Massage for migraine:A meta-analysis
2016-09-14XiaoYiTangWenRuShangZhiWenWengRuiJinQiuJinHuiTianYanGangLiuGuiHuaTian
Xiao-Yi Tang,Wen-Ru Shang ,Zhi-Wen Weng,Rui-Jin Qiu,Jin-Hui Tian,,Yan-Gang Liu*,Gui-Hua Tian,*
1TuiNa and Pain Department and Beijing,Dongzhimen Hospital,Beijing University of Chinese Medicine,100700 Beijing,China.2Key Laboratory of Chinese Internal Medicine of MOE and Beijing,Dongzhimen Hospital,Beijing University of Chinese Medicine,100700,Beijing,China.3Evidence-based Medicine Center,Lanzhou University,Lanzhou,730000,China.
Introduction
As the most common primary headache in modern society,migraine is caused by nerve,vascular function disorders,manifested as recurrent head pains with one side.This disease is also accompanied with nausea,vomiting,allergic to light and sound and is mainly divided into two types which are migraine with or without aura[1].This disease most likely attacks patients aged 25 to 55 years[2].Previous epidemiological studies showed that the 1-year prevalence rate was about 10%to 12%,and the lifetime prevalence rate was about 15%to 20%[3].Furthermore,migraine ranked seventh in the world among the causes of disability,seriously compromising the life qualities of patients[4].
Although there are conventional drugs for migraine,many patients have turned to complementary therapies to help them sustain their physical,emotional,and spiritual well being for the severe drug-tolerance and adverse reactions[5,6].Therefore,a safe and effective alternative therapy is needed.
Massage is a kind of physical treatment featured with controlled movement of the specific parts of the subject’s body,which is used to relax muscles,relieve soreness and pain and improve sleep qualities.It is convenient,effective and safe[7].
There are various theories concerning the mechanism of massage.The gate-control theory believes that massage acting on specific areas activates large diameter nerve fibers to inhibit the activities of T cells,leading to the pain release[8].Ernst et al.proposed the theory that massage could ease the pain by relaxing the body and mind as well as releasing endorphin to increase the threshold of the pain[9].Some other researchers also believe that massage can shift the autonomic nervous system[10].
Previous systematic reviews showed that massage therapy was effective for patients with pains caused by a variety of diseases(e.g.,neoplasm,osteoporosis,rheumatoid arthritis)without obvious adverse effects[10,11].Clinical trials showed that massage could effectively reduce the frequency and level of headaches of migraine,improving the quality of life.However,most of the researches were based on small samples.Therefore,this study collected the randomized controlled trials(RCTs)which treat migraine with massage,where the method of the Cochrane systematic review was used to evaluate the safety and effectiveness of massage for migraine,which may provide a reliable guidance for the choice of migraine treatment.
Methods
Types of Outcome Parameters
Major outcome parameters:(1)the efficiency.According to“Disease of TCM syndrome diagnosis curative standard”of State Administration of Traditional Chinese Medicine,efficiency is divided into:1)the clinical cure:the disappear of the headache symptoms;2)markedly effect:the effective headache symptoms basically disappeared,occasionally felt slightly headache;3)effective:headache symptom basically relieved,but still felt a sense of heavy and distention in the head;4)invalid:no effect.(2)adverse events,including nausea,fatigue,and so on.
Exclusion Criteria
Patients suffered from other types of diseases or patients were treated with 1)Chinese medicine or 2)electroacupuncture.
Search Strategies
We performed literature search in the Cochrane Library,PubMed,Web of Science,Chinese Journal Full-text Database(CNKI),and Wanfang database.Retrieval periods from each database were stopped until Oct.2015.The search terms included migraine,status migrainosus,sick headache,massage,tuian,anmo,zone therapy,reflexology, rolfing,and bodywork.We searched RCTs following the RCT search strategy of the Cochrane Reviewer Handbook 5.1.0.We used subject heading combined with free words to do other retrieval and adjusted the strategy according to different database.Wedetermined the final retrieval strategy through several pre-search.
