Falls from height: A retrospective analysis
2018-03-17KasimTurgutMehmetEdizSarihanCemilColakTanervenAlikrrb
Kasim Turgut, Mehmet Ediz Sarihan, Cemil Colak, Taner Güven, Ali Gür, Sükrü Gürbüz
1 Department of Emergency Medicine, Education and Research Hospital, Adiyaman University, Adiyaman, Turkey
2 Department of Emergency Medicine, School of Medicine, Inonu University, Malatya, Turkey
3 Department of Biostatistics and Medical Informatics, School of Medicine, Inonu University, Malatya, Turkey
INTRODUCTION
Falls are the second most common cause of injury associated mortality after traffic accidents. They comprise a significant percentage of blunt trauma cases and emergency department (ED) admissions.[1]A fall is defined as an injury to a person that occurs after landing on the ground after falling from a higher place, such as a ladder, scaffold, building, roof, or other elevated place or work area.[2]Falls mostly affect males, and disproportionately affect the very young or very old.They cause more deaths in old people than in children.[3]Many factors affect the mortality and morbidity of falls, such as patient age, fall height, cause of fall, type of ground on which the patient fell, and body parts injured.[4]This study aimed to analyze the demographic characteristics of falls from height and their effects on morbidity and mortality.
METHODS
The study was approved by the Inonu University Ethics Committee (No: 2014/154). We retrospectively enrolled 460 patients of all ages presenting to the Inonu University Emergency Service between November 2011 and November 2014 with a history of falls from height. Patients with incomplete or missing data or those with trauma from simple falls were excluded. The patients were divided in two groups: those who died and survivors. The patient data were recorded on standard forms, which included the following parameters: age,gender, vital signs, cause of fall, fall height, fall location,type of ground on which the patient fell, season, time of day fall occurred, injured body part, and trauma scores[Revised Trauma Score (RTS), Circulation, Respiration,Abdomen, Motor, Speech (CRAMS), Abbreviated Injury Scale (AIS), Injury Severity Score (ISS), New Injury Severity Score (NISS), Trauma and Injury Severity Score (TRISS), Glasgow Coma Score (GCS)] on hospitalization and discharge.
Statistical analysis
The data were analyzed with IBM SPSS, ver. 22.00. The Shapiro-Wilk test was used to examine the fit of quantitative values to a normal distribution. The Mann-WhitneyU-test and Kruskal-Wallis test were used for statistical analysis.Multiple comparisons were done with the Conover-Imam test. Yates’, Pearson’s, and Fischer’s chi-square tests were used for qualitative values. Continuous variables are presented as the mean±standard deviation (SD). AP-value<0.05 was considered statistically significant.
RESULTS
During the 3-year study period, 460 patients [292(63.5%) men, 168 (36.5%) women; mean age 27±24.99(range 1–88) years] were admitted to the ED after falling from a height. The overall mortality rate was 5.6% (26)and it was 6.9% for men and 3.6% for women. The highest number of casualties was in the 0–5-year age group (28.3%) followed by the 6–15-year age group(18.5%). Patients in all age groups died and the ≥62-year age group had the greatest number of deceased, 15 patients. There was a significant relationship between mortality and the 0–5- and ≥62-year age groups (P<0.05).The greatest number of falls was from 1.1–4 meters (m)(46.1%). The relationship between mortality and fall height was significant at 0–1, 4.1–9, and >9 m (P<0.001).The patients fell mostly on solid ground (83.7%), but the outcomes of patients falling on solid versus soft ground did not differ significantly (P>0.05). Of the falls, 92.2%were unintentional, 8.1% were workplace accidents,and 1.7% were related to suicide. The highest mortality rate was in the suicide group (12.5%). The causalities mostly fell from balconies, stairs, and domestic furniture in decreasing order. The highest mortality rate was in the group falling from balconies (30.8%). There was a significant relation between mortality and place of fall(P<0.05). Most falls were from 12:01 to 18:00 o’clock and the highest number of deaths occurred in the same period (Table 1). Most falls were in June or July (15.6% and 15.6%, respectively). Half of the patients were treated in the ED and discharged, while 27.8% were hospitalized in the neurosurgery service and 15.4% in the orthopedics service.
