Skin problems in children under five years old at a rural hospital in Southern Ethiopia
2016-08-26JosManuelRamosPaulaMolesPovedaDaluTessemaMubarackKedirGamadiSafayoAbrahamTesfasmariamFranciscoReyesIsabelBelinchon5DepartmentofPaediatricsandGeneralMedicineGamboGeneralRuralHospitalEthiopia
Jos´e Manuel Ramos,Paula Mol´es-Poveda,Dalu Tessema,Mubarack Kedir,Gamadi Safayo,Abraham Tesfasmariam,Francisco Reyes,Isabel Belinch´on5Department of Paediatrics and General Medicine,Gambo General Rural Hospital,Ethiopia
2Department of Internal Medicine,Hospital General Universitario de Alicante,Alicante,Spain
3Department of Clinical Medicine,Universidad Miguel Hern´andez de Elche,Alicante,Spain
4Department of Dermatology,Hospital Arnau de Vilanova,Valencia,Spain
5Department of Dermatology,Hospital General Universitario de Alicante,Alicante,Spain
ARTICLE INFO
Article history: Received 15 Jan 2016 Received in revised form 3 Feb 2016 Accepted 13 Mar 2016 Available online 7 Jun 2016
Skin problems in children under five years old at a rural hospital in Southern Ethiopia
Jos´e Manuel Ramos1,2,3*,Paula Mol´es-Poveda4,Dalu Tessema1,Mubarack Kedir1,Gamadi Safayo1,Abraham Tesfasmariam1,Francisco Reyes1,Isabel Belinch´on51Department of Paediatrics and General Medicine,Gambo General Rural Hospital,Ethiopia
2Department of Internal Medicine,Hospital General Universitario de Alicante,Alicante,Spain
3Department of Clinical Medicine,Universidad Miguel Hern´andez de Elche,Alicante,Spain
4Department of Dermatology,Hospital Arnau de Vilanova,Valencia,Spain
5Department of Dermatology,Hospital General Universitario de Alicante,Alicante,Spain
ARTICLE INFO
Article history: Received 15 Jan 2016 Received in revised form 3 Feb 2016 Accepted 13 Mar 2016 Available online 7 Jun 2016
Children Under five years Skin problem Scabies Impetigo
Original articlehttp://dx.doi.org/10.1016/j.apjtb.2016.05.009
ABSTRACT
Objective:To examine the prevalence of cutaneous disorders in children under 5 years old who attended a rural hospital in Southern Ethiopia.
Methods:A prospective cross-sectional study was conducted from January 26 to February 20,2015 in children under 5 years old who attended Gambo Rural Hospital in West Arsi of the Oromia Region,Ethiopia.
Results:A total of 324 children were included(59.6%male)whose median age was 16.4 months.In total,147 children[45.4%;95%confidence interval(CI):40.0%-50.8%]under 5 years had a skin problem,of which 101(68.7%)consulted for that reason.The other 46(31.3%)consulted for a general health problem and the dermatological condition was a secondary finding during the physical exploration.In 93 children(28.7%;95%CI: 20%-33.8%),it was the main disease,and in 54 children(16.5%;95%CI:13.0%-21.1%)it was concomitant with other diseases.The most common dermatological disease was scabies(n=44,13.6%;95%CI:10.3%-17.7%).Impetigo was diagnosed in 32 children (9.9%;95%CI:7.1%-13.3%),of which 23(71.9%)had complicated impetigo.Nineteen children(5.9%;95%CI:3.8%-9.0%)had eczema,10(3.1%)had eczema associated to other conditions.The following most frequent skin problems were tinea(n=9;2.8%),infected wound and ulcer(n=7;2.2%),and burns(n=6;1.9%).
Conclusions:Skin problems,mainly scabies,impetigo,and eczema were common in young children attended at a rural hospital in Southern Ethiopia.Children under 5 years should be examined thoroughly to rule out skin diseases,especially scabies.
1.Introduction
Pneumonia,diarrhea,and malaria are among the leading causes of mortality in children younger than 5 years old[1]. Integrated Management of Childhood Illness(IMCI)is an approach to child health that focuses on the well-being of the child as a whole according to the recommendations of the World Health Organization and the United Nations Children's Fund[2]. Their activities include management of childhood diarrhea(with oral rehydration salts only),malaria,malnutrition,measles,ear infection,and anemia.IMCI is performed at outpatient clinics in children under five years old[3]and in community case management performed by community health workers[4].
In the past,studies from developing countries have reported a high prevalence of skin disorders in pediatric populations[5]. Few population-based studies focus on disorders in children in low-income countries,and some of these studies are performed on healthy children at school[5-9].Despite the high frequency of certain skin diseases in developing countries,they have yet to be regarded as a significant health problem in the development of public health strategies[10].
