规范化疼痛管理模式在老年髋部骨折手术患者中的应用效果①
2017-08-01赵克聪孙海燕范静宇张宝翠杨威刘克敏
赵克聪,孙海燕,范静宇,张宝翠,杨威,刘克敏
规范化疼痛管理模式在老年髋部骨折手术患者中的应用效果①
赵克聪,孙海燕,范静宇,张宝翠,杨威,刘克敏
目的观察规范化疼痛护理管理在老年髋部骨折手术患者中的应用效果。方法2015年1月至2016年6月入院行髋部骨折手术的老年患者(年龄>58岁)75例,随机分为对照组37例和观察组38例;对照组采用常规疼痛管理,观察组予规范化疼痛管理。比较两组患者最强程度疼痛视觉模拟评分(VAS)和满意度计分。结果两组患者VAS评分术前无显著性差异(Z=0.845,P>0.05),术后观察组VAS评分显著低于对照组(Z=5.427,P<0.001)。观察组护理满意度评分显著高于对照组(t=21.346,P<0.001)。结论规范化疼痛管理能够显著地降低老年髋部骨折患者围术期疼痛,提高满意率,值得临床推广应用。
髋部骨折;老年;规范化疼痛管理;护理
[本文著录格式]赵克聪,孙海燕,范静宇,等.规范化疼痛管理模式在老年髋部骨折手术患者中的应用效果[J].中国康复理论与实践,2017,23(7):848-850.
CITED AS:Zhao KC,Sun HY,Fan JY,et al.Effect of standardized pain management on old patients after hip fracture surgery[J]. Zhongguo Kangfu Lilun Yu Shijian,2017,23(7):848-850.
疼痛是一种不愉快的感觉和情绪上的感受,伴有实质或潜在的组织损伤[1-2]。有效的围术期疼痛护理管理策略有助于患者康复[3-5],而不完善的术后疼痛护理管理除了增加患者痛苦外,还会增加医疗费用[6],延长患者康复时间[7],不符合加速康复外科的要求[8-11]。
老年髋部骨折手术患者围术期的疼痛程度如能维持较低水平,将有助于他们早期下床活动和接受康复训练,减少长期卧床引起的各种并发症[12]。大量数据表明,高质量的护理工作是减轻围术期疼痛程度的一个关键因素[13-16]。通过对护理工作的改进,我们在常规疼痛护理管理模式的基础上开发出更加完善的规范化疼痛护理管理模式。
1 资料与方法
1.1 一般资料
2015年1月至2016年6月,北京博爱医院收治的拟行髋部骨折手术患者75例。
纳入标准:①行髋部骨折手术且身体状态较好;②术前理解和表达能力正常;③无慢性疼痛病史;④签署知情同意书。
排除标准:①近期服用过镇痛药物;②同时接受其他疼痛管理方法;③术后出现静脉血栓、伤口感染等并发症。
本研究经本院伦理会审核批准。
随机数字表法将患者分为对照组和观察组:用微软EXCEL软件生成75个随机数字,将数字按照患者接受手术的日期一一对应,按降序重新排列。第1~38位数字对应的患者入观察组,接受规范化疼痛护理管理模式;第39~75位数字对应的患者入对照组,接受传统疼痛护理管理模式。两组患者一般资料无显著性差异(P>0.05)。见表1。
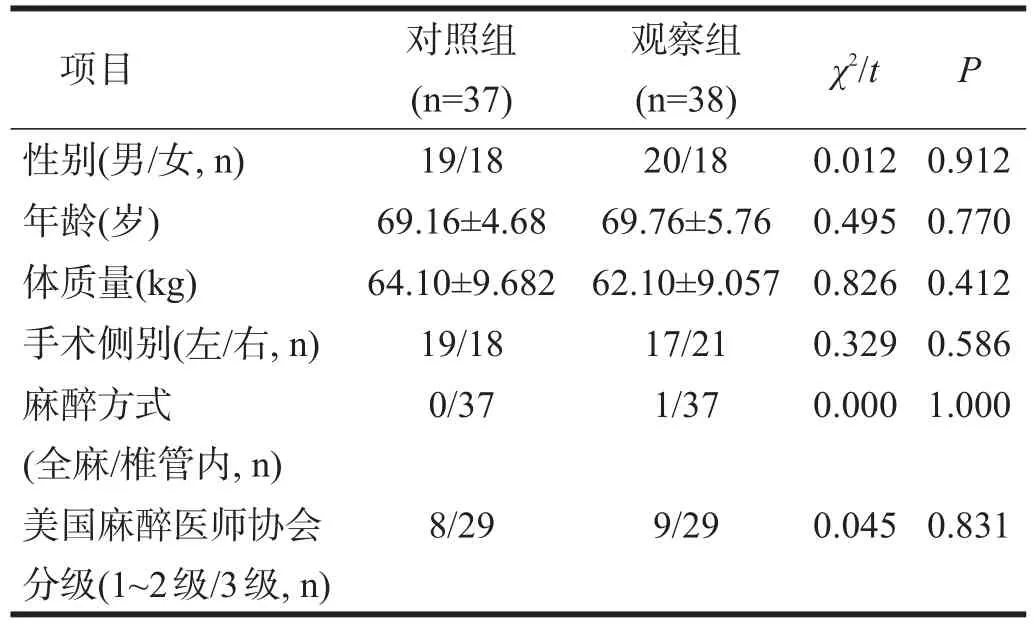
