婴幼儿肝移植术的麻醉管理
2016-09-05常小丽浙江大学附属第一医院麻醉科浙江杭州310006
常小丽,吴 健(浙江大学附属第一医院麻醉科,浙江杭州310006)
婴幼儿肝移植术的麻醉管理
常小丽,吴健△(浙江大学附属第一医院麻醉科,浙江杭州310006)
目的回顾性分析婴幼儿肝移植术的麻醉管理。方法选取2013年7月21日至2014年5月20日该院收治的先天性胆道闭锁、终末期肝病接受肝移植术患儿7例(包括活体肝移植1例)。患儿入室时均无静脉通路,予以氯胺酮2~5 mg/kg和阿托品0.02 mg/kg肌内注射后开放外周静脉,先后予以咪达唑仑注射液(力月西)0.05~0.20 mg/kg、丙泊酚2~3 mg/kg、维库溴铵0.1~0.2 mg/kg、芬太尼5 μg/kg进行静脉快速诱导后经口可视下插管,麻醉维持采用2%~3%七氟烷吸入复合静脉泵注瑞芬太尼0.2~0.3 μg/(kg·min)和顺式阿曲库铵2~3 μg/(kg·min)。观察患儿一般情况、手术时间、无肝期、出血量、尿量、静脉滴注量,以及阻断前即刻、阻断后即刻、无肝期20 min、再灌注即刻、新肝期1 h和手术结束时的呼吸、循环、血气、凝血指标等变化。结果7例患儿均未出现严重麻醉相关并发症,术后顺利脱机拔管。阻断后即刻心率[(129.00±4.38)次/分]较阻断前即刻明显加快[(114.14±11.65)次/分],差异有统计学意义(P<0.05),但2个时刻平均动脉压(MAP)和中心静脉压(CVP)比较,差异无统计学意义(P>0.05);再灌注后即刻和新肝期1 h MAP[(45.14±6.49)、(54.57± 6.50)mm Hg(1 mm Hg=0.133 kPa)]较阻断前即刻[(69.57±5.97)mm Hg]明显降低,差异均有统计学意义(P<0.05),但3个时刻心率和CVP比较,差异均无统计学意义(P>0.05);手术结束时血钠水平[(139.5±3.51)mmol/L]较阻断前即刻[(133.00± 6.03)mmol/L]明显升高,再灌注后即刻和新肝期1 h血糖[分别为(11.21±3.90)、(13.91±4.48)mmol/L]较阻断前即刻[(6.39± 2.45)mmol/L]明显升高,差异均有统计学意义(P<0.05);新肝期1 h乳酸[(4.40±1.54)mmol/L]较阻断前即刻[(2.50± 2.16)mmol/L]明显升高,血pH值(7.32±0.04)较阻断前即刻(7.40±0.07)明显降低,差异均有统计学意义(P<0.05)。结论
婴幼儿肝移植术的麻醉更为精细和特殊,呼吸、循环及内环境应严密监测、及时干预,积极改善婴幼儿肝移植预后。
肝移植;麻醉;监测,手术中;血流动力学;血气分析;婴儿
在婴幼儿肝移植术中会发生多系统的、复杂的、剧烈的病理生理改变,主要表现为血流动力学、凝血功能和内环境紊乱,并危及重要脏器功能。术中连续严密的监测和有效及时的处理措施是麻醉管理的关键[1-3]。本院作为大型肝、肾移植中心,2013年7月21日至2014 年5月20日由同一手术和麻醉团队参与完成了7例婴幼儿肝移植术麻醉,其中活体肝移植1例,现将术中麻醉管理分析总结如下。
1 资料与方法