Literature Selection
Two researchers (Tang Xiao-yi and Shang Wen-ru)independently reviewed literatures and the selected articles should make sure to be cross checked.If there were controversial issues selecting articles or disagreement between the 2 authors,a third researcher(Tian Gui-hua)was invited to evaluate processes.
Data Extraction
We extracted data according to the following principle:1)Basic information(B):the basic information of included studies,including titles,first author,published time;2)Participants(P):the basic characteristics of the objects,including the sample size of the test group and the control group;3)Intervention(I):intervention measures, including treatment’s name and frequency which was used in experiment group;4)Comparison(C):including treatment’s name and drug’s name which was used in control group;5)Outcome measures(O):including the effective rate,adverse reactions;6)Study design(S):bias risk assessment information,including random allocation method,allocation concealment method,and so on.
Quality Assessment
It was independently carried out by two reviewers(Tang Xiao-yi and Shang Wen-ru).In case of dispute,a third reviewer(Tian Gui-hua)was invited to solve the dispute.
Bias Risk Assessment
The risk of the bias assessment tool of the Cochrane Reviewer Handbook 5.1.0 was used to evaluate bias risks[12].The evaluation indicators include 1)whether used the random allocation method;2)whether hided the distribution plan;3)whether used blind methods;4)whether the data was complete;5)Whether reported results selectively;6)whether there were other possible sources of bias or not.We used"yes","clear"and"no"to answer the six questions,representing low bias,lack of relevant information or bias uncertainty and high bias,respectively.
Quality of Evidence
We used a GRADE system to evaluate the quality of evidence[13].Here are the quality grading of evidence:1)High:the effect estimates were close to the true value of the effect;2)Moderate:the true value may be approximate to the estimated value,but there was still a probability that they were totally different;3)Low:the true values may differ from the estimates;4)Very low:the real value was very likely to be quite different from the estimated value.RCT was generally believed that its evidence had high quality,but we still downgrade the quality grading of RCT through the following factors.Downgrade factors:1)the limitations of the research;2)the inconformity of results;inconsistency;3)the indirect evidence;4)the result was not accurate;5)reporting bias.
Statistical Analysis
RevMan 5.3 software was used for meta-analysis.Counting data adapted risk ratio(RR)for data analysis.They both were represented by 95%confidence intervals(Interval Confidence,CI).Heterogeneity tests were used in the I2test.If P≥0.05,and I2≤50%.The heterogeneity was not strong.Thus we used the fixed effect model.If P<0.05,I2>50%,there was a strong heterogeneity and thus sources of heterogeneity should be analyzed first.When there was a statistical heterogeneity and rather than a clinical heterogeneity,the random effects model was used to analyze data.If there was a clinical heterogeneity between different studies,or the statistical heterogeneity was too large to be explained,we abandoned pooled analysis,and used qualitative analysis.When the same index included more than 5 trails,the funnel plot was used to test publication bias[14].
GRAEDpro GDT was employed for evaluation of the quality of evidence and mapping by 2 researchers(Tang Xiao-yi,Shang Wen-ru),independently.If there were differences,we addressed the issue by detailed discussion and comparison or find the third reviewer(Tian Gui-hua)for further evaluation.
Results
Search Results
According to the retrieval strategy and the method of data collection mentioned above,153 related articles were initially located.We removed 47 duplicate articles by using EndNote X7 software and artificial screening for verification.79 articles with mismatched research objects and diagnosis methods were excluded after reading titles and abstracts.
We read full texts of 27 articles after the initial screening,and then we excluded 2 partial data duplicate publications.3 articles which were non-randomized.2 trails that control measures were not consistent with the inclusion standard,and 2 trails that outcome measures were inconsistent.In the end,a total of 18 studies and 2025 patients were included[15-32].Note that 17 studies were brought into quantitative analysis since one study with limited data could only make qualitative analysis[15].Two researchers reached results with high consistency.The flow of studiesin the PRISMA chart is shown in Figure1.