Skin and soft tissue injuries were the most common traumatic lesions (37.4%). In the head injury group,linear fracture and subarachnoid hemorrhage had significant (P<0.05) effects on mortality. The most common thoracic injury was rib fracture (56.5%). The least common lesions involved the abdomen and pelvis.Upper extremity injuries were more common than lower extremity injuries. Abdominopelvic, thoracic, and extremity injuries had no significant effect on mortality.The most deadly spinal fractures were cervical fractures(33.3%). Spinal fractures had a significant (P<0.001)effect on mortality (Table 2). There were significant(P<0.05) relationships between fall height and the trauma scores. As fall height increased, AIS, ISS, and NISS increased, while GCS, RTS, CRAMS, and TRISS decreased (Table 3). All of the trauma scores (GCS, AIS,RTS, ISS, NISS, TRISS, and CRAMS) had significant(P<0.05) effects on mortality (Table 4).
DISCUSSION
Falls from height are a common cause of blunt trauma.[1]Age, fall height, cause of fall, ground typestruck, injured body part, and organ injuries are the main factors that affect the morbidity and mortality of falls from height.[5,6]In agreement with the literature,we found that age, fall height, fall location, head injury,linear skull fracture, subarachnoid hemorrhage, cervical fracture, thoracic vertebra fracture, and GCS, AIS, ISS,NISS, RTS, TRISS, and CRAMS had significant effects on mortality.
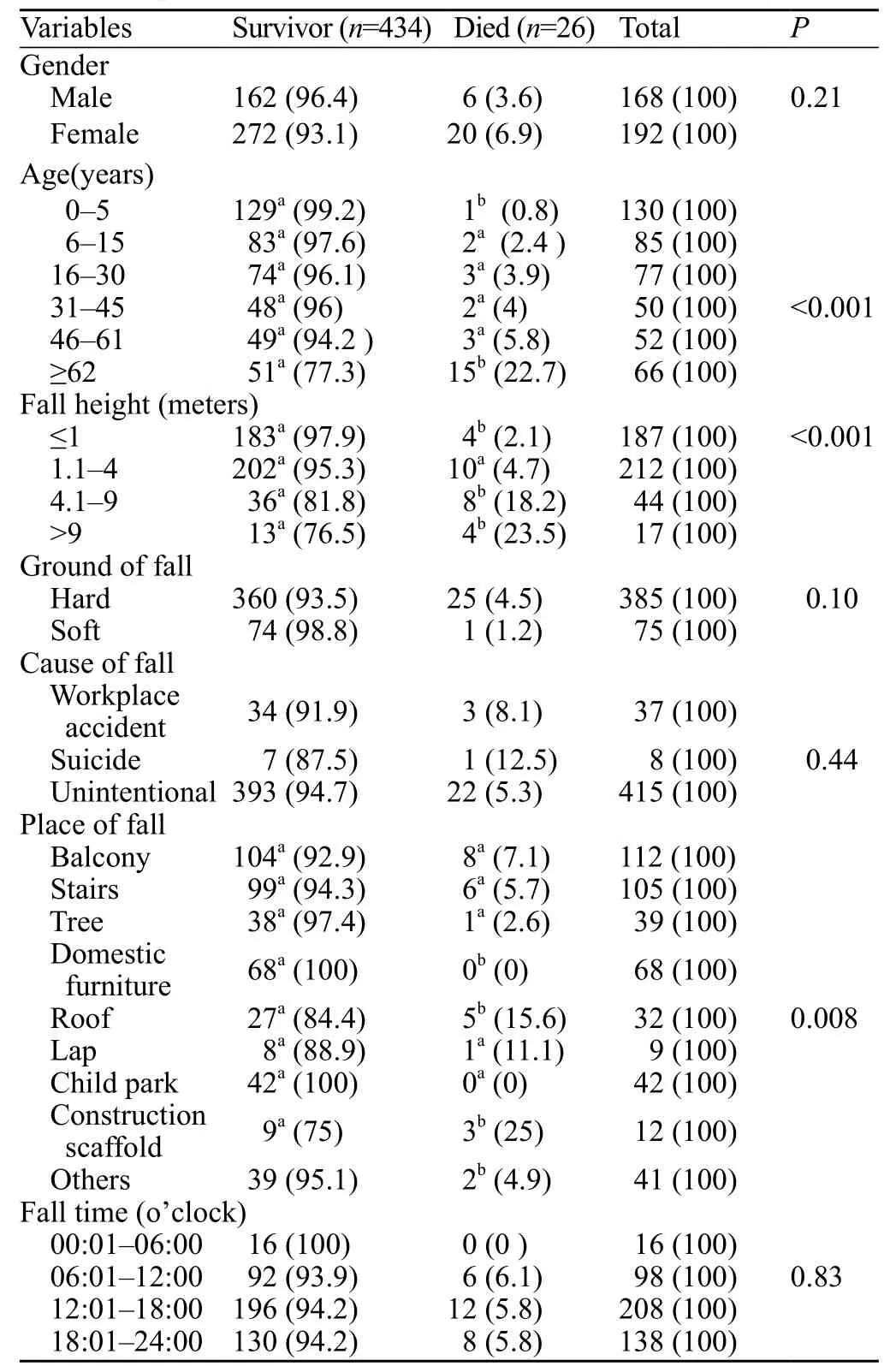
Table 1. Population characteristics associated with fall from height (n, %)
In this study, the majority of falls involved males(63.5%), in agreement with the literature.[5,7-9]Generally,men are exposed to trauma and falls more often than women because boys are more active than girls at earlyages and more men are physical laborers than women.The highest number of falls in our study was in the 0–5-year group (28.3%). In other studies, the greatest number was in the 0–4- and 0–10-year groups.