1.1一般资料7例均为先天性胆道闭锁、终末期肝病患儿,其中男2例,女5例;年龄5~12个月;体质量8~10 kg。大量腹水1例,肝功能衰竭1例,母亲供肝1例。术式均采用改良背驮式肝移植。
1.2方法
1.2.1麻醉方法患儿均在入室后建立静脉通路,无创监测心电图(ECG)、血压(NIBP)、脉搏血氧饱和度(SpO2),肌内注射氯胺酮(江苏恒瑞医药股份有限公司,批号:Kh130308)2~5 mg/kg和阿托品(上海禾丰制药有限公司,批号不详)0.02 mg/kg,同时面罩吸氧去氮,待患儿入睡后开放外周静脉通路,先后予以咪达唑仑注射液(力月西,江苏恩华药业股份有限公司,批号:20131212)0.05~0.20 mg/kg、丙泊酚(Gorden Pharme S.P. A.,批号:1303099)2~3 mg/kg、维库溴铵(浙江仙琚制药股份有限公司,批号:130201)0.1~0.2 mg/kg、芬太尼(宜昌人福医药有限责任公司,批号:20130301)5 μg/kg进行静脉快速诱导后经口可视下气管插管,呼吸模式选择压力控制通气(PCV)模式,设置吸气压力使潮气量VT为8~10 mL/kg,设定呼吸频率(RR)为20~30次/分,吸呼比为1∶2,吸入气体中氧浓度分数(FiO2)为0.6,术中维持呼气末二氧化碳分压(PETCO2)为35~45 mm Hg(1 mm Hg= 0.133 kPa)。麻醉维持采用2%~3%七氟烷(江苏恒瑞医药股份有限公司,批号:13060131)吸入复合静脉泵注瑞芬太尼(宜昌人福医药有限责任公司,批号:20130304)0.2~0.3 μg/(kg·min)和顺式阿曲库铵(江苏恒瑞医药股份有限公司,批号:13051013)2~3 μg/(kg·min)。B超引导下于桡动脉置入24 G穿刺针,颈内静脉置入双腔中心静脉导管,用以监测中心静脉压(CVP)和静脉滴注血管活性药物。
1.2.2术中管理术中采用变温毯、输血加温仪和温水冲洗等综合措施保温,并严密监测鼻咽温度变化。术中补液遵循“丢多少补多少”的原则,补液量参照术前累计丢失量、术中失血量、不显性失液量、尿量和CVP给予。术中维持血红蛋白(Hb)80~100 g/L。无肝前期和无肝期保持良好的凝血功能,新肝期预防过度纠正凝血功能形成新肝期血栓。无肝期积极补钙、降钾、纠酸并保温,避免再灌注后综合征的发生。术中根据情况予以多巴胺1~5 μg/(kg·min)静脉滴注,门静脉开放后,予以肾上腺素0.1~0.5 μg/min维持循环稳定。
1.2.3观察指标观察患儿一般情况、手术时间、无肝期、出血量、尿量、静脉滴注量,术中持续监测ECG、NIBP、SpO2、心率(HR)、平均动脉压(MAP)、CVP、体温(T)、PETCO2,以及阻断前即刻、阻断后即刻、无肝期20 min、再灌注即刻、新肝期1 h和手术结束时的呼吸、循环、血气、凝血指标等变化。
1.3统计学处理应用SPSS19.0统计软件进行数据分析。计量资料以±s表示,采用重复测量设计的方差分析,P<0.05为差异有统计学意义。
2 结 果
2.1手术基本情况7例患儿均未出现严重的麻醉相关并发症,术后顺利脱机拔管。患儿体质量(8.71±0.76)kg,年龄(8.43±2.07)个月,手术时间(371.43±44.13)min,无肝期(47.57±4.43)min,手术出血量(442.86±50.86)mL,静脉滴注浓缩红细胞(3.07±1.74)U、新鲜冰冻血浆(320.00± 157.59)mL、5%清蛋白(357.14±133.63)mL,总静脉滴注量(1 585.00±650.57)mL。见表1。