This study was performed to learn about the burden of skin morbidity in children younger than 5 years old attended at an outpatient department of a rural hospital in Ethiopia with a view towards future integration of matters relating to skin diseases in children with the IMCI program.
2.Materials and methods
2.1.Settings
The study was performed at the Gambo General Rural Hospital(GRH),which is located in Gambo(Kore),West-Arsi province of the Oromia region.It is located in Southern Ethiopia,245 km from Addis Ababa.A Catholic missionary order manages the hospital and also the Gambo School.It is located at an altitude of 2200 meters above sea level.Subsistence farming and animal husbandry are the main occupations of the region's inhabitants.
2.2.Type of study
A prospective cross-sectional study was conducted from January 26 to February 20,2015.Children under 5 years who attended at GRH during the study period and visited by one of the three nurses at the under five-year-old outpatient clinic were included.In all,985 children visited the outpatient clinic at GRH,of which 324 were included in the study.
2.3.Socio-demographic information and physical examination
TheresearchteamconsistedofoneSpanishdermatologistandan Oromic-speaking nurse.First,the nurse visited the children according to the IMCI protocol of the Ethiopian Ministry of Health [3,4].Then,adermatologistperformedadermatologicalexamination. The medical and dermatological diagnosis was based on the anamnesis and physical examination.The dermatologist recorded clinical and epidemiological data.Infants were screened to assess general skin health,and attention was focused on skin diseases.
Clinical information was obtained using a standardized data collecting form,including variables such as place of residence,age,sex,weight,height,and type of skin disorders.Dermatological diagnosis was made based on clinical findings.Laboratory tests to confirm diagnoses were not performed.
The skin problems were classified as:(1)a skin problem as a main diagnosis and referred by relatives;or(2)a skin problem not referred by relatives but diagnosed after specific dermatological screening.
2.4.Data management
Data were coded and entered into logbooks and then analyzed using SPSS for Windows version 22.0(IBM,Chicago,Ill,USA).Continuous variables were presented as mean with standard deviation or median and interquartile range,and qualitative variables were expressed as absolute and relative frequencies.Estimates of prevalence were obtained with a 95% confidence interval(CI)using the Wilson procedure.Correlation between scabies and categorical risk factors were conducted using the Chi-square test and Student's t-test.The Kruskal-Wallis test was performed on continuous variables to see whether they had a normal or non-normal distribution(the Kolmogorov-Smirnov test with P<0.05).Statistical significance was accepted for P<0.05.
2.5.Ethical considerations
The study protocol was performed according to the Helsinki declaration and approved by Institutional Ethical Review Board of the Gambo Rural Hospital and the Ethical Review Committee of the Ethiopian Catholic Secretariat.Informed written consent was obtained from parents/guardians.Confidentiality about patient information was maintained.
3.Results
During the study,324 children were included;59.6%were male and 40.4%female.Their mean age was 16.4 months. The main cause of medical consultation was respiratory tract problems(n=135;41.7%),followed by skin problems (n=102;31.2%)and gastrointestinal problems(n=64;19.8%)(Table 1).In 93(91.2%)of the 102 children who consulted for a skin problem,this was the unique problem,and 9 cases(8.8%)presented with another medical condition. Moreover,46(14.2%)cases were diagnosed with an additional skin problem that was not the main consultation after the physical examination.In total,147 children(45.4%;95% CI:40.0%-50.8%)under 5 years had a skin problem and 54 (16.5%;95 CI:13.0%-21.1%)were associated with another medical condition.
Table 2 shows the distribution of skin problems in children. The most common skin disease detected was scabies(n=44,13.6%);25 cases were scabies without complication,and 19 cases were complicated scabies,mainly scabies with impetigo (n=15)(Table 2).Children with complicated scabies were moreprone to be referred by their parents(89.5%)than children with non-complicated scabies(72.0%)(P=0.1).Therefore,12 of 19 cases(63.2%)of complicated scabies were>12 months,and 5 of 25(20.0%)of non-complicated scabies were≤12 months (P<0.001).