[9,10]The high number of falls in these age groups is related to the very active nature of children and lack of protection. Overall,74.3% of the patients were ≤45 years old, indicating that people of active ages are more frequently involved in trauma. Older individuals, especially those over 60 years old, lose their ability to balance, which causes more falls.[11]According to the National Trauma Data Bank, falls are the most common cause of death at older ages.[12]İcer et al[5]found that the highest proportion of deaths (19.2%)from falls was in individuals ≥55 years old. In our study,it was in individuals over 61 years old and the mean age of all deaths was 55.27±26.46 years.

Table 2. Distribution of injuries sustained (n, %)
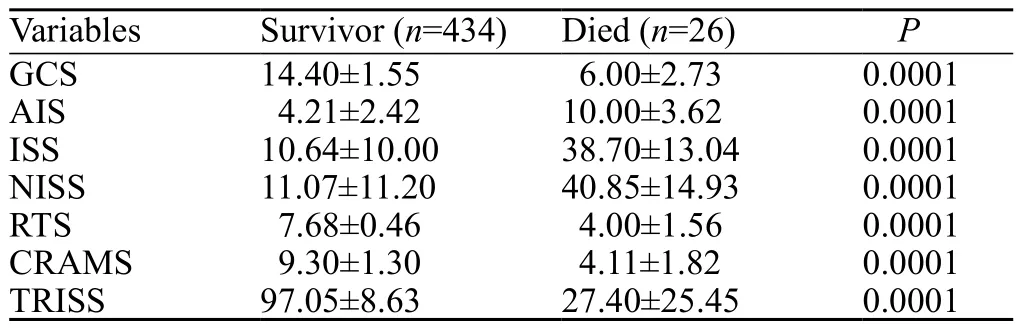
Table 4. Trauma scores of survivor and died patient
Generally, the mortality rate is greater with falls from higher places compared with lower places.[5]The reported mortality rates of falls from ≥12 meters and ≥18 meters were 50% and 100%, respectively.[13]However,a survivor who fell from 19 stories (57 meters) has also been reported.[14]Liu et al[15]found that the mortality rate due to falls from >6 meters was 22.7% and while Velmohos et al[16]found that it was 9.6% for falls from>9 meters. In our series, the mortality rate from falls from >9 meters was 23.5%, which is compatible with the literature. Al et al[17]found that the mean fall height was 3.2±2.4 meters and Yagmur et al[18]found that it was 4.5±2.6 meters. In our series, the mean fall height was 2.51±3.7 meters for all patients and 6.79±9.87 meters for those who died.
The main causes of falls from height are suicide,workplace accidents, and unintentional accidents.[11]In our series, 90.2% of the falls resulted from unintentional accidents. In an Indian study, falls from height comprised the highest number of deaths among workplace accidents and the majority of these falls were from construction sites.[19]In our series, 8.1% of the workplace accidents were falls and 32.4% of them were from constructionsites. In the construction sector and other workplaces,sufficient measures must be taken to prevent falls,competent workers should be employed, and adequate training must be given to reduce the number of workplace accidents.