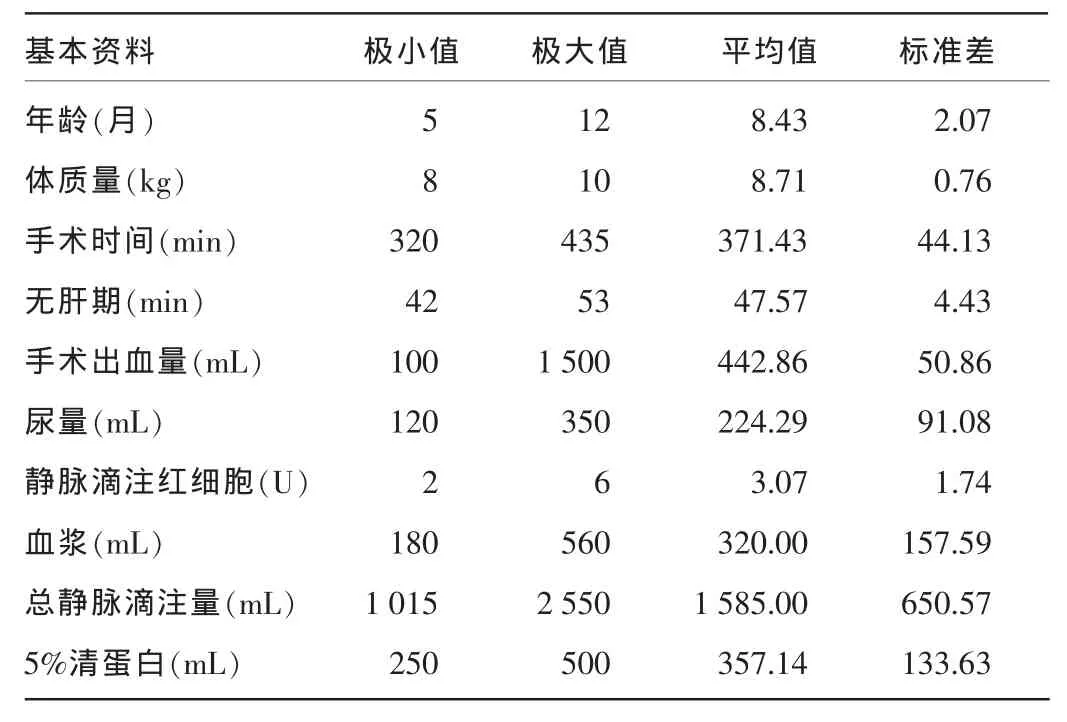
表1 患儿手术基本情况(n=7)
2.2呼吸管理患儿术前皆排除急性上呼吸道感染和肺部其他病变,于静脉诱导时面罩充氧去氮后在可视下行经口气管插管,管子型号以套囊不充气时刚刚有漏气为宜。7例患儿皆通气插管顺利,未发生喉痉挛、支气管痉挛等呼吸并发症。
2.3术中血流动力学指标的变化患儿术前均排除明显心血管系统疾病。术中除过度搬动肝脏和快速失血外,循环基本可维持稳定。与阻断前即刻比较,阻断后即刻HR明显加快,差异有统计学意义(P<0.05),但MAP 和CVP比较,差异无统计学意义(P>0.05);再灌注后即刻和新肝期1 h MAP明显降低,差异有统计学意义(P<0.05),但HR和CVP比较,差异无统计学意义(P>0.05)。见表2。
2.4术中血气分析指标的变化与阻断前即刻比较,手术结束时血钠(Na+)水平明显升高,再灌注后即刻至新肝期1h血糖(GLU)明显升高,新肝期1 h乳酸(Lac)水平明显升高,血pH值明显降低,差异均有统计学意义(P<0.05)。新肝期乳酸逐渐累积,代谢性酸中毒有加重趋势。见表3。
2.5术中凝血指标的变化与阻断前即刻比较,无肝期20 min和新肝期1 h各项凝血指标未见明显变化,差异均无统计学意义(P>0.05)。见表4。
表2 患儿术中血流动力学指标的变化(±s)

表2 患儿术中血流动力学指标的变化(±s)
注:与阻断前即刻比较,aP<0.05。
观察指标H R(次/分)M A P (m m H g )C V P (m m H g)阻断前即刻 阻断后即刻 无肝期2 0 m i n 再灌注后即刻 新肝期1 h 1 1 4 . 1 4 ± 1 1 . 6 5 6 9 . 5 7 ± 5 . 9 7 6 . 1 4 ± 3 . 2 9 1 2 9 . 0 0 ± 4 . 3 8a7 5 . 2 9 ± 8 . 5 0 3 . 0 0 ± 2 . 2 4 1 1 3 . 8 6 ± 1 5 . 4 4 6 2 . 8 6 ± 7 . 7 6 5 . 5 7 ± 3 . 8 7 1 0 3 . 2 9 ± 1 3 . 1 7 4 5 . 1 4 ± 6 . 4 9a8 . 4 3 ± 3 . 4 1 1 1 2 . 2 9 ± 9 . 7 4 5 4 . 5 7 ± 6 . 5 0a7 . 2 9 ± 4 . 5 4
表3 患儿术中血气分析指标的变化(±s)

表3 患儿术中血气分析指标的变化(±s)
注:与阻断前即刻比较,aP<0.05。K+表示血钾;Ca2+表示血钙;BE表示剩余碱;HCO3-表示碳酸氢根。