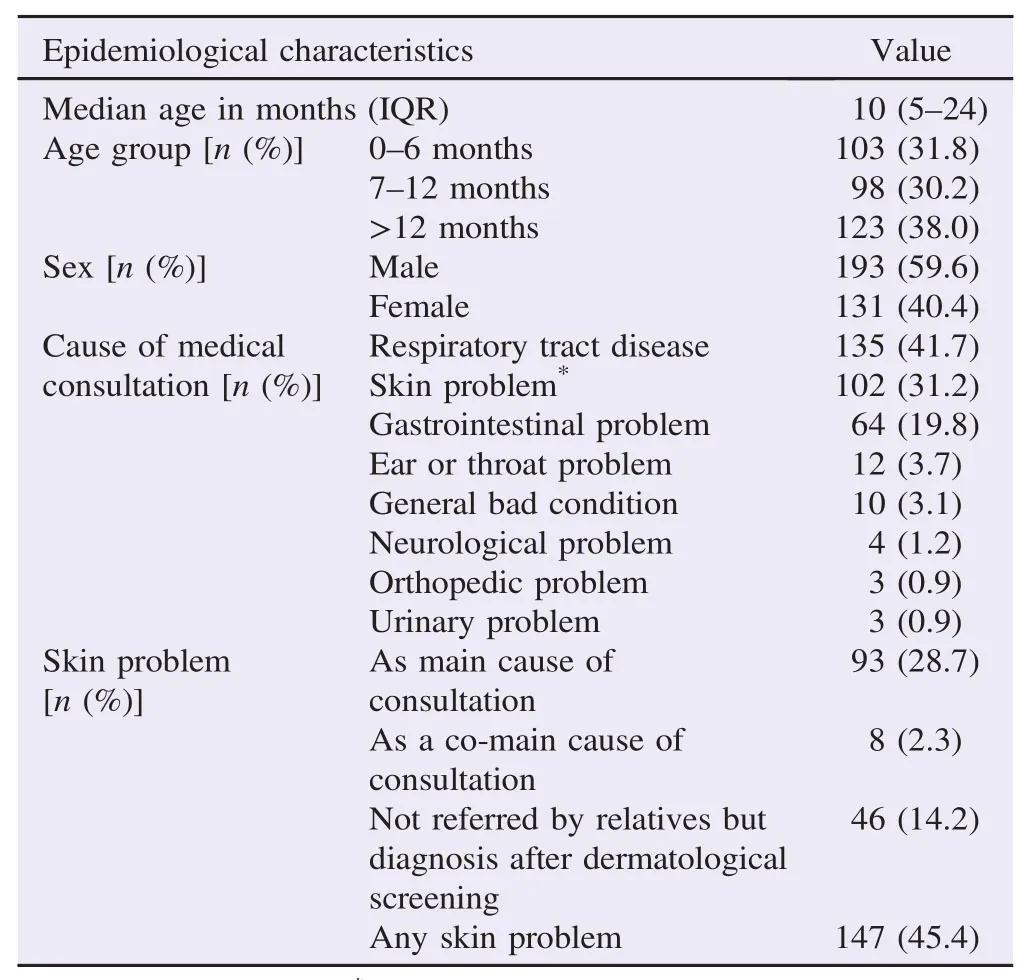
Table 1Epidemiological characteristics of children under five years old included in the study.
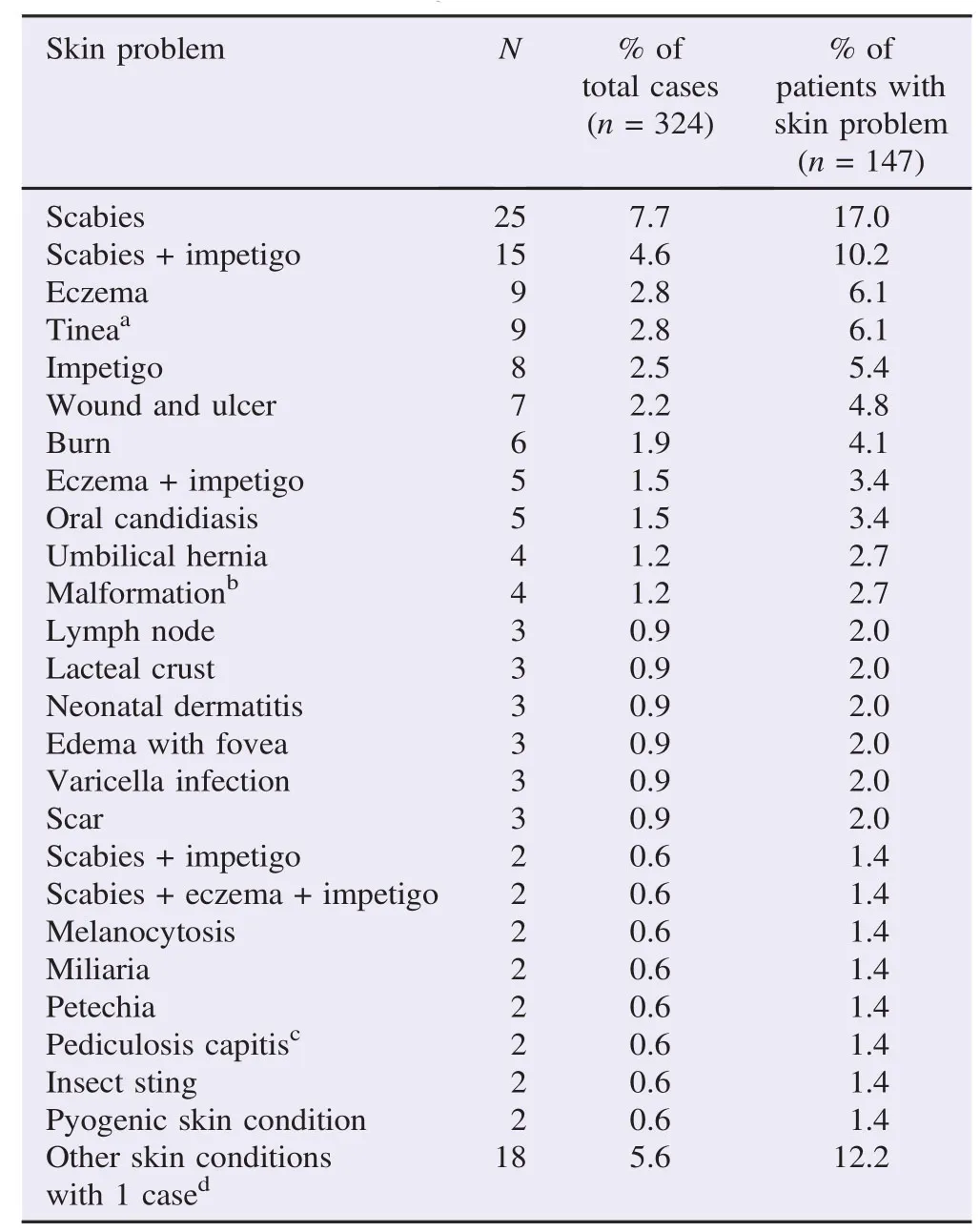
Table 2Skin problems diagnosed during dermatological examination.
Impetigo was the second skin morbidity diagnosed(n=32;9.9%);9 cases(2.8%)were only impetigo and 23(7.1%)children had impetigo with another complication.
Eczema was the third skin problem,which affected 19 children(5.9%);9 cases(2.8%)were only eczema,and 10(3.1%)children had eczema associated to another condition(scabies,scabies plus impetigo,impetigo,or tinea capitis)(Table 3).From 9 infants with eczema without other skin morbidities,4(44.4%)came to the outpatient clinic referred by relatives,and for this reason,5 were diagnosed after specific screening was performed (P<0.001).Among children aged 0-6 months 4.9%of them had eczema;of 98 children aged 7-12 months,no cases were diagnosed,and 11.4%of 123 children aged>12 months had eczema(P=0.001)(Table 4).
Tinea was the next most common skin morbidity,and it was diagnosed in 9 children(2.8%);8 cases were tinea capitis(one with secondary impetigo and another with eczema),and there was one case of tinea corporis.Tinea infection affected 2%of children between 7 and 12 months and 5.7%of them were>12 months(P=0.03)(Table 4).Infected wounds and ulcers were diagnosed in 7 children(2.2%);all of these cases came to the outpatient clinic referred by their relatives(P<0.001)(Table 3),and all of these cases were children>12 months(P=0.003)(Table 4).Six cases of burns(1.9%)were attended.Of these,five were produced by hot water,and one by hot metal.Other skin disorders diagnosed are listed in Table 2.