表1 两组一般资料比较
1.2 方法
1.2.1 常规疼痛管理
患者接受各项检查,护理人员介绍医院基本情况等;进行基础药物镇痛治疗,进行适当用药安全指导;介绍患者应该注意的事项,定时巡视病房,清洁卫生、换药等。
1.2.2 规范化疼痛管理
发放“骨科患者疼痛认知度调查问卷表”,掌握相关信息;对患者进行疼痛相关知识的教育宣传,主动讲授疼痛产生的原因、病理机制、治疗措施及不良反应等;对患者的疼痛程度进行综合评估,提前制定具有针对性个体化多模式疼痛护理方案;根据患者病情和临床经验进行超前镇痛;随时掌握患者心理及情绪变化,出现紧张焦虑等不良情绪时,及时采取相应的心理疏导措施,必要时请心理专科医生协助治疗;加强用药安全指导,嘱患者严格按医嘱服用止疼药,尽可能减少不良反应发生;保证病房环境的舒适和卫生,帮助患者保持良好愉快的心情和充足的休息,必要时可用镇定安神类药物提高患者睡眠质量;为患者制定科学合理的饮食方案;召开优质护理经验交流会,对疼痛护理管理过程中出现的问题和所积累的经验及时进行总结与分享;质量控制小组采用PDCA循环工作法(Plan,计划;Do,实施;Check,检查;Action,处理)对规范化疼痛护理管理中出现的问题进行处理。
1.3 评定方法
治疗前后采用疼痛视觉模拟评分(Visual Analogue Score,VAS)评价患者最高疼痛程度。出院前调查患者满意度评分。
1.3.1 VAS
用一条长10 cm直尺,两端分别标上数字“0”和“10”,“0”表示无痛,“10”表示最剧烈疼痛,标尺上的数字代表疼痛程度。不定期多次评估,取最大值。
1.3.2 患者满意度评分
发放“患者满意度调查问卷表”,每项分“非常满意”(2分)、“满意”(1分)、“不满意”(0分)三个等级,共10项,满分20分:疼痛相关知识的健康宣教;护理人员对疼痛相关知识的掌握程度;疼痛护理管理方案的可接受性及实施者的技术与能力;心理疏导的及时性和有效性;病房环境及设施;生活照顾;护理在患者饮食安排及睡眠质量中的作用;护理在康复训练质量中的作用;疼痛护理管理过程中的不良反应;患者与护理人员沟通渠道。
1.4 统计学分析
采用SPSS 19.0统计软件进行统计学分析。服从正态分布的计量资料(年龄、体质量、患者满意度评分)采用(xˉ±s)表示,组间比较采用独立样本t检验;非正态分布资料(VAS)采用中位数(四分位数)表示,采用秩和检验。计数资料用χ2检验。显著性水平α= 0.05。
2 结果
两组治疗后VAS均显著下降(P<0.001),观察组低于对照组。见表2。观察组满意度评分(18±1.53),显著高于对照组(11±1.64)(t=21.346,P<0.001)。

表2 两组治疗前后VAS的比较
3 讨论
疼痛会延长老年人髋部骨折术后的卧床时间,不仅易引起肺栓塞、肺炎、心血管意外等严重并发症[17-18],而且疼痛产生的失眠、焦虑也会影响到他们的康复计划[19]。改善围术期髋部骨折疼痛程度至关重要。
尽管目前围术期疼痛治疗手段较多,但围术期疼痛仍然没有得到很好控制[20]。护士在加速外科康复中的作用非常重要[21],由他们参与的多模式镇痛既能增加镇痛效果,又降低了不良反应[22];反之,将使得患者术后疼痛管理水平显著下降[23-24]。护士不仅应参与术后疼痛管理,而且应在术后疼痛管理中占主导地位[25]。
