质子泵抑制剂发生小肠细菌过生长的临床研究
2016-08-18周东晓陈光耀马英杰郑州人民医院消化科河南郑州45000郑州消化疾病研究所河南郑州45000新乡医学院研究生部河南新乡4500
杨 丽 周东晓 陈光耀 高 晓 马英杰▲1.郑州人民医院消化科,河南郑州 45000;2.郑州消化疾病研究所,河南郑州 45000;.新乡医学院研究生部,河南新乡 4500
质子泵抑制剂发生小肠细菌过生长的临床研究
杨丽1,2周东晓3陈光耀3高晓3马英杰1,2▲
1.郑州人民医院消化科,河南郑州450003;2.郑州消化疾病研究所,河南郑州450003;3.新乡医学院研究生部,河南新乡453003
目的探讨长期口服质子泵抑制剂(proton pump inhibitors,PPI)引发小肠细菌过生长(small intestinal bacterial overgrowth,SIBO)的风险及干预措施。方法选取77例服用PPI为观察组,41例健康志愿者作为对照组,采用前瞻性对照性研究,采用乳果糖氢呼气试验(lactulose hydrogen breath test,LHBT)检测SIBO。SIBO阳性者给予停用PPI或不停用PPI加服左氧氟沙星口服(0.2 g,tid,1周),两种干预均在4周时再次复查SIBO。结果研究开始前和8周后PPI组和对照组SIBO阳性率差异无统计学意义(P>0.05),24周后PPI组SIBO阳性率明显高于对照组(P<0.05)。PPI组随着用药时间的延迟,SIBO发生率升高,0、8、24周间差异有统计学意义(P<0.05)。停药和服用抗菌药物SIBO转阴率差异无统计学意义(P>0.05)。结论 服用PPI可增加小肠细菌过生长的风险,且这种风险随服药时间延长而升高,停药或加用抗菌药物可以使SIBO消失。
质子泵抑制剂;乳果糖氢呼气试验;小肠细菌过生长;干预
质子泵抑制剂(proton pump inhibitors,PPI)因其强大的抑酸作用及低毒性的特点,被广泛应用于酸相关性疾病的临床治疗及预防非甾体抗炎药相关的胃肠出血风险防范,具有良好的效果。但是,随着临床应用的日益广泛以及对其药物特性及安全性的进一步认识,其可能的潜在风险也受到了关注。该课题拟就长期服用PPI是否会增加小肠细菌过增长(small intestinal bacteria overgrowth,SIBO)的风险进行观察研究,现报道如下。
1 资料与方法
1.1临床资料
观察组选取2013年6月~2015年6月在郑州人民医院消化科就诊需常规剂量服用PPI的患者77例,男41例,女36例,年龄31~75岁,平均(42.9±10.1)岁,77例服用PPI疗程均达8周以上,其中48例持续用药24周以上;对照组为41例健康志愿者,男24例,女17例,年龄23~70岁,平均(37.5±11.9)岁,对照组患者不使用任何药物。两组的年龄、性别等一般资料比较差异均无统计学意义(P>0.05),具有可比性。
观察组和对照组在入选前8周内均未使用过任何微生态制剂、抗生素及胃肠动力调节药物;无胃肠道及腹部手术史。
1.2评估与干预
观察对象开始(0周)、8周、24周时检测小肠细菌,SIBO阳性者根据患者服药要求和意愿分别给予停药观察4周、或不停用PPI加服左氧氟沙星口服(0.2 g,tid,1周),两种干预措施均在4周时复查SIBO。
1.3SIBO检测方法
应用乳果糖氢呼气试验(lactulose hydrogen breath test,LHBT)检测小肠细菌过度生长情况。气体检测设备为英国Bedfont公司生产的EC60 Gastrolyzer,氢气浓度以ppm表示,检测范围0~500 ppm,灵敏度为1 ppm,精度±5%。连接仪器的为新型D型接口。底物为荷兰苏威制药生产的乳果糖口服液(商品名:杜密克)。按照操作手册的操作规程对患者进行乳果糖氢气呼气试验(LHBT)。先测空腹氢气浓度,然后口服乳果糖10 g(可加少许温水送服),每15分钟测试1次呼气氢浓度,共2 h。基础值超过20 ppm或试餐后呼气氢浓度上升超过12 ppm为SIBO阳性,如基础值低于20 ppm或试餐后呼气氢浓度上升低于12 ppm为SIBO阴性。
1.4统计学分析
采用SPSS17.0统计学软件包进行数据处理,计数资料以率(%)表示,采用χ2检验;计量资料以表示,采用t检验,P<0.05为差异有统计学意义。
2 结果
2.1PPI与SIBO发生的相关性