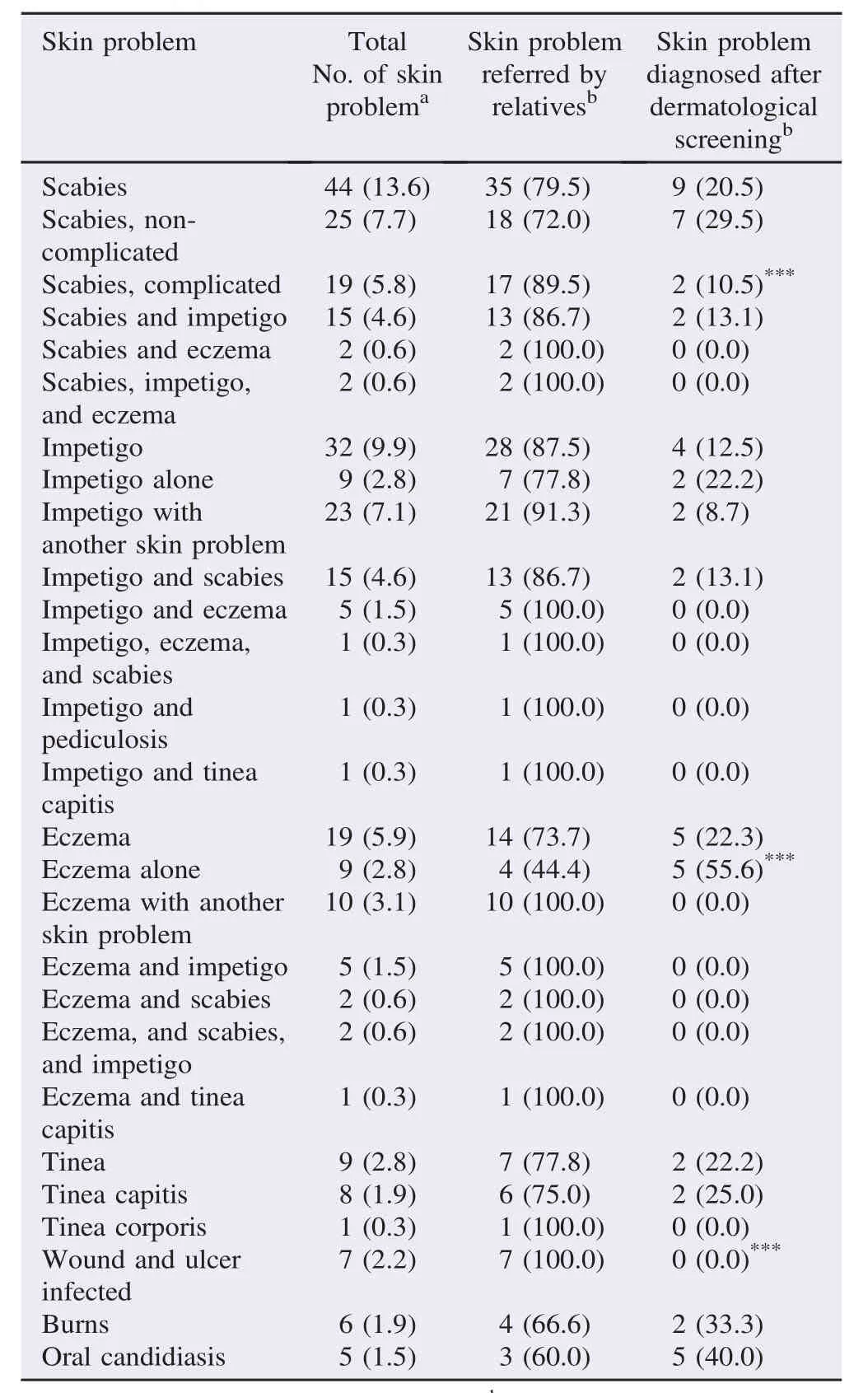
Table 3Main skin problem diagnosis according to whether the skin problem was referred by relatives or diagnosed after the skin dermatological screening.n(%).
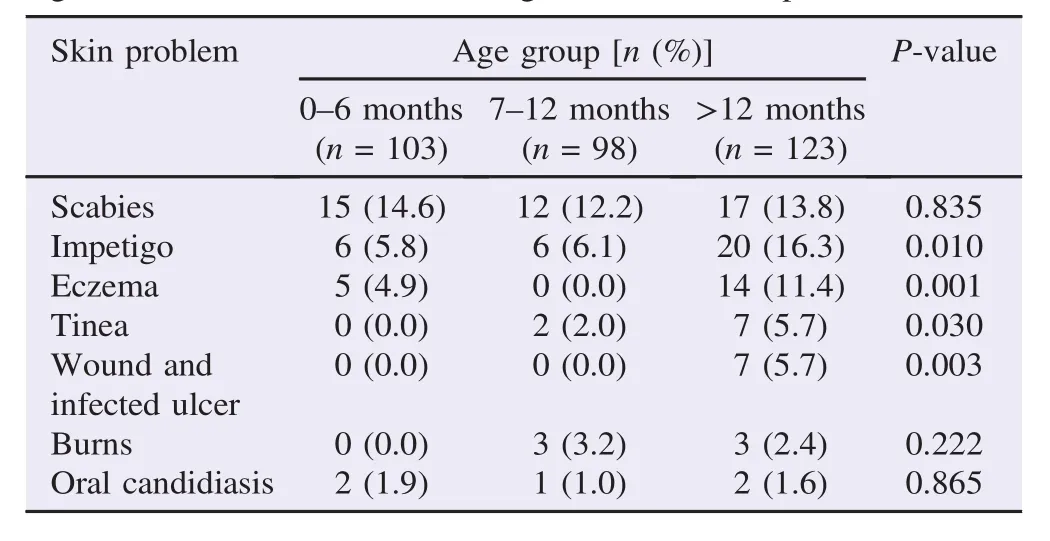
Table 4Age in months of children according to the main skin problems.