实施规范化疼痛护理管理模式对护士有严格的要求。护士需要主动对患者进行详细疼痛知识教育、履行合理的疼痛程度评估、提前制定个性化护理方案、动态观察心态及精神变化、实时进行心理疏导、加强用药安全指导、保障病房环境卫生舒适、制定科学合理的饮食运动方案。本研究显示,接受这种规范化疼痛护理管理模式的患者,围术期最高疼痛程度较低,患者对疼痛护理管理的满意度评分较高。
通过问卷表发现和解决临床问题是一项有效的手段[26]。发放“骨科患者疼痛认知度调查问卷表”是我们实施规范化疼痛护理管理的一个重要步骤。该表通过一系列通俗易懂的问题,了解患者对疼痛的认知以及对疼痛治疗效果的预期,同时获取患者对疼痛治疗的个体化需求,以期达到最大程度减轻患者疼痛程度的效果。
我国规范化疼痛护理管理模式仍处在初级阶段,还有许多亟待解决的问题。本研究显示,如何确保镇痛作用的时效性是整个管理过程的重点和难点;护理人员角色的转变和合理定位也是日后需要解决的问题。在实施规范化疼痛护理管理过程中,需要定期聘请专业人员对护理人员进行知识培训,提高综合素质。由于患者自身状况并不相同,而个体化护理在疼痛护理管理中有显著性作用[27],在规范化疼痛护理管理中要特别强调在主体原则一致的基础上,因人而异制定具体方案。此外,中医和音乐治疗在术后疼痛治疗中的作用益愈突出[28-29],如何在规范中融入中医和音乐治疗元素,也是我们今后研究的方向。
总之,对老年髋部骨折手术患者而言,规范化疼痛护理管理能够有效降低术后疼痛程度,提高患者满意度,是一种有效的疼痛护理管理模式。
[1]Pope N,Tallon M,McConigley R,et al.The experiences of acute non-surgical pain of children who present to a healthcare facility for treatment:a systematic review protocol[J].JBI Database System Rev Implement Rep,2015,13(10):12-20.
[2]Cesaro P,Ollat H.Pain and its treatments[J].Eur Neurol,1997,38(3):209-215.
[3]Min BW,Kim Y,Cho HM,et al.Perioperative Pain Management in Total Hip Arthroplasty:Korean Hip Society Guidelines[J].Hip Pelvis, 2016,28(1):15-23.
[4]Basat HC,Ucar DH,Armangil M,et al.Post operative pain management in shoulder surgery:suprascapular and axillary nerve block by arthroscope assisted catheter placement[J].Indian J Orthop,2016,50(6):584-589.
