镍钛记忆合金弓齿钉内固定治疗第五跖骨基底部骨折临床观察
2017-06-15谭毅贤程德根梁小军
谭毅贤+程德根+梁小军

【摘要】 目的:探究鎳钛记忆合金弓齿钉内固定治疗第五跖骨基底部骨折的疗效,为临床治疗方法的选择提供理论依据。方法:回顾性分析本院2014年3月-2016年4月收治的80例第五跖骨基底部骨折患者的临床资料。依据治疗方式不同将其分为观察组和对照组,每组各40例。观察组采用镍钛合金弓齿钉内固定治疗,对照组则采用石膏外固定治疗。术后3个月对两组骨折愈合时间、愈合率、愈合程度(AOFAS评分及VAS评分)及并发症进行比较。结果:观察组平均愈合时间为(4.9±1.3)周,明显短于对照组的(7.9±1.1)周(P<0.05)。观察组39例完全愈合,对照组32例完全愈合,两者对比差异有统计学意义(P<0.05);观察组2例出现并发症,对照组8例(P<0.05)。观察组AOFAS评分为(94.36±5.27)分,对照组为(87.10±6.31)分,两组比较差异有统计学意义(P<0.05);观察组VAS评分为(0.87±0.25)分,对照组为(1.42±0.45)分,两组比较差异有统计学意义(P<0.05)。结论:对第五跖骨基底部骨折患者行镍钛合金弓齿钉内固定治疗的临床总有效率优于外固定治疗,并发症较少,推荐临床广泛应用。
【关键词】 镍钛记忆合金弓齿钉; 内固定治疗; 第五跖骨基底部骨折; 疗效
【Abstract】 Objective:To explore effect of nickel titanium memory alloy bow tooth nail internal fixation on the treatment of the fifth metatarsal basal part fractures and to provide a theoretical basis for clinical on the fifth metatarsal bone fracture treatment methods.Method:From March 2014 to April 2016,a total of 80 fracture cases in the base of the fifth metatarsal in our hospital were divided into the observation group and control group according to different treatment methods,40 cases in each group.The observation group was treated with nickel titanium alloy bow tooth nail internal fixation,the control group was treated with plaster external fixation.After operation,the healing time,healing rate,healing degree (AOFAS score and VAS score) and the incidence of complications of the two groups were compared and analyzed.Result:After observation of 2-12 weeks,the average healing time of the observation group was significantly shorter than that of the control group,the difference was statistically significant(P<0.05).In the observation group,39 cases were healed,while 32 cases were healed in the control group,the difference had statistical significance( 字2=6.13,P<0.05);2 cases had complications in the observation group,8 cases had complications in the control group,the difference was statistical significance(P<0.05).AOFAS score of the observation group was (94.36±5.27)score,the control group of that was (87.10±6.31) score (P<0.05).VAS score of the observation group was (0.87±0.25) score,the control group was of that (1.42±0.45) score(P<0.05).Conclusion:Compared with plaster external fixation,nickel titanium alloy bow tooth nail internal fixation has higher efficiency,better curative effect and fewer complications in treatment of the fifth metatarsal basal part fracture.It is recommended to a wide range of clinical applications.And it opens the new era in the field of treatment for the fractures of the fifth metatarsal.