Basic characteristics of included Studies
All the studies were from China,in which 10 studies compared the massage therapy with routine drug therapies[18,21,23,25,29,31-32].1 study compared massage with acupuncture[22].5 studies compared massage+acupuncture with acupuncture [17,19,20,24,30].1 study compared 3 sub-groups,which were the massage group,the acupuncture group,and the massage+acupuncture group[16].1 study compared massage+routine nursing care with routine nursing care[15].18 literatures both used the effective rate as the main outcome measures to determine the efficacy(Table 1).

Figure1 Study flow diagram.
Risk of bias in included studies
The risk of the bias assessment tool of Reviewer Handbook 5.1.0 was used to evaluate included studies.Among included studies,in random allocations.1 study used a random number table[29],while 2 studies used a computer random digital method[21,32],and the rest only mentioned the term of“random”without detailed explanations.All studies didn’t mention the allocation concealment scheme and blinding.As for incomplete outcome data,1 trail reported drop out rate[32],which was very low and pretty balance in two groups,while the rest did not have incomplete data reported.All trails indicated no selective reporting bias.However,due to inadequate information,it was unclear whether there were other bias or not.
The evaluation results of two reviewers were basically consistent,but there was a small difference for the allocation concealment bias of 2 trails using the computer digital random method.The third researcher was invited to address this issue and came to the same conclusion.Although there was no mention of the allocation concealment method.However,it was still judged as low risks according to the decision criteria of Cochrane Reviewer Handbook 5.1.0(the computer digital random method was so subtle that the researchers cannot predict allocation schemes(Figure2,Figure3).

Table 1 Basic characteristics of included studies.

Figure 2 Graph of Risks of bias.

Figure 3 Summary of risks of bias.
Results of Statistical analysis
Effective rate
The total effective rate was reported in 18 studies.According to the differences of treatment and control measures,18 studies were divided into 4 groups,which were the massage versus regular drugs group,the massage versus acupuncture group,the massage+acupuncture versus acupuncture group,and the massage+routine nursing care versus routine nursing care group.
Massage versus regular drugs
There were 10 articles which reported the effective rate of the massage group and the regular drug group[18,21,23,25-29,31,32].According to the length of time to judge the curative effect,they were divided into 2 sub-groups,the long term group(>3 months)and the short-term group(less than 3 months).There was good homogeneity(P=0.68,I2=0%)between each study,and thus the fixed effect model was chosen.These results showed that compared with regular drugs,the massage therapy significantly improved the effective rate with statistically significant differences(RR=1.25,95%CI(1.19,1.32)P<0.000 01)(Figure 4).
Massage versus acupuncture
There were 2 studies reporting the effective rate of the massage group and the acupuncture group[16,22].There was a statistical heterogeneity among 2 studies(P=0.14,I2=54%).Therefore,the random effect model was used and the results showed that there was no statistically significant difference between massage and acupuncture(RR=0.94,95%,CI(0.77,1.16),P>0.05)(Figure 5).
Massage+acupuncture versus acupuncture
There were 6 trails reporting the effective rate of the massage group and the acupuncture+massage group[16,17,19,20,24,30].According to the length of time to judge the curative effect,they were divided into 2 sub-groups,the long term group(>3 months)and the short-term group (less than 3 months).The heterogeneity among the studies was not strong(P=0.91,I2=0%),and thus we adopted the fixed effect model.These results showed that compared with the treatment of acupuncture,massage+acupuncture therapies significantly improved the effective rate with statistically significantly difference(RR=1.11,95%CI(1.06,1.17),P<0.000 1)(Figure 6).