观察指标N a+(m m o l / L )K+(m m o l / L )C a2+(m m o l / L )G L U (m m o l / L )L a c (m m o l / L )B E (m m o l / L )H b (g / L )H C O3-(m m o l / L )p H阻断前即刻 无肝期2 0 m i n 再灌注后即刻 新肝期1 h 手术结束1 3 3 . 0 0 ± 6 . 0 3 3 . 4 7 ± 0 . 7 9 1 . 1 5 ± 0 . 0 6 6 . 3 9 ± 2 . 4 5 2 . 5 0 ± 2 . 1 6 -3 . 8 0 ± 3 . 3 3 8 1 . 2 9 ± 1 7 . 3 2 2 0 . 5 6 ± 2 . 8 3 7 . 4 0 ± 0 . 0 7 1 3 2 . 7 1 ± 5 . 9 4 3 . 7 7 ± 0 . 7 6 1 . 0 9 ± 0 . 0 4 8 . 2 0 ± 4 . 2 3 3 . 5 1 ± 1 . 4 6 -6 . 0 7 ± 1 . 7 3 9 4 . 8 6 ± 9 . 8 6 1 8 . 3 9 ± 1 . 8 8 7 . 3 7 ± 0 . 0 4 1 3 4 . 1 4 ± 5 . 6 4 3 . 4 4 ± 0 . 6 8 1 . 1 5 ± 0 . 1 0 1 1 . 2 1 ± 3 . 9 0a3 . 8 7 ± 1 . 2 3 -4 . 8 9 ± 2 . 9 2 9 7 . 1 4 ± 1 8 . 4 7 2 0 . 1 6 ± 2 . 3 3 7 . 3 5 ± 0 . 0 7 1 3 6 . 0 0 ± 5 . 2 9 3 . 2 3 ± 0 . 3 9 1 . 0 5 ± 0 . 0 9 1 3 . 9 1 ± 4 . 4 8a4 . 4 0 ± 1 . 5 4a-6 . 2 9 ± 2 . 0 8 8 6 . 8 6 ± 2 0 . 6 8 1 9 . 1 6 ± 1 . 7 7 7 . 3 2 ± 0 . 0 4a1 3 9 . 5 0 ± 3 . 5 1a3 . 2 6 ± 0 . 3 6 1 . 1 3 ± 0 . 0 6 9 . 7 0 ± 1 . 2 2 3 . 6 9 ± 1 . 2 1 -1 . 7 9 ± 2 . 3 3 9 6 . 5 7 ± 1 7 . 2 5 2 3 . 0 7 ± 1 . 8 2 7 . 3 7 ± 0 . 0 6
表4 患儿术中凝血指标的变化(±s)
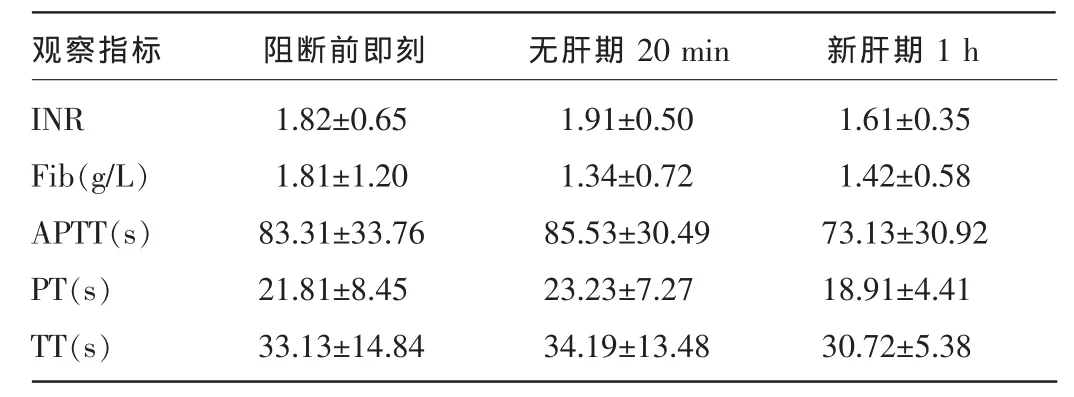
表4 患儿术中凝血指标的变化(±s)
注:INR表示国际标准化比值;Fib表示纤维蛋白原;APTT表示活化部分凝血活酶时间;PT表示凝血酶原时间;TT表示凝血酶时间。
观察指标I N R F i b (g / L )A P T T (s )P T (s )T T (s)无肝期2 0 m i n 新肝期1 h阻断前即刻1 . 6 1 ± 0 . 3 5 1 . 4 2 ± 0 . 5 8 7 3 . 1 3 ± 3 0 . 9 2 1 8 . 9 1 ± 4 . 4 1 3 0 . 7 2 ± 5 . 3 8 1 . 8 2 ± 0 . 6 5 1 . 8 1 ± 1 . 2 0 8 3 . 3 1 ± 3 3 . 7 6 2 1 . 8 1 ± 8 . 4 5 3 3 . 1 3 ± 1 4 . 8 4 1 . 9 1 ± 0 . 5 0 1 . 3 4 ± 0 . 7 2 8 5 . 5 3 ± 3 0 . 4 9 2 3 . 2 3 ± 7 . 2 7 3 4 . 1 9 ± 1 3 . 4 8
