Effect of aerobic exercise on insulin resistance and central adiposity disappeared after the discontinuation of intervention in overweight women
2016-07-21ShenglongLeLijunMoDjingLuYifnYngXioTnPetriWiklunSulinCheng
Shenglong Le,Lijun Mo*,Djing Lu*,Yifn Yng,Xio Tn,Petri Wiklun,Sulin Cheng,c
aDepartment of Physical Education,Shanghai Jiao Tong University,Shanghai 200240,ChinabSchool of Physical Education and Training,Shanghai University of Sport,Shanghai 200438,ChinacSchool of Kinesiology,Shanghai University of Sport,Shanghai 200438,ChinadDepartment of Health Sciences,University of Jyväskylä,Jyväskylä FI-40014,Finland Received 12 March 2016;revised 30 March 2016;accepted 2 April 2016 Available online 8 April 2016
Original article
Effect of aerobic exercise on insulin resistance and central adiposity disappeared after the discontinuation of intervention in overweight women
Shenglong Lea,Lijuan Maob,*,Dajiang Luc,*,Yifan Yanga,Xiao Tand,Petri Wiklundd,Sulin Chenga,c
aDepartment of Physical Education,Shanghai Jiao Tong University,Shanghai 200240,ChinabSchool of Physical Education and Training,Shanghai University of Sport,Shanghai 200438,ChinacSchool of Kinesiology,Shanghai University of Sport,Shanghai 200438,ChinadDepartment of Health Sciences,University of Jyväskylä,Jyväskylä FI-40014,Finland Received 12 March 2016;revised 30 March 2016;accepted 2 April 2016 Available online 8 April 2016
Abstract
Purpose:This study aimed to assess whether the benefits of exercise on central adiposity and insulin resistance(HOMA-IR)are maintained after discontinuation of intervention in the overweight/obese(OWOB)women.
Methods:The study subjects were from 2 independent studies with similar aerobic exercise(AE)intervention programs.In study I,15 OWOB postmenopausal women with pre-diabetes(body mass index,BMI=24-33 kg/m2,aged 52-65 years)completed an 8-month exercise intervention and were followed for 2 years after the intervention.In study II,12 OWOB(BMI=25-35 kg/m2,aged 30-50 years)premenopausal women participated in a 6-weekAE and were followed for 4 years after the intervention.The exercise program consisted of progressiveAE with intensity of 60%-75%of initial fitness level,30-60 min/time and 3-5 times/week.Fat mass(FM)was assessed by Dual Energy X-ray Absorptiometry (DXA Prodigy;study I)or bioelectrical impedance device(Inbody 720;study II).Plasma glucose and insulin were assessed by chemiluminescent immunoassay and HOMA-IR was calculated.
Results:Both 8-month and 6-week moderateAE were effective in reducing HOMA-IR(-18.9%,p=0.012 and-26.7%,p=0.046,respectively),and 8-month AE reduced FM at upper abdominal region(-6.2%,p=0.021).However,these improvements were not maintained in either study at the follow-up.
Conclusion:TheAE program used in these studies was effective to reduce insulin resistance and/or FM in central body region among overweight and obese women.However,when exercise intervention was discontinued,the beneficial effects following both short-and long-term intervention disappeared.Thus maintaining exercise seems to be required if one wants to reap the benefits of exercise in the long-term.
©2016 Production and hosting by Elsevier B.V.on behalf of Shanghai University of Sport.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Keywords:Exercise intervention;Obesity;Postmenopause;Premenopause;Relapse
1.Introduction
The current public health burdens caused by chronic disease cluster are associated with sedentary lifestyle and unbalanced diet.1Studies have shown that increasing individual levels of physical activity(PA)by exercise intervention is effective for reducing insulin resistance2-5and adiposity;6,7especially among populations with sedentary lifestyle and obesity.7However,such studies are still facing the challenge in terms of whether the subjects would maintain the PA level after the discontinuation of the organized exercise and whether the benefit gained from exercise intervention remained after intervention over time.