开始时和8周时PPI组和对照组的SIBO阳性率比较差异无统计学意义(P>0.05)。其中48例继续服PPI至24周者,有10例检测出阳性,24周累计阳性率58.3%(28/48),其中23例SIBO阳性纳入干预研究。对照组8周时检出1例阳性,24周时检测出1例,累计阳性率17.1%(7/41),两组24周累计阳性率比较差异有统计学意义(P<0.05),对照组有6例纳入干预研究。PPI组随着用药时间延迟,SIBO发生率升高,0、8、24周间差异有统计学意义(P<0.05)。见表1。

表1 PPI与SIBO发生的相关性[%(n/n)]
2.2SIBO阳性者的干预结果
共29例纳入干预观察,11例是完成PPI疗程的观察对象,均不给予抗菌药物治疗;18例为对照组的6例和PPI组的12例(继续服用PPI)给予左氧氟沙星口服1周。4周复测LHBT。结果服用抗菌药物和停药PPI两组SIBO转阴率差异无统计学意义(P>0.05)。提示PPI引发者停用PPI大部分可自行恢复;服用抗菌药物可使SIBO消失。见表2。
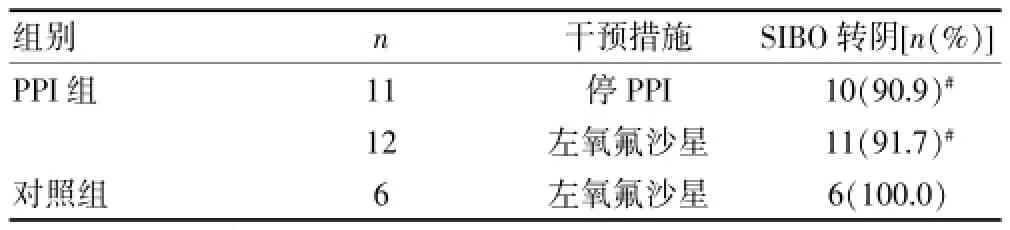
表2 SIBO阳性者的干预结果
3 讨论
健康人的胃、十二指肠、空肠细菌的种类及数量极少,主要为革兰阳性需氧菌,如链球菌、葡萄球菌和乳酸杆菌。回肠末端由于肠液流量少,蠕动减慢,细菌数逐渐增加,主要含乳酸杆菌、大肠埃希菌、类杆菌和梭状芽胞杆菌等[1]。正常小肠肠道菌群,受到胃酸、胆酸、胆盐、胃肠道的节律运动、黏膜分泌(消化酶、抗体免疫物质)和更新脱落、黏液流动、肠腔电位等调节,仅有极少量的革兰阴性厌氧菌存在并维持着小肠生态的相对稳定[2]。SIBO是一种肠道内的细菌移位导致小肠内厌氧菌群数量增多或者种类改变的状态,表现为腹胀、腹泻、营养吸收不良以及小肠动力异常等的临床综合征[3]。引起SIBO的病因较多,成人报道较多的病因有胃酸减少或胃酸缺乏性、小肠壅积、小肠动力障碍、胰腺疾病[4-7]。
Husebye等[8]认为升高小肠1个pH值相当于小肠内微生物计数增加了13.8%。PPI制剂强效抑酸导致的胃酸分泌低下可能引起潜在副作用也受到关注。目前对PPI引起SIBO的机率、发病的时间、危害、明确的机制等问题,尚不十分清楚。Ratuapli等[9]对566例服用PPI的患者进行了LHBT,发现服用PPI组的SIBO阳性率与未服药组的阳性率无明显差异,但是并未将PPI的使用时间纳入。Lombardo等[10]发现长期服用PPI制剂者SIBO患病率为50%。Lo WK等[11]最近对有关质子泵抑制剂的使用与SIBO关系进行了Meta分析,结果提示使用PPI的患者患SIBO的合并危险度是未使用者的2.282倍。国内研究认为PPI的使用时间与SIBO阳性率均存在正相关[12,13]。在PPI长期应用发生SIBO的机制中,推测PPI导致的胃酸分泌低下及对宿主防御能力的影响可能是主要原因。有研究表明,PPI在体外表现出对中性粒细胞功能的损害,降低其对内皮细胞的粘附能力[14]。
本研究通过乳果糖氢呼气试验,检测服用PPI制剂患者的小肠细菌生长情况。结果发现服用PPI制剂8周SIBO累计阳性率为37.5%,24周SIBO累计阳性率为58.3%,而对照组同时点SIBO阳性率分别为12.2%、14.6%。说明SIBO在PPI制剂服用人群中有较高的发生率,且随着服药时间的延长,发生率有逐渐上升的趋势。由于各种临床症状的重叠,与PPI使用相关的SIBO常被忽视。文献报道对症状轻微的SIBO患者,限制碳水化合物的膳食,增加脂肪、矿物质和维生素,相关症状可缓解。对于症状明显者,推荐1~2周标准剂量的抗菌药物,如利福昔明、左氧氟沙星等,或在1个短疗程的抗菌药物之后,给予益生菌[15,16]。本研究发现不停用PPI应用左氧氟沙星有较好效果。
[1]Erwin G Zoetendal,Jeroen Raes,Bartholomeus van den Bogert,et al.The human small intestinal microbiota is driven by rapid uptake and conversion of simple carbohydrates[J].ISME J,2012,6(7):1415-1426.
[2]Delphine M Saulnier,Yehuda Ringel,Melvin B Heyman,et al.The intestinal microbiome,probiotics and prebiotics in neurogastroenterology[J].Gut Microbes,2013,4(1):17-27.