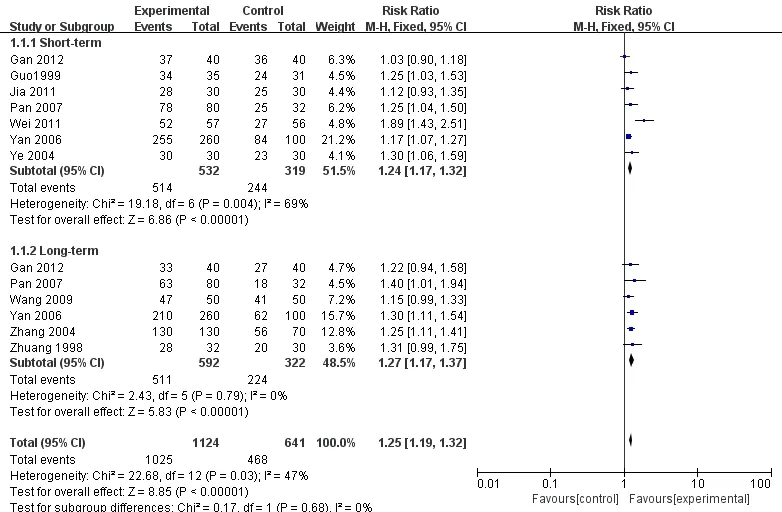
Figure4 Forest plot of comparison:Effective rate of massage versus regular drugs.

Figure5 Forest plot of comparison:Effective rate of massage versus acupuncture.

Figure6 Forest plot of comparison:Effective rate of massage+acupuncture versus acupuncture.
Massage+routine nursing careversus routine nursing care
There was 1 study reporting the effective rate of the massage+routine nursing care group and the routine nursing care group[15].The effective rate of the study group was significantly higher than the control group,and the difference was statistically significant(P<0.05).
Adverseevents
There were 2 studies reporting adverse reactions[21,23].They both reported that the massage group had no adverse reactions.More specifically,1 study reported that all patients in the flunarizine group were exhausted where 5 patients had insomnia and 3 patients felt nausea and dry[21].
Quality of evidence
Our review had 2 outcome measures,which were effective rate and adverse events.However,because of the small amount of data and the large heterogeneity,we didn’t conduct combined analysis for adverse events.Thus we only evaluated the effective rate with the GRADE system,and excluded massage+routine nursing care versus routine nursing care groups because of limited number of studies.The quality of evidence of the effects of Massage versus regular drug groups and massage+acupuncture versus acupuncture was“moderate”.The quality of evidence of the effects of massage versus acupuncture group was“low”.The two researchers were consistent with the evaluation results(Table2).
Publication bias
We made the funnel plot of massage versus regular drugs and massage+acupuncture versus acupuncture by Rev Man 5.3 software.They showed that the scattered points of the references were distributed on both sides of the line and near the top of the funnel,indicating that the publication bias was small(Figure7,Figure8).
Discussion
Summary of major results
We evaluated the effective rate and adverse events of massage for migraine.We used meta-analysis to evaluate the effective rate of massage versus regular drugs,massage versus acupuncture,and massage+acupuncture versus acupuncture.We made qualitative analysis of the adverse events and the effective rate of massage+routine nursing care and routine nursing care.The results showed that massage was superior to regular drugs and routine nursing care,and it had effects for migraine.In addition,its curative effect was comparable to acupuncture,while massage+acupuncture may produce better results without obvious adverse reactions.
Evidenceintegrity analysis
In order to reduce the possibility of selective bias,we widely searched the major Chinese and English database including Cochrane Library,PubMed,Web of Science,China Knowledge Resource Integrated Database and Wanfang database.We included databases as much as possible,and at the same time addressed the issue of database duplication carefully.RCTs are usually considered to be high quality clinical studies and thus we only included RCTs.Risk of the bias assessment tool of Cochrane Reviewer Handbook 5.1.0 was used to evaluate the risk of bias and the quality of the studies.In addition,according to the GRADE system,the quality of evidence was translated to a solid conclusion.

Figure7 Funnel plot of comparison:3.4.1.1 Effective rate of massage versus regular drugs.

Figure8 Funnel plot of comparison:3.4.1.3 Effective rate of massage+acupuncture versus acupuncture.

Table2* Summary of quality assessments.
Limitations
Limitations of included studies
Our study also had some limitations:(1)Some studies lacked baseline comparisons.(2)Since massage required manual operation,variations in the skills of massage doctors(e.g.,accuracy,strength and other changes)may lead to variations in effects.It is full of challenges to reach the same standard,which inevitably lead to bias.(3)Because of the specificity of massage,it is difficult to blame patients and researchers.(4)Outcome measures needs further optimization.Most of included studies only used “effective rate”as outcome measures,and no attention was paid to the factors that could influence the recommendation decisions,such as adverse reactions,patient tolerances,economic costs,and so on.