Table 3. The relation between trauma scores and fall height
In many studies of falls, the greatest number of falls occurred in summer.[3,9,20,21]In our series, 45.9% of the falls and 30.8% of the deaths occurred during summer. Al et al[17]and Gulatı et al[3]found that the highest number of falls occurred from 00:00 to 06:00 o’clock. That was because people sleep on rooftops in summer because of the warm weather in the regions where those studies were conducted. The weather in our region is cool in the summer and people do not sleep on the rooftops.In our series, the majority of falls and deaths occurred from 12:01 to 18:00 o’clock (46.1%), which coincides with the active work hours. In descending order, the patients in our series underwent definitive treatment in the emergency, neurosurgery, orthopedics, and general surgery departments. Other studies of falls obtained similar results, i.e., the majority of falls were treated in the emergency department.[1,9]
In falls from height, the first body part that hits the ground and the lesions resulting from fall impact affect the morbidity and mortality. The majority of injuries are to the skin and subcutaneous tissues and head.[5,7,9,17]In our series, similar to the literature, skin and subcutaneous tissue (37.4%) and head (25.4%) injuries were most frequent. Of those who died, 73.1%[19]had head injuries and 50% also had subarachnoid hemorrhages.
We calculated the trauma scores of those who died and the survivors. The results accorded with the literature and there were significant relationships between mortality and the trauma scores.[5,17,22]There were also significant relationships between the trauma scores and fall height.
In the present study, we evaluated the mortality factors of patients that admitted to hospital. We determined brain injury as the main cause of death.But, the majority of traumatic deaths occurred in prehospital setting; on-scene or during transport and the leading cause of death is polytrauma.[23]The incidence of prehospital mortality is great among overall trauma related deaths. So, prehospital medicine and trauma prevention programs are significant factors to reduce traumatic deaths.[24]All countries should take measures for prehospital medicine and physician based rescue systems may reduce traumatic deaths.
In this study, the data on the falls were obtained from the patients or their relatives. Consequently, the fall heights of some patients might be inaccurate. We collected data from the hospital records of the ED doctors. These records often lack data because the ED doctors have limited time to complete their charts. Therefore, we were obliged to exclude many patients. Neither of these limitations can be avoided easily.
CONCLUSION
In conclusion, age, fall height, fall location, head and spinal system injuries, and trauma scores related to mortality. The main causes of death were subarachnoid hemorrhage and subdural hematoma. The emergency services have an important role in treating victims of falls from height and other forms of trauma. Consequently,emergency services staff should be trained to use a systematic approach to trauma patients. Triage must be done accurately at the accident location and critical patients should be referred to trauma centers quickly.This should reduce the mortality and morbidity due to falls from height.
Funding:None.
Ethical approval:The study was approved by the Inonu University Ethics Committee (No: 2014/154).
Conflicts of interest:No any benefits have been received from a commercial party related directly or indirectly to the study.
Contributors:KT proposed the study and wrote the first draft. All authors read and approved the final version of the paper.
1 Ersoy S, Sonmez BM, Yilmaz F, Kavalci C, Ozturk D,Altinbilek E, et al. Analysis and injury paterns of walnut tree falls in central anatolia of turkey. World J Emerg Surg.2014;9:42.
2 WorkSafeBC’s 2013 Annual Report. 2013 Statistics Serving British Columbians. Available from: https://www.worksafebc.com/en/search#q=2013%20 report&sort=relevancy&f:language-facet=[English]
3 Gulatı D, Aggarwal AN, Kumar S, Agarwal A. Skeletal injuries following unintentional fall from height. Ulus Travma Acil Cerrahi Derg. 2012;18(2):141-6.
4 Oguztürk H, Turgut K, Turtay MG, Sarihan ME, Gur A,Beydilli I, et al. Apricot tree falls: a study from Malatya,Turkey. Biomedical Research. 2016; 27(1):210-3.
5 İcer M, Güloglu C, Orak M, Ustundag M. Factors affecting mortality caused by falls from height. Ulus Travma Acil Cerrahi Derg. 2013;19(6):529-35.