3 讨 论
近年来,婴幼儿肝移植术已在国内广泛开展,其主要适应证是肝外胆道闭锁、急性肝衰竭、Wilson病(肝豆状核变性)终末期、自身免疫性肝炎、血管瘤和肝母细胞瘤等。
本研究7例均为先天性胆道闭锁、终末期肝病患儿。先天性胆道闭锁是指婴幼儿肝内胆管、肝管或胆总管发生闭锁或不发育,肝内外胆管出现阻塞,导致淤胆性肝硬化而最终发生肝功能衰竭的疾病。其发生率在东南亚国家为1∶8 000~1∶9 000,高于欧美国家的1∶12 000~1∶15 000。男女比例约为1∶1.5。先天性胆道闭锁的病因目前尚不清楚。
手术方式包括活体肝移植和尸肝劈离式肝移植,本研究中1例为活体肝移植,供肝来自患儿母亲。婴幼儿肝移植术最大的难点是移植物体积的匹配问题,由于受体较小、血管和胆道纤细,使得手术操作极为复杂[4-5]。对患儿应做好充分的术前准备,改善营养状况,保证能量摄入,纠正明显的水、电解质、酸碱平衡紊乱,根据需要输血和血制品,提高Hb和清蛋白水平。
肝移植手术步骤复杂,尤其是门静脉阻断后的无肝期和开放后的再灌注损伤,由于婴幼儿解剖生理尚未成熟,对患儿的生理功能影响极大,很容易出现循环功能紊乱、凝血功能异常、酸中毒、电解质紊乱和低体温[6-7]。3岁以内患儿T调节中枢尚未发育成熟,体表面积大,皮下脂肪较薄,内脏暴露时间长,冷的肝脏灌注液、全身麻醉药会不同程度地抑制T调节,减少产热,术中极易出现严重的低体温。低体温会影响凝血功能,降低血小板和其他凝血因子的活性,造成术野广泛渗血,并降低组织灌注。手术室温度应在25℃左右,应严密监测T变化,输血、静脉滴注用加温仪,腹腔用温水冲洗,多重全面地做好保温措施。本研究7例患儿均做了全面的保温措施,未出现严重的低体温。
术中应维持血流动力学稳定,保证心、脑、肾等重要脏器的组织灌注[8-9]。婴幼儿体质量轻,血容量小,呼吸、循环储备功能低,对出血的敏感性更高。婴幼儿肝移植手术创伤大、出血渗血多,应及时静脉滴注血浆、Fib、凝血酶原复合物等凝血因子以改善凝血功能,同时静脉滴注清蛋白、红细胞等,尽量减少使用晶体和人工胶体液。尤其是门静脉和下腔静脉阻断后的无肝期,MAP明显降低,HR明显加快,在积极补液的同时间断注射去氧肾上腺素,微泵维持多巴胺2~5 μg/(kg·min),并注意尿量,如尿量减少,提示肾脏灌注不足,可适当补充血容量并给予呋塞米利尿[10]。由于婴幼儿血管较细,穿刺困难,本研究仅1例桡动脉穿刺置管失败,最后实施股动脉穿刺置管,与桡动脉比较,二者测得的收缩压和舒张压会有所差异,但MAP基本一致,故7例患儿循环指标具有可比性。
术中监测血气指标非常重要。动脉血气分析既可以提示呼吸参数是否需要调整,又可以实时反映内环境变化,给术中用药提供参考依据[11]。尤其是开放再灌注后的新肝初期,极易出现代谢性酸中毒、高血钾和低血钙,因此,再灌注后应尽快进行血气分析,并参照检测数据及时纠正GLU、电解质、酸碱平衡紊乱。新肝期酸中毒是由于下腔静脉阻断时血液淤积,使无氧代谢增加,产生大量酸性代谢产物,开放后进入循环;同时供肝内高浓度K+的灌注液开放后快速进入循环引起高血钾,严重时会出现心律失常和心脏骤停。低血钙是由于输入大量库存血,其中的枸橼酸螯合了血中的Ca2+,低血钙可抑制心肌收缩,减慢心脏传导,开放后应维持在1.0 mmol/L左右。