Limitations of systematic review
There were limitations of systematic review:(1)We failed to retrieve the relevant gray literatures,and only included Chinese and English literatures,meaning that existed literatures in other languages were not covered in this review.The results of massage versus the acupuncture group and massage+routine nursing care versus the routine nursing care group demonstrated insufficient evidences because of limited clinical studies.(3)Only two studies focused on adverse reactions,and the heterogeneity was too large to conduct meta-analysis.
Practicability
Our study was not suitable for people who were over 65 years old and under 14 years old.Most of the elderly people suffered from osteoporosis and the bodies of kids were prone to folding.The massage for the elderly people and kids should be soft.It was different from the operation requirement of included studies.
Tips for future clinical studies
Tips for future clinical studies are as follows.(1)Trials should be used sufficient random methods,and hided allocation methods.It is recommended to use a central randomization method.(2)Trials should blind researchers who measure the outcome measurements.(3)Trials should report the cases of lost to follow-up.If there are drop out cases,the ITT analysis should be conducted.(4)The above plans should be particularly explained in the methodology section of the paper.(5)Migraine has different types.The included patients should have the same type and degree of headache.(6)Western medicine always comes with adverse reactions while both the acupuncture and massage have been shown to be effective without obvious adverse reactions.In order to address the questions of patients,further comparison between Chinese medicine and western medicine is suggested using RCT.(7)Attentions should be paid to the factors that affect the recommendation decisions,such as tolerance of patients,economic cost,and adverse reactions.
Conclusion
Current evidences suggested that the massage therapy may be superior to drug therapies,and it had no obvious side effects,which could be considered as a safe and effective treatment option for migraine.In addition,there was no difference between the efficacy of massage and the acupuncture therapy while the combination of massage and acupuncture may produce better results.
Conflict of Interests
The authors declare that there is no conflict of interests regarding the publication of this paper.
1.Headache Classification Committee of the International Headache Society(IH-S).The International Classification of Headache Disorders,3rd edition (beta version).Cephalalgia 2013;33:629–808.
2.Etemad LR,Yang W,Globe D,etal.Costs and utilization of tnptan users who receive drug prophylaxis for migraine versus tnptan users who do not receive drug prophylaxis.J Manag Care Pharm 2005;11:137-144.
3.Olesen J,Lekander I,Andlin-Sobocki P,Jönsson B.Funding of headache research in Europe.Cephalalgia 2007;27(9):995–9.[MEDLINE:17727472]
4.Steiner TJ,Stovner LJ,Birbeck GL.Migraine:the seventh disabler.Cephalalgia 2013;33:289–90.
5.Dodick DW,Silberstein SD.Migraine prevention.Practical Neurology 2007;7(6):383–93.[MEDLINE:18024778]
6.Linde K,Allais G,Brinkhaus B,Manheimer E,Vickers A,White AR.Acupuncture for migraine prophylaxis.Cochrane Database of Systematic Reviews 2009,Issue 1.Art. No.: CD001218. DOI:10.1002/14651858.CD001218.pub2.
7.Song BL,Yu TY.Massage Therapeutics(version 2).Beijing:People's Health Publishing House,2012.
8.Melzack R,Wall PD.The Challenge of Pain.2nd Edition.London:Penguin Books,1996.
9.Ernst E.Massage therapy for low back pain:a systematic review.Journal of Pain and Symptom Management 1999;17(1):65–9.
10.Moyer CA,Rounds J,Hannum JW.A meta-analysis of massage therapy research.Psychological Bulletin 2004;130(1):3–18.
11.Furlan AD,Giraldo M,Baskwill A,Irvin E,Imamura M.Massage for low-back pain.Cochrane Database of Systematic Reviews 2015,Issue 9.Art.No.:CD001929.DOI:10.1002/14651858.CD001929.pub3.