4.Discussion
In our study,skin morbidities were common in children under five years old attending our outpatient department in rural Southern Ethiopia.Scabies,impetigo,and eczema were the leading causes of skin morbidity diagnosis,followed by tinea,infected wounds,and burns.This pattern seems similar to the distribution of skin diseases described in other studies carried out at both the primary and community healthcare levels in developing countries[10,11].In fact,these skin problems are related with poverty,and are associated with particularly poor living conditions,a lack of water sanitation facilities,and lowlevel education[6,11,12].
Scabies is a neglected disease and needs to be perceived as an important public health problem causing morbidity in many resource-poor communities[13,14].In our study,it was the main skin problem diagnosed.The overall prevalence of scabies in children under five years attended in our outpatient department was 13.6%.In the study by Ukonu and Eze[6],performed at a referral center in Mekelle(an urban area of Northern Ethiopia)onadultsandchildren,scabieswasthefifthcauseof dermatological conditions attended and the first cause of admission due to dermatological diseases.However,in a study performed at a referral hospital in Addis Ababa,scabies was present in 0.9%of cases[14].In studies among schoolchildren in resource-poor communities,its prevalence ranged from 1% to 5% [7,9,15].Moreover,in a recent systematic review,the prevalence of scabies ranged from 0.2%to 71.4%[16].
Although scabies might affect people from all socioeconomic levels,the primary contributing factors in contracting it seem to be poverty,hygiene conditions,and overcrowded living situations[17].Scabies often spreads among householders rapidly,due to their close contact and overcrowding within poor housingconditions(wetandsmallhouses) [13,14]. Complications from scabies are common;in fact,scabies is very strongly associated with bacterial infection of the skin,ranging from impetigo,abscesses,and cellulitis to septicemia [14,16,18].In a recent study performed in Fiji[19],it was estimatedthat19%ofscabieswerecomplicatedwith impetigo.In our study,44.3%of scabies were complicated with impetigo and/or eczema.Our study was performed at an outpatient department of a rural hospital.Moreover,we have seen that cases with complicated scabies were more prone to come to the clinic for this reason than the cases with noncomplicated scabies.
Impetigo is another common problem.It is a skin infection related to Streptococcus pyogenes and Staphylococcus aureus infection.In our study,impetigo was secondary or associated to another skin problem in 69%of the cases.Post-streptococcal glomerulonephritis after scabies and impetigo is a known complication[20].Althoughglobalmortalityfromacute glomerulonephritis is very low and the prognosis is good in the majority of cases with complete resolution,it is an important cause of morbidity in low-and middle-income countries.
Eczematous dermatitis was another common skin problem diagnosed.In our study,5.6%of children visited had eczema,which represents 12.9%of all the skin problems.At a referral dermatological hospital in Addis Ababa(All African Leprosy Rehabilitation and Training Center),eczema accounted for 6% of the cases attended[21].At the Italian Dermatological Centre in Mekelle,where 30608 outpatients visited in 2005-2007,the leading cause of dermatological disease was eczema(22.4%)[7].In a recent cohort of children<1 year in Southern Ethiopia,the prevalence of eczema was 8.6%[22].
In a study performed in a cohort of 1065 infants,the presence of eczema in children<1 year was associated with maternal allergic history,household size of more than 4-6,and sleeping on the floor[21].We did not perform an interviewadministered questionnaire to investigate possible risk factors for eczema.
Tinea was the first skin problem in community studies and the second in school populations[5,9,15,23,24].In our study,2.9% of children under 5 years had tinea,which represents 6.8%of the cases with dermatological problems visited in our outpatient clinic.Most cases were tinea capitis.It is the rule that tinea capitis is the leading presentation of tinea infection[15,24]. Tinea infection in the present study was higher in older children attended.In studies performed in Ethiopia that done in schoolchildren,1 out of 4 had tinea[24,25].Like other skin morbidities,tinea is related to household crowding,a lack of hygiene,and it reflects low socio-economic status[8,25].
The following limitations of the study have to be taken into consideration.First of all,the sample taken was a convenience sample,we only studied the children attended by one of the three nurses working at a specific under five year outpatient clinic. Second,we did not administer a structured questionnaire regarding hygiene habits(such as sharing clothes and dealing with animals outside the house).This would be useful for identifying the risk factors associated with each skin condition. Third,diagnosis was carried out only on a clinical basis owing to the large number of children visited and the time factor.In addition,finally,the study was conducted during a hot season only.This might have influenced the prevalence of some skin diseases such as tinea and eczema.