术中还应适时监测凝血指标。尤其是无肝后期和新肝初期,凝血因子减少可引起血浆PT、APTT、TT等延长,Fib下降,应适当输注血浆、Fib、凝血酶原复合物等凝血因子改善凝血功能。但是,由于婴幼儿血管较细,容易形成血栓,现在普遍认为不应过度纠正凝血功能,避免血管内血栓形成导致肝移植失败[12]。
综上所述,婴幼儿肝移植术的麻醉要求熟悉婴幼儿解剖、病理生理和药理,临床穿刺技术熟练,呼吸、循环、内环境等管理严谨周密,才能为一台成功的肝移植术保驾护航,提高手术成功率和患儿存活率。
[1]张梁,张烨,丁冠男,等.婴幼儿患者亲体肝移植术的麻醉管理[J].临床麻醉学杂志,2015,31(10):957-961.
[2]夏强,张建军,李齐根,等.婴幼儿活体肝移植33例[J].中华消化外科杂志,2011,10(1):40-43.
[3]李雅兰,彭雪梅,Claudia D,等.儿童肝移植术的麻醉处理[J].中华麻醉学杂志,2007,27(7):629-631.
[4]Yang SC,Huang CJ,Chen CL,et al.Living donor liver transplantation with body-weight more or less than 10 kilograms[J].World J Gastroenterol,2015,21(23):7248-7253.
[5]Camk1ran A,Araz C,Seyhan Ball S,et al.Anesthetic management in pediatric orthotopic liver transplant for fulminant hepatic failure and endstage liver disease[J].Exp Clin Transplant,2014,12 Suppl 1:106-109.
[6]Walia A,Mandell MS,Mercaldo N,et al.Anesthesia for liver transplantation in US academic centers:institutional structure and perioperative care[J]. Liver Transpl,2012,18(6):737-743.
[7]Bennett J,Bromley P.Perioperative issues in pediatric liver transplantation[J].Int Anesthesiol Clin,2006,44(3):125-147.
[8]Yudkowitz FS,Chietero M.Anesthetic issues in pediatric liver transplantation[J].Pediatr Transplant,2005,9(5):666-672.
[9]Elgendy H,EI Moghazy WM,Nafady-Hago H,et al.Outcome of critically-ill children after living-donor liver transplant[J].Exp Clin Transplant,2015,13 Suppl 1:S100-107.