12.Higgins JPT,Green S(editors).Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0[updated March 2011].The Cochrane Collaboration,2011.
13.Zeng XT,Leng WD,Li S,et al.How to Understand and Use GRADE System Correctly?A Briefly Outline.Chin J Evid-based Med 2011;11(9):985-990.
14.Wang JL.Clinical Epidemiology(version 2).Shanghai:Shanghai Scientific and Technical Publishers,2001.
15.Liao SQ,Xia LQ,Liang YH,et al.The clinical therapeutic effect of acupoint massage combined with auricular acupuncture for patients with migraine.Int J Nurs 2015;34(10):1438-1440.
16.HU Wei-qiong,XU Si-wei,ZHONG Li-wei,WANG Si-you.Observations on the Effect of Tuina plus Acupuncture for Cervical Migraine. Journal of Acupuncture and Tuina Science 2015;2(4):50-52.
17.Zhang CP.Analysis of the prognosis of migraine treated by acupuncture combined with massage therapy.China Hwalth Care&nutrition 2014;24(2):733.
18.Ye SL,Wei H,Jiang Z.Massage treatment of cervical migraine.Jiangxi Journal of Traditional Chinese Medicine 2004;(04):36.
19.Lv M,Liu XY.Clinical observation of acupuncture combined with massage for migraine.Liaoning Journal of Traditional Chinese Medicine 2006;33(5):604-604.
20.Yao H.Clinical observation of acupuncture plus massage for migraine.Journal of New Chinese Medicine 1996;(09):36.
21.Zhuang ZQ,Wang CR.Clinical observation of foot massage for migraine.Chinese Manipulation&Qi Gong Therapy 1998;(02):8-9.
22.Zhang CS,et al.Clinical study on the effect of Mongolian treatment of shaking head and it’s influence to TCD.Journal of Medicine&Pharmacy of Chinese Minorities 2014;20(11):8-11.
23.Zhang AR,Gu HD,Xu YF.Manual massage for cervical migraine.JMed Theor&Prac 2004;17(04):422.
24.Li YH.Clinical effect observation of acupuncture combined with massage in treating 80 cases of migraine.Journal of Guiyang College of Traditional Chinese Medicine 2013;35(2):161-162.
25.Pan LP.Observation and Analysis of massage for cervical migraine. Chinese Journal of Traditional Medical Traumatology&Orthopedics 2007;15(08):48-49.
26.Yan SL,Huang PY.The treatment effect of cervical migraine by tuina.Medical Journal of Chinese People's Health 2006;18(24):977-1026.
27.Wang C.Massage for migraine and it’s influence to 5-HT in peripheral blood plasma.World Chinese Medicine 2009;4(04):203.
28.Gan L.Clinical experience of treating 40 patients with migraine by massage.Clinical Journal of Chinese Medicine 2012;04(12):36-37.
29.Jia BL.The Clinical Research of pinggantongluo manipulation to treat migraine of liver-yang hyperactivity.Shandong University of Traditional Chinese Medicine 2011.
30.Zou JF.75 cases of acupuncture plus massage for vascular migraine.Journal of Nanjing University of Traditional Chinese Medicine 1994;10(06):39.
31.Guo AS,Li AH.Clinical observation of massage manipulation for migraine.Chinese Manipulation&Qi Gong Therapy 1999;15(05):6-7.
32.Wei LL,Zheng SH,Cui X.Clinical observation of 57 cases of weijiao massage for migraine.Guiding Journal of Traditional Chinese Medicine and Pharmacy 2011;17(5):72-74.
杂志排行
Traditional Medicine Research的其它文章
- Experimental research of integrative Chinese medicine in multiple sclerosis
- Complete response of hepatocellular carcinoma treated with traditional herbal medicine:A case report
- Similarities and differences of doctor-patient co-operated evidence-based medical record of treating digestive system diseases with integrative medicine compared with traditional medical records
- The effect of acupuncture plus drug versus drug alone on patients with mild cognitive impairment:a systematic review
- Effects and safety of acupuncture for DFUs:a systematic review and meta-analysis
- TMR:A new star for the research of traditional medicine