【Key words】 Nickel titanium memory alloy bow foot nail; Internal fixation; Fracture in the base of the fifth metatarsal; Curative effect
First-authors address:Duanzhou Peoples Hospital,Zhaoqing 526040,China
doi:10.3969/j.issn.1674-4985.2017.13.003
第五跖骨基底部骨折是临床上最常见的跖骨骨折的类型之一,常发生于足部跖屈、前足内翻时,如扭伤、砸伤、车祸等[1-3]。第五跖骨基底部骨折可依靠不同材料进行内固定治疗,如镍钛记忆合金、加压空心螺钉、可吸收螺钉等,也可采用石膏外固定的治疗方案[4]。本文就镍钛记忆合金弓齿钉内固定治疗与石膏外固定治疗进行对比研究,讨论对第五跖骨基底部骨折行镍钛记忆合金弓齿钉内固定治疗的疗效,现报道如下。
1 資料与方法
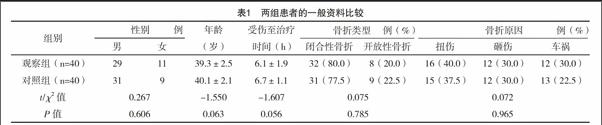
1.1 一般资料 回顾性分析本院2014年3月-2016年4月收入的80例第五跖骨基底部骨折患者临床资料,按随机数字表法分为观察组和对照组,每组40例。两组患者年龄、性别、受伤至治疗时间、骨折类型、骨折原因等一般资料比较,差异均无统计学意义(P>0.05),具有可比性,见表1。纳入标准:(1)根据Lawrence解剖分区,Ⅰ区撕脱骨折块位移>2 mm,合并跖骰关节面骨折;(2)Ⅱ区骨折块位移>2 mm。排除标准:(1)合并足踝部其他部位骨折;(2)无位移的Ⅰ、Ⅱ区骨折;(3)Ⅲ区应力性骨折。该研究已经伦理学委员会批准,患者知情同意。典型例图见图1。
1.2 方法
1.2.1 观察组 采用镍钛记忆合金弓齿钉内固定治疗方案:(1)麻醉:腰硬联合麻醉或全麻。(2)固定:患者取仰卧位,常规消毒铺单,依次切开伤处皮肤、皮下组织,显露骨折部位,清理骨折端碎骨屑,并用生理盐水进行清洗。断端对合后固定,选择合适大小镍钛记忆合金弓齿钉进行内固定。注意术后半个月到18个月,需根据患者具体情况将内固定取出[5]。(3)拆线:术后2周拆线。(4)复查X线片:术后4周复查。(5)恢复训练:术后2周拆线后,鼓励患者下床活动,要求患者拄双拐且不负重;术后4周,根据具体情况指导患者进行部分负重活动;术后6~8周进行完全负重的独立活动[6]。
1.2.2 对照组 采用石膏外固定的治疗方案:(1)麻醉:连续硬膜外麻醉。(2)固定:用石膏进行外固定[7-8]。要求患者保持中立位,石膏制动。嘱咐患者于第1、2、4、6周复诊,观察骨折处局部肿胀程度,并根据肿胀程度调整石膏的松紧度,拆线时间、复查时间、恢复训练同观察组。
1.3 观察指标 于术后2~12周内对患者进行随访,观察比较两组愈合时间、愈合率、愈合程度(AOFAS评分和VAS评分)和并发症发生情况[9-10]。AOFAS评分疼痛、功能、外观3个方面对患者进行评分,VAS评分0~10分,0分表示无痛,10分代表难以忍受的最剧烈的疼痛。
1.4 统计学处理 采用SPSS 21.0软件对所得数据进行统计分析,计量资料用(x±s)表示,比较采用t检验;计数资料以率(%)表示,比较采用 字2检验,P<0.05为差异有统计学意义。
2 结果
2.1 两组患者愈合时间比较 观察组平均愈合时间为(4.9±1.3)周,明显短于对照组(7.2±1.1)周,比较差异有统计学意义(P<0.05)。
2.2 两组患者愈合及并发症发生情况比较 观察组愈合率97.50%明显高于对照组80.00%,两组比较差异有统计学意义( 字2=6.13,P<0.05)。第五跖骨基底部骨折后可能会出现一些并发症,如踝关节背伸活动受限、感染、畸形愈合等[11-12]。观察组活动轻度受限1例,感染1例,经进一步治疗后好转,并发症发生率为5.00%,对照组背伸活动受限2例,畸形愈合2例,感染4例,并发症发生率为20.00%,两组比较差异有统计学意义( 字2=4.11,P<0.05)。见表2。
2.3 两组患者愈合程度比较 观察组AOFAS评分明显高于对照组,VAS评分低于对照组,两组比较差异均有统计学意义(P<0.05)。见表3。
3 讨论