[10]Huang CJ,Cheng KW,Chen CL,et al.Predictive factors for pediatric patients requiring massive blood transfusion during living donor liver transplantation[J].Ann Transplant,2013,18:443-447.
[11]Yang SC,Huang CJ,Chen CL,et al.Living donor liver transplantation with body-weight more or less than 10 kilograms[J].World J Gastroenterol,2015,21(23):7248-7253.
[12]Lee J,Ryu HG,Kim A,et al.Anesthetic management of an 8-month-old infant with osteogenesis imperfecta undergoing liver transplantation:a case report[J].Korean J Anesthesiol,2014,66(6):472-475.
Anesthetic management of infant and young child with liver transplantation
Chang Xiaoli,Wu Jian(Department of Anesthesiology,First Affiliated Hospital,Zhejiang University,Hangzhou,Zhejiang 310006,China)
ObjectiveTo retrospectively analyze the anesthetic management of infant and young child liver transplantation.MethodsSeven pediatric patients(including 1 cases of living donor liver transplantation)with liver transplantation due to congenital biliary atresia and end-stage liver disease in our hospital from July 21,2013 to May 20,2014 were included in this retrospective study.The patients entered into the operation room without venous access.The peripheral vein was opened after intramuscular injection of ketamine 2-5 mg/kg and atropine 0.02 mg/kg.Anesthesia were rapidly induced by intravenous midazolam 0.05-0.20 mg/kg,propofol 2-3 mg/kg,vecuronium 0.1-0.2 mg/kg and fentanyl 5 μg/kg.Then intubation was visually performed through mouth.The anesthetic maintenance adopted 2%-3%sevoflurance inhalation combined with 0.2-0.3 μg/(kg·min)remifentanil and 2-3 μg/(kg·min)cis-atracurium by venous pump.The indexes including general situation,operation time,time of anhepatic phase,amount of bleeding,urine volume and intravenous infusion amount were observed;the changes of respiration,circulation,blood gas and coagulation indicators were recorded immediately before occlusion of the portal vein,immediately after occlusion of the portal vein,20 min during the anhepatic phase,immediately after reperfusion,1 h during the neohepatic phase and end of operation.ResultsAll of the seven patients were successfully extubated without obvious anesthesia related complications.HR immediately after occlusion of the portal vein was significantly increased compared with that immediately before oc clusion,and the difference was statistically significant[(129.00±4.38)bpm/min vs.(114.14±11.65)bpm/min,P<0.05],but MAP and CVP at these two time points had no statistically significant(P>0.05);MAP immediately before occlusion of the portal vein and at 1 h during the neohepatic phase were[(45.14±6.49),(54.57±6.50)mm Hg(1 mm Hg=0.133 kPa),which were significantly decreased compared with(69.57±5.97)mm Hg before occlusion,the differences were statistically signioficant(P<0.05),but HR and CVP had no statistical differences among these 3 time points(P>0.05);blood sodium level at the end of operation was significantly increased compared with that immediately before occlusion[(139.5±3.51)mmol/L vs.(133.00±6.03)mmol/L],blood glucose levels immediately after reperfusion and at 1 h during the neohepatic phase were(11.21±3.90)mmol/L and(13.91±4.48)mmol/L respectively,which were significantly higher than(6.39±2.45)mmol/L immediately before occlusion,the differences were statistically significant(P<0.05);the lactic acid level at 1 h during the neohepatic phase was significantly increased compared with that immediately before occlusion[(4.40±1.54)mmol/L vs.2.50±2.16)mmol/L],blood pH value was significantly decreased(7.32±0.04 vs. 7.40±0.07),the difference was statistically significant(P<0.05).ConclusionAnesthesia in infant and young child liver transplantation is more elaborate and special.Respiration,circulation and internal environment should be closely monitored in order to conduct timely intervention and actively improve the prognosis of infant and young child liver transplantation.
Livertransplantation;Anesthesia;Monitoring,intraoperative;Hemodynamics;Bloodgas analysis;Infant
10.3969/j.issn.1009-5519.2016.13.015
A
1009-5519(2016)13-1997-04
常小丽(1986-),硕士研究生,主要从事临床麻醉工作。
△,E-mail:13605700492@163.com。
(2016-04-14)