[5]Choi S,O'Hare T,Gollish J,et al.Optimizing pain and rehabilitation after knee arthroplasty:a two-center,randomized trial[J].Anesth Analg, 2016,123(5):1316-1324.
[6]Maiese BA,Pham AT,Shah MV,et al.Hospitalization Costs for Patients Undergoing Orthopedic Surgery Treated With Intravenous Acetaminophen(IV-APAP)Plus Other IV Analgesics or IV Opioid Monotherapy for Postoperative Pain[J].Adv Ther,2017,34(2):421-435.
[7]Gornitzky AL,Flynn JM,Muhly WT,et al.A rapid recovery pathway for adolescent idiopathic scoliosis that improves pain control and reduces time to inpatient recovery after posterior spinal fusion[J].Spine Deform,2016,4(4):288-295.
[8]Loop T.Fast track in thoracic surgery and anaesthesia:update of concepts[J].Curr OpinAnaesthesiol,2016,29(1):20-25.
[9]Khorgami Z,Petrosky JA,Andalib A,et al.Fast track bariatric surgery:safety of discharge on the first postoperative day after bariatric surgery[J].Surg Obes Relat Dis,2017,13(2):273-280.
[10]Kapritsou M,Papathanassoglou ED,Bozas E,et al.Comparative evaluation of pain,stress,neuropeptide Y,ACTH,and cortisol levels between a conventional postoperative care protocol and a fast-track recovery program in patients undergoing major abdominal surgery[J].Biol Res Nurs,2017,19(2):180-189.
[11]Agarwal BB,Chintamani,Agarwal S.Fast track surgery-minimizing side effects of surgery[J].Indian J Surg,2015,77(Suppl 3):753-758.
[12]Stambough JB,Nunley RM,Curry MC,et al.Rapid recovery protocols for primary total hip arthroplasty can safely reduce length of stay without increasing readmissions[J].J Arthroplasty,2015,30(4):521-526.
[13]Tay Swee Cheng R,Klainin-Yobas P,Hegney D,et al.Factors relating to perioperative experience of older persons undergoing joint replacement surgery:an integrative literature review[J].Disabil Rehabil, 2015,37(1):9-24.
[14]Specht K,Kjaersgaard-Andersen P,Kehlet H,et al.Nursing in fast-track total hip and knee arthroplasty:A retrospective study[J].Int J Orthop Trauma Nurs,2015,19(3):121-130.
[15]Specht K,Kjaersgaard-Andersen P,Pedersen BD.Patient experience in fast-track hip and knee arthroplasty-a qualitative study[J].J Clin Nurs,2016,25(5-6):836-845.
[16]Vaismoradi M,Skar L,Soderberg S,et al.Normalizing suffering:a meta-synthesis of experiences of and perspectives on pain and pain management in nursing homes[J].Int J Qual Stud Health Well-being,2016, 11(1):31203.
[17]Shin WC,Woo SH,Lee SJ,et al.Preoperative prevalence of and risk factors for venous thromboembolism in patients with a hip fracture:an indirect multidetector CT venography study[J].J Bone Joint Surg Am, 2016,98(24):2089-2095.
[18]Lou N,Wang D,Wang Z,et al.Management of acute postoperative hypertension for reducing cardiovascular complications in cancer patients:when and how aggressively?[J].Turk J Med Sci,2016,46(6):1634-1640.
[19]Doering LV,McGuire A,Eastwood JA,et al.Cognitive behavioral therapy for depression improves pain and perceived control in cardiac surgery patients[J].Eur J Cardiovasc Nurs,2016,15(6):417-424.
[20]Medrzycka-Dabrowska WA,Dabrowski S,Basinski A,et al.Perception of barriers to postoperative pain management in elderly patients in Polish hospitals with and without a"Hospital Without Pain"Certificate-a multi-center study[J].Arch Med Sci,2016,12(4):808-818.