[3]Jan Bures,Jiri Cyrany,Darina Kohoutova,et al.Small intestinal bacterial overgrowth syndrome[J].World J Gastroenterol,2010,16(24):2978-2990.
[4]MariaCarmenCollado,MariaCernada,ChristineBaüerl,etal. Microbial ecology and host-microbiota interactions during early life stages[J].Gut Microbes,2012,3(4):352-365.
[5]Sachdev AH,Pimentel M.Gastrointestinal bacterial overgrowth:Pathogenesis and clinical significance[J].Ther Adv Chronic Dis,2013,4(5):223-231.
[6]Richard A Schatz,Qing Zhang,Nilesh Lodhia,et al.Predisposing factors for positive D-Xylose breath test for evaluation of small intestinal bacterial overgrowth:A retrospective study of 932 patients[J].World J Gastroenterol, 2015,21(15):4574-4582.
[7]Larry S Miller,Anil K Vegesna,Aiswerya Madanam Sampath,et al.Lleocecal valve dysfunction in small intestinal bacterial overgrowth:A pilot study[J].World J Gastroenterol,2012,18(46):6801-6808.
[8]Husebye E,Hellström PM,Sundler F,et al.Influence of microbial species on small intestinal myoelectric activity and transit in germ-free rats[J].Am J Physiol Gastrointest Liver Physiol,2001,280(3):368-380.
[9]Ratuapli SK,Ellington TG,O'Neill MT,et al.Proton pump inhibitor therapy use does not predispose to small intestinal bacterial overgrowth[J].Am J Gastroenterol,2012,107 (5):730-735.
[10]Lombardo L,Foti M,Ruggia O,et al.Increased incidence of small intestinal bacterial overgrowth during proton pump inhibitor therapy[J].Clin Gastroenterol Hepato,2010,8(6):504-508.
[11]Lo WK,Chan WW.Proton pump inhibitor use and the risk of small intestinal bacterial overgrowth:A metaanalysis[J].Clin Gastroenterol Hepatol,2013,11(5):483-490.
[12]宋明伟,姜葵.质子泵抑制剂与小肠细菌过生长关系的研究[J].天津医科大学学报,2014,20(6):445-447,458.
[13]金玲肖,刘福,龙惠珍,等.应用质子泵抑制剂导致小肠细菌过度生长发生的可能性[J].中国微生态学杂志,2010,22(12):1113-1114.
[14]Yoshida N,Yoshikawa T,Tanaka Y,et al.A new mechanism for anti-inflammatory actions of proton pump inhibitors-inhibitory effects on neutrophil-endothelial cell interactions[J].AlimentPharmacolTher,2000,14(1):74-81.
[15]Rosania R,Giorgio F,Principi M,et al.Effect of probiotic or prebiotic supplementation on antibiotic therapy in the small intestinal bacterial overgrowth:A comparative evaluation[J].Curr Clin Pharmacol,2013,8(2):169-172.
[16]Hamvas J.Proton pump inhibitor therapy and small bowel bacterial contamination[J].Orv Hetil,2012,153(33):1287-1293.
Assessment and intervention of small intestinal bacterial overgrowth during proton pump inhibitor therapy
YANG Li1,2ZHOU Dongxiao3CHEN Guangyao3GAO Xiao3MA Yingjie1,2
1.Department of Gastroenterology,Zhengzhou People's Hospital,Zhengzhou 450003,China;2.Zhengzhou Institute of Digestive Disease,Zhengzhou450003,China;3.Graduate Division,Xinxiang Medical College,Xinxiang453003,China
Objective To investigate the prevalence of small intestinal bacterial overgrowth(SIBO)in patients with longterm treatment with proton pump inhibitors(PPI),and explore the intervention measures for SIBO.Methods 77 patients treatment of PPI were selected as observation group,41 healthy volunteers were selected as control group,all subjects were prospectively analysed by lactulose hydrogen breath test(LHBT).SIBO positive persons were given stopping PPI or levofloxacin(0.2 g,tid,1 w)and not stoping PPI,and all subjects
SIBO review in 4 weeks.Results The SIBO positive rates had no statistically significant differences between two groups before and 8 weeks after the PPI treatment (P>0.05).After 24 weeks,the SIBO positive rate of the PPI group was significantly higher than that of the control group (P<0.05).The SIBO positive rate of PPI treatment group was increased with the extension of treatment time.There was significant difference at pre-treatment,8 weeks post-treatment and 24 weeks post-treatment in PPI treatment group (P<0.05).The SIBO negative conversion had no significantly differences between the PPI stopping group and antibiotics treatment group(P>0.05).Conclusion Taking PPI can increase the risk of small intestinal bacterial overgrowth,and this risk increases with the time of drug administration,SIBO can be turned negative by using antibiotic or stop taking PPI. [Key words]Proton pump inhibitors;Lactulose hydrogen breath test;Small intestinal bacteria overgrowth;Intervention
R378
B
1673-9701(2016)14-0097-03
河南省郑州市科技项目(CZSYJJ13015)