6 Guneytepe UI, Aydin SA, Gokgoz S, Ozguc H, Ocakoglu G, Aktas H. Factors affecting mortality and scoring systems in geriatric trauma patients. Uludag Medical Journal. 2008;34:15-9.
7 Jain V, Jain S, Dhaon BK. A multi factorial analysis of the epidemiology of injuries from falls from heights. Int J Crit Illn Inj Sci. 2014;4(4):283-7.
8 Guzel A, Karasalihoglu S, Kucukugurluoglu Y. Evaluation of patients applied to pediatric emergency department due to falls. Turkish Journal of Trauma and Emergency Surgery.2007;13:211-6.
9 Yavuz M, Tomruk O, Baydar C, Kupeli A. Evaluation of accidental fall from high cases who admitted to emergency service. Journal of Forensic Medicine. 2004;18:8-12.
10 Pressley JC, Barlow B. Child and adolescent injury as a result of falls from buildings and structures. Inj Prev. 2005;11(5):267-73.
11 Eren A, Arslan M, Hilal A, Cekin N. Deaths due to fall from a height in Adana. Adli Tıp Bülteni. 2009;14:12-5.
12 Southerland LT, Stephens JA, Robinson S, Falk J, Phieffer L, Rosenthal JA, et al. Head trauma from falling increases subsequent emergency department visits more than other fall-related injuries in older adults. J Am Geriatr Soc.2016;64(4):870-4.
13 Buckman RF, Buckman PD. Vertical deceleration trauma.Principles of management. Surg Clin North Am. 1991;71(2):331-44.
14 Lee BS, Eachempati SR, Bacchetta MD, Levine MR, Barie PS. Survival after a documented 19-story fall: a case report. J Trauma. 2003;55(5):869-72.
15 Liu CC, Wang CY, Shih HC, Wen YS, Wu JJ, Huang CI, et al.Prognostic factors for mortality following falls from height.Injury. 2009;40(6):595-7.
16 Velmahos GC, Demetriades D, Theodorou D, Cornwell EE 3rd,Belzberg H, Asensio J, et al. Patterns of injury in victims of urban free falls. World J Surg. 1997;21(8):816-20; discussion 820-1.
17 Al B, Yıldırım C, Coban S. Falls from heights in and around the city of Batman. Ulus Travma Acil Cerrahi Derg.2009;15(2):141-7.
18 Yagmur Y, Guloglu C, Aldemir M, Orak M. Falls from flatroofed houses: a surgical experience of 1,643 patients.Injury. 2004;35(4):425-8.
19 Kohli A, Banerjee KK. Pattern of injuries in fatal falls from buildings. Med Sci Law. 2006;46(4):335-41.
20 Zahavi A, Luckman J, Yassur I, Michowiz S, Goldenberg-Cohen N. Severe cranial neuropathies caused by falls from heights in children. Graefes Arch Clin Exp Ophthalmol.2016;254(4):765-72.
21 Shields BJ, Burkett E, Smith GA. Epidemiology of balcony fall-related injuries, United States, 1990-2006. Am J Emerg Med. 2011;29(2):174-80.
22 Eryilmaz M, Durusu M. Fall from heights among adults.Meandros Medical and Dental Journal. 2008; 9:29-32.
23 Kleber C, Giesecke MT, Tsokos M, Haas NP, Schaser KD,Stefan P, et al. Overall distribution of trauma-related deaths in Berlin 2010: advancement or stagnation of German trauma management? World J Surg. 2012;36(9):2125-30.
24 Kleber C, Giesecke MT, Tsokos M, Haas NP, Buschmann CT. Trauma-related preventable deaths in Berlin 2010: need to change prehospital management strategies and trauma management education. World J Surg. 2013;37(5):1154-61.
杂志排行

World journal of emergency medicine的其它文章
- Perceptions of emergency medicine residents on the quality of residency training in the United States and Saudi Arabia
- Intravenous fluid selection rationales in acute clinical management
- Association between the elderly frequent attender to the emergency department and 30-day mortality: A retrospective study over 10 years
- Differential diagnoses of magnetic resonance imaging for suspected acute appendicitis in pregnant patients
- Ultrasound curriculum taught byfirst-year medical students: A four-year experience in Tanzania
- Prognostic value of cortisol and thyroid function tests in poisoned patients admitted to toxicology ICU