[21]Ozalp Gerceker G,Karayagiz Muslu G,Yardimci F.Children's postoperative symptoms at home through nurse-led telephone counseling and its effects on parents'anxiety:A randomized controlled trial[J].J Spec Pediatr Nurs,2016,21(4):189-199.
[22]Sullivan D,Lyons M,Montgomery R,et al.Exploring opioid-sparing multimodal analgesia options in trauma:a nursing perspective[J].J Trauma Nurs,2016,23(6):361-375.
[23]Riemondy S,Gonzalez L,Gosik K,et al.Nurses'perceptions and attitudes toward use of oral patient-controlled analgesia[J].Pain Manag Nurs,2016,17(2):132-139.
[24]Vincent JL,Shehabi Y,Walsh TS,et al.Comfort and patient-centred care without excessive sedation:the eCASH concept[J].Intensive Care Med,2016,42(6):962-971.
[25]Montgomery R,McNamara SA.Multimodal pain management for enhanced recovery:reinforcing the shift from traditional pathways through nurse-led interventions[J].AORN J,2016,104(6S):S9-S16.
[26]Kulpa M,Zietalewicz U,Kosowicz M,et al.Anxiety and depression and cognitive coping strategies and health locus of control in patients with ovary and uterus cancer during anticancer therapy[J].Contemp Oncol(Pozn),2016,20(2):171-175.
[27]张建男,何亮.个性化护理干预在颅内动脉瘤介入栓塞术患者持续性头痛中的应用[J].中国康复理论与实践,2012,18(9):881-883.
[28]Wu MS,Chen KH,Chen IF,et al.The efficacy of acupuncture in post-operative pain management:a systematic review and meta-analysis[J].PLoS One,2016,11(3):e0150367.
[29]Mondanaro JF,Homel P,Lonner B,et al.Music therapy increases comfort and reduces pain in patients recovering from spine surgery[J].Am J Orthop(Belle Mead NJ),2017,46(1):E13-E22.
Effect of Standardized Pain Management on Old Patients after Hip Fracture Surgery
ZHAO Ke-cong,SUN Hai-yan,FAN Jing-yu,ZHANG Bao-cui,YANG Wei,LIU Ke-min
1.Capital Medical University School of Rehabilitation,Beijing 100068,China;2.Department of Orthopedics and Rehabilitation,Beijing Bo'ai Hospital,China Rehabilitation Research Center,Beijing 100068,China
LIU Ke-min.E-mail:keminlqliu@sina.com
ObjectiveTo observe the effects of standardized pain management on old patients with hip fracture.Methods From January, 2015 to June,2016,75 old patients(more than 58 years old)with hip fracture were randomly divided into control group(n=37)and observation group(n=38).The control group accepted routine pain management,while the observation group accepted standardized pain management.They were assessed with Visual Analogue Score(VAS)of the most intensive pain,and their scores for satisfaction were compared.Results There was no significant difference in VAS between two groups before operation(Z=0.845,P>0.05).The VAS was significantly lower in the observation group than in the control group postoperatively(Z=5.427,P<0.001).The scores of satisfaction was more in the observation group than in the control group(t=21.346,P<0.001).Conclusion Standardized pain management can significantly reduce perioperative pain in old patients after hip fracture surgery,and improve the satisfaction.
hip fracture;aged;standardized pain management;nursing
R473.6
A
1006-9771(2017)07-0848-03
2017-02-18
2017-05-22)
10.3969/j.issn.1006-9771.2017.07.024
1.首都医科大学康复医学院,北京市100068;2.中国康复研究中心北京博爱医院骨科,北京市100068。作者简介:赵克聪(1967-),女,汉族,北京市人,副主任护师,主要研究方向:骨科康复护理。通讯作者:刘克敏(1963-),男,汉族,山西长治市人,博士,主任医师,教授,主要研究方向:骨科治疗与康复。E-mail:keminlqliu@sina.com。