Our study highlights the importance of skin problems,especially scabies,among children under 5 years old in a rural area of Southern Ethiopia.We recommend that all children under 5 attended at outpatient clinics should be examined to rule out skin diseases.Health extension workers and nurses,who are the main personnel visiting these children within the community or at the health center,are trained in the management of childhood malaria,malnutrition,measles,ear infection,and anemia [2,3].In light of our results,due to the high rate of skin morbidities shown in children under 5 years at the clinic,the following training implemented in the strategy of integrated community case management should be in the diagnosis and treatment of the main dermatologic problems,like scabies or impetigo.Our study reinforces an eventual integration of matters relating to skin diseases in children with IMCI programsasrecommendedinthe“Epidemiologyand ManagementofCommonSkinDiseasesinChildrenin Developing Countries”report produced by the Department of Child and Adolescent Health and Development of the WHO in 2005[10].
Moreover,as Accorsi et al.[7]and Marrone[12]stated,“skin disease control should be an important component of the strategy for poverty eradication that is in place in Ethiopia.”In fact,poverty is the major risk factor for poor health and the pathway leading from poverty to poor health includes a lack of access to decent housing,sanitation,and clean water.At the end,scabies,as a neglected disease,needs to be perceived as an important public health problem causing morbidity in many resource-poor communities.
Conflict of interest statement
We declare that we have no conflict of interest.
Acknowledgments
Paula Moles Leiva was supported by a grant from the Valencian Territorial Section of the Spanish Academy of Dermatology and Venereology(Secci´on Territorial Valenciana de la Academia Española de Dermatología y Venerología)(Solidary Grant No.1/2014).We express our gratitude to Meggan Harris for their assistance in translation and editing.
References
[1]Liu L,Johnson HL,Cousens S,Perin J,Scott S,Lawn JE,et al. Global,regional,and national causes of child mortality:an updated systematic analysis for 2010 with time trends since 2000.Lancet 2012;379:2151-61.
[2]Edward A,Kumar B,Niayesh H,Naeem AJ,Burnham G,Peters DH.The association of health workforce capacity and quality of pediatric care in Afghanistan.Int J Qual Health Care 2012;24:578-86.
[3]Shaw B,Amouzou A,Miller NP,Tafesse M,Bryce J,Surkan PJ. Access to integrated community case management of childhood illnesses services in rural Ethiopia:a qualitative study of the perspectives and experiences of caregivers.Health Policy Plan 2016;31:656-66.
[4]Miller NP,Amouzou A,Tafesse M,Hazel E,Legesse H,Degefie T,et al.Integrated community case management of childhood illness in Ethiopia:implementation strength and quality of care.Am J Trop Med Hyg 2014;91:424-34.
[5]Murgia V,Bilcha KD,Shibeshi D.Community dermatology in Debre Markos:an attempt to define children's dermatological needs in a rural area of Ethiopia.Int J Dermatol 2010;49:666-71.
[6]Ukonu AB,Eze EU.Pattern of skin diseases at university of Benin teaching hospital,Benin city,Edo State,South-South Nigeria:a 12 month prospective study.Glob J Health Sci 2012;4:148-57.
[7]Accorsi S,Barnabas GA,Farese P,Padovese V,Terranova M,Racalbuto V,et al.Skin disorders and disease profile of poverty: analysis of medical records in Tigray,Northern Ethiopia,2005-2007.Trans R Soc Trop Med Hyg 2009;103:469-75.
[8]MarroneR,VignallyP,RossoA,DideroD,PizziniE,DassoniF,etal. EpidemiologyofskindisordersinEthiopianchildrenandadolescents: ananalysisofrecordsfromtheItalianDermatologicalCentre,Mekelle,Tigray,Ethiopia,2005 to 2009.Pediatr Dermatol 2012;29:442-7.
[9]Oninla OA,Oninla SO,Onayemi O,Olasode OA.Pattern of paediatric dermatoses at dermatology clinics in Ile-Ife and Ilesha,Nigeria.Paediatr Int Child Health 2016;36:106-12.
[10]von Philipsborn P,Steinbeis F,Bender ME,Regmi S,Tinnemann P. Poverty-related and neglected diseases-an economic and epidemiological analysis of poverty relatedness and neglect in research and development.Glob Health Action 2015;8:25818.
[11]Hay RJ,Bendeck SE,Chen S,Estrada R,Haddix A,McLeod T,et al.Skin diseases.In:Jamison DT,Breman JG,Measham AR,Alleyne G,Claeson M,Evans DB,et al.,editors.Disease control priorities in developing countries.2nd ed.New York:Oxford University Press;2006,p.707-22.
