,Garcia-Segui A,Hasan W,Novoa J,Desai MM,et al.Laparoscopic retropubic simple prostatectomy.J Urol 2005;173:757-60.
[23]Yun HK,Kwon JB,Cho SR,Kim JS.Early experience with laparoscopic retropubic simple prostatectomy in patients with voluminous Benign Prostatic Hyperplasia(BPH).Korean J Urol 2010;51:323-9.
[24]Castillo O,Bolufer E,Lo´pez-Fontana G,Sa´nchez-Salas R,Fonero´n,Vidal-Mora I,et al.Laparoscopic simple prostatectomy(adenomectomy):experience in 59 consecutive patients.Actas Urol Esp 2011;35:434-7[Article in Spanish].
[25]McCullough TC,Heldwein FL,Soon SJ,Galiano M,Barret E,Cathelineau X,et al.Laparoscopic versus open simple prostatectomy:an evaluation of morbidity.J Endourol 2009;23:129-33.
杂志排行
Asian Journal of Urology的其它文章
- Bipolar transurethral enucleation and resection of the prostate:Whether it is ready to supersede TURP?
- Innovative endoscopic enucleations of the prostate-Xie’s Prostate Enucleations
- Non-invasive evaluation of lower urinary tract symptoms(LUTS)in men
- Botulinum toxin and benign prostatic hyperplasia
- The use of 5-alpha reductase inhibitors in the treatment of benign prostatic hyperplasia
- Update on minimally invasive surgery and benign prostatic hyperplasia