第五跖骨基底部骨折是临床常见的跖骨骨折类型之一[10-11]。长期以来,对第五跖骨骨折的治疗多采用外固定治疗,如手法复位、夹板、石膏等[12-15]。本研究发现,与镍钛记忆合金弓齿钉内固定治疗相比,石膏外固定治疗的愈合时间相对较长、愈合率低、愈合程度(AOFAS评分及VAS评分)差,并发症发生率高。本次调查中,观察组平均愈合时间明显短于对照组患者的平均愈合时间,差异有统计学意义(P<0.05)。观察组愈合率明显高于对照组,两组对比差异有统计学意义( 字2=6.13,P<0.05),这表明镍钛记忆合金内固定治疗该类患者疗效显著,可切实增加患者愈合率;观察组并发症发生率明显低于对照组,差异有统计学意义( 字2=4.11,P<0.05)。观察组AOFAS评分为(94.36±5.27)分,对照组AOFAS评分为(87.10±6.31)分,两组比较差异有统计学意义(P<0.05);观察组VAS评分为(0.87±0.25)分,对照组患者VAS评分为(1.42±0.45)分,差异有统计学意义(P<0.05)。
镍钛记忆合金的优势在于其具有持续的压缩力,其他普通的金属材料很难企及,因此镍钛记忆合金弓齿钉的使用是第五跖骨基底部骨折治疗史上的一个里程碑[16-18]。镍钛记忆合金弓齿钉内固定治疗方法不仅使患者骨折愈合时间减少,且愈合率高、愈合程度(AOFAS评分及VAS评分)较好,并发症少见,克服了长期以来采用外固定治疗方法导致的固定不稳定、畸形愈合、局部肿胀等现象[19]。另一方面,对于医务人员来说,镍钛记忆合金弓齿钉内固定治疗操作方便,简单易行[20]。但治疗前应将镍钛记忆合金弓齿钉置于冰水中,用弓齿钉进行内固定时再进行复温,固定成功后所有用水必须是温水[21]。尽量保证手术固定一次成功,避免对镍钛记忆合金弓齿钉进行反复降温升温处理[22]。
參考文献
[1] Lobenhoffer P.Posterolateral transfibular approach to tibial plateau fractures[J].J Orthop Trauma,2011,25(3):31.
[2] Desandis B,Murphy C,Rosenbaum A,et al.Multiplanar CT Analysis of Fifth Metatarsal Morphology:Implications for Operative Management of Zone II Fractures[J].Foot & Ankle International,2015,37(5):366-369.
[3] Lui T H.Lateral foot pain following open reduction and internal fixation of the fracture of the fifth metatarsal tubercle:treated by arthroscopic arthrolysis and endoscopic tenolysis[J].Case Reports,2014,5(34):122.
[4] Aynardi M,Pedowitz D I,Saffel H,et al.Outcome of nonoperative management of displaced oblique spiral fractures of the fifth metatarsal shaft.[J].Foot Ankle Int,2013,34(12):1619-1623.
[5] Wang X,Deng Y,Yu L,et al.Comparison of hollow compression screws and absorbable screws for the treatment of the fifth metatarsal fracture:Ankle function and fracture displacement[J].Chinese Journal of Tissue Engineering Research,2015,3(1):53-54.
[6] Wang X,Zhang C,Wang C,et al.Accurate determination of screw position in treating fifth metatarsal base fractures to shorten radiation exposure time[J].Singapore Medical Journal,2016,5(12):1-13.