[12]Morrone A.Poverty,health and development in dermatology.Int J Dermatol 2007;46:1-9.
[13]Abou-El-Naga IF.Demographic,socioeconomic and environmental changes affecting circulation of neglected tropical diseases in Egypt.Asian Pac J Trop Med 2015;8:881-8.
[14]Heukelbach J,Mazigo HD,Ugbomoiko US.Impact of scabies in resource-poor communities.Curr Opin Infect Dis 2013;26:127-32.
[15]Emodi LJ,Ikefuna AN,Uchendu U,Duru UA.Skin diseases among children attending the out patient clinic of the University of Nigeria teaching hospital,Enug.Afr Health Sci 2010;10:362-6.
[16]Romani L,Steer AC,Whitfeld MJ,Kaldor JM.Prevalence of scabies and impetigo worldwide:a systematic review.Lancet Infect Dis 2015;15:960-7.
[17]Hegab DS,Kato AM,Kabbash IA,Dabish GM.Scabies among primary schoolchildren in Egypt:sociomedical environmental study in Kafr El-Sheikh administrative area.Clin Cosmet Investig Dermatol 2015;8:105-11.
[18]Romani L,Koroivueta J,Steer AC,Kama M,Kaldor JM,Wand H,et al.Scabies and impetigo prevalence and risk factors in Fiji:a national survey.PLoS Negl Trop Dis 2015;9:e0003452.
[19]Steer AC,Jenney AW,Kado J,Batzloff MR,La Vincente S,Waqatakirewa L,et al.High burden of impetigo and scabies in a tropical country.PLoS Negl Trop Dis 2009;3:e467.
[20]Ralph AP,Carapetis JR.Group a streptococcal diseases and their global burden.Curr Top Microbiol Immunol 2013;368:1-27.
[21]Gimbel DC,Legesse TB.Dermatopathology practice in Ethiopia. Arch Pathol Lab Med 2013;137:798-804.
[22]Kelbore AG,Alemu W,Shumye A,Getachew S.Magnitude and associated factors of atopic dermatitis among children in Ayder referral hospital,Mekelle,Ethiopia.BMC Dermatol 2015;15:15.
[23]Kalu EI,Wagbatsoma V,Ogbaini-Emovon E,Nwadike VU,Ojide CK.Age and sex prevalence of infectious dermatoses among primary school children in a rural South-Eastern Nigerian community.Pan Afr Med J 2015;20:182.
[24]Leiva-Salinas M,Marin-Cabanas I,Betlloch I,Tesfasmariam A,Reyes F,Belinchon I,et al.Tinea capitis in schoolchildren in a rural area in Southern Ethiopia.Int J Dermatol 2015;54:800-5.
[25]Teklebirhan G,Bitew A.Prevalence of dermatophytic infection and the spectrum of dermatophytes in patients attending a tertiary hospital in Addis Ababa,Ethiopia.Int J Microbiol 2015;2015: 653419.
*Corresponding author:Jos´e Manuel Ramos,Department of Internal Medicine,Hospital General Universitario de Alicante,Calle Pintor Baeza,12,03010 Alicante,Spain.
Tel:+34 965933000
E-mail:jramosrincon@yahoo.es
The study protocol was performed according to the Helsinki declaration and approved by Institutional Ethical Review Board of the Gambo Rural Hospital and the Ethical Review Committee of the Ethiopian Catholic Secretariat.Informed written consent was obtained from parents/guardians.Confidentiality about patient information was maintained.
Foundation Project:Valencian Territorial Section of the Spanish Academy of Dermatology and Venereology(Secci´on Territorial Valenciana de la Academia Española de Dermatología y Venerología)(Solidary Grant No.1/2014).
Peer review under responsibility of Hainan Medical University.The journal implements double-blind peer review practiced by specially invited international editorial board members.
杂志排行

Asian Pacific Journal of Tropical Biomedicine的其它文章
- Larvicidal activities of chinaberry,neem and Bacillus thuringiensis israelensis(Bti)to an insecticide resistant population of Anopheles arabiensis from Tolay,Southwest Ethiopia
- Cutaneous leishmaniasis in Iran:Results from an epidemiological study in urban and rural provinces
- Increased uptake of intermittent preventive treatment for malaria in pregnant women in Zambia(2006-2012):Potential determinants and highlight of lessons learnt
- A review of concurrent infections of malaria and dengue in Asia
- Precise identification of different stages of a tick,Ixodes granulatus Supino,1897 (Acari:Ixodidae)
- In vivo assessment of the toxic potential of Dissotis rotundifolia whole plant extract in Sprague-Dawley rats