[7] Tsukada S,Ikeda H,Seki Y,et al.Intramedullary screw fixation with bone autografting to treat proximal fifth metatarsal metaphyseal-diaphyseal fracture in athletes:a case series[J].BMC Sports Science,Medicine and Rehabilitation,2012,4(1):1-7.
[8] Chon J G,Choi H,Kim J B,et al.The Short Term Outcome of Surgical Treatment for the Fifth Metatarsal Base Fracture Using a Headless Cannulated Compression Screw[J].J Korean Foot Ankle Soc,2016,20(3):131.
[9] Polzer H,Polzer S,Mutschler W,et al.Acute fractures to the proximal fifth metatarsal bone:Development of classification and treatment recommendations based on the current evidence[J].Injury-international Journal of the Care of the Injured,2012,43(10):1626-1632.
[10] Gasse N,Luth T,Loisel F,et al.Fixation dun transfert dun tendon divisé du tibial antérieur par ancrage sur la base du cinquième métatarsien[J].Revue De Chirurgie Orthopédique Et Traumatologique,2012,98(7):744-748.
[11] Massada M M,Pereira M A,de Sousa R J,et al.Intramedullary screw fixation of proximal fifth metatarsal fractures in athletes[J].Acta Ortopédica Brasileira,2012,20(5):262-265.
[12] Ritchie J D,Shaver J C,Anderson R B,et al.Excision of symptomatic nonunions of proximal fifth metatarsal avulsion fractures in elite athletes[J].American Journal of Sports Medicine,2011,39(11):2466.
[13] Murawski C D,Kennedy J G.Percutaneous internal fixation of proximal fifth metatarsal jones fractures (Zones II and III) with Charlotte Carolina screw and bone marrow aspirate concentrate:an outcome study in athletes[J].American Journal of Sports Medicine,2011,39(39):1295-1301.
[14] Berlet G C,Olms K,Saxena A.Fifth metatarsal fractures[J].Foot Ankle Spec,2014,7(2):127-134.
[15] DeVries J G,Cuttica D J,Hyer C F.Cannulated screw fixation of jones fifth metatarsal fractures:a comparison of titanium and stainless steel screw fixation[J].J Foot Ankle Surg,2011,50(2):207-212.
[16] Beirer M,Harrasser N,Schmidutz F,et al.Therapeutic approach to fractures of the proximal fifth metatarsalbone[J].MMW Fortschr Med,2013,155(1):53-54.
[17] Wolons D,Gandhi F,Malovrh B.An experimental investigation of the pseudoelastic hysteresis damping characteristics of nickel titanium shape memory alloy wires[J].Journal of Intelligent Material Systems & Structures,2013,9(2):116-126.
[18] Ozturk M M,Bhattacharyya A.Thermal Response of an Isolated Rectangular,Layered Nickel-Titanium Shape Memory Alloy Thin Film with Variable Material Properties[J].Lecture Notes in Engineering & Computer Science,2013,22(1):798-801.
[19] Abdullah Z,Razali R,Subuki I,et al.An Overview of Powder Metallurgy (PM) Method for Porous Nickel Titanium Shape Memory Alloy (SMA)[J].Advanced Materials Research,2016,11(33):269-274.
[20] Decker S,Kr?mer M,Marten A K,et al.A nickel-titanium shape memory alloy plate for contactless inverse dynamization after internal fixation in a sheep tibia fracture model:A pilot study[J].Technology & Health Care Official Journal of the European Society for Engineering & Medicine,2015,23(4):463.
[21] Knick C R,Srour M D,Morris C J.Characterization of sputtered nickel-titanium shape memory alloy and microfabricated thermal actuators[C].IEEE Mems,2016:524-527.
[22] Zhang B.Synchrotron Radiation X-Ray Diffraction of Nickel-Titanium Shape Memory Alloy Wires during Mechanical Deformation[J].Unt Theses & Dissertations,2015,55(3):43-45.
(收稿日期:2017-03-17) (本文編辑:周亚杰)