To date,the results of whether the benefit from exercise could remain after exercise intervention are still inconclusive. Some studies have shown that lifestyle intervention including exercise can prevent or delay progression to type 2 diabetes,4-12and thateffectspersisteven aftertheintervention is stopped.10-12These positive results are mainly from long-term interventions.However,other studies showed that the participants who initially lost weight following lifestyle interventions gradually regained weight by the end of intervention.7,13One ofthe main reasons for the loss of the health benefits from exercise is that weight loss is in a dose-response of exercise fashion.14One study has shown that more than half of the obese and diabetes patients involved in an exercise program did not maintain the same level of PA at 6 months after the intervention.15A decrease of exercise is accompanied with weight regain,even for those who have previously succeeded in loss their weight over time.16Therefore,relationships between organized exercise interventions,their cessation,and the maintenance(or lack of)long-term health benefits remain incompletely defined.
The present report aimed to address the following issue:when considering“ExerciseisMedicine”fordiseasessuchasimpaired glucosemetabolism,canthebenefitof“ExerciseisMedicine”on insulin resistance and central adiposity be maintained after discontinuation of interventions during prolonged follow-up?We reported outcomes based on 2 different studies.Both studies had used same exercise type and intensity;however with different duration of intervention in overweight/obese(OWOB)women.
2.Methods
2.1.Subjects
The study subjects were from 2 independent studies with similar aerobic exercise(AE)intervention program that were introduced elsewhere.17,18Briefly,for the purpose of this report,only those in the exercise group with both pre-intervention and follow-up assessment results were included.Study I included 15OWOB postmenopausalwomen (bodymassindex,BMI=24-33 kg/m2,aged 52-65 years)with pre-diabetes who have completed an 8-month exercise intervention and followed for 2 years.Study II consisted of 12 OWOB premenopausal women(BMI=25-35 kg/m2,aged 30-50 years)participated in a 6-week AE and followed for 4 years after onset of intervention.Studies I and II were approved by the Ethics Committee of Shanghai Institute of Nutrition(No.2013-003)and the Ethical Committee of Central Finland Health Care District(7/2011 OTE),respectively.Written informed consents were obtained from all subjects prior to the assessments.
2.2.Background information
Background information including medical history,current health status,and level of PA was collected via selfadministered questionnaires and was described elsewhere.17,18For this report,the level of PA in terms of hours and times per week was only considered unsupervised exercises because subjects participating in supervised exercise sessions was similar. The inactivity(IPA)was defined as amount of hours spent sitting and lying down including sleep per day.
2.3.Anthropometry and fat mass(FM)
Anthropometry and body composition were assessed in the morning after 12-h fasting.Height was determined using a wall-fixed measuring device,and body mass using a calibrated scale,and from these,BMI was calculated.In study I,a dualenergy X-ray absorptiometry(DXA Prodigy;GE Lunar Corp.,Madison,WI,USA)was used to estimate FM of the whole body and abdominal android and gynoid regions.Precision of the repeated measurements of FM expressed as coefficient of variation was on average 2.2%.In study II,a bioelectrical impedance analysis device(Inbody 720;Biospace Co.Ltd.,Seoul,Korea)was used for determining FM.Precision of the repeated measurements of FM expressed as coefficient of variation was on average 0.6%.
2.4.Insulin resistance
Venousbloodsamplesweretakeninstandardizedfastingconditions at 7:00-8:00 a.m.Plasma samples were used to assess glucose and insulin and explained in previous papers.17,18The homeostasis model assessment of insulin resistance(HOMA-IR)index was calculated as(fasting insulin concentration×fasting glucose concentration)/22.5.19
2.5.Exercise intervention
Both studies used the same exercise program.17Specifically,for exercise intervention,supervised exercise program(mainly aerobic exercise such as Nordic walking plus stretching and other group exercise)based on the recommendation for sedentary adults was implemented.20The supervised exercise program was progressive and variable and was monitored by an exercise researcher for 2 times a week during the course of the study.The other 1-3 times of unsupervised exercise sessions were performed by participants themselves according the instruction.The intensity of exercise was increased from 60% to 75%of the maximum oxygen uptake(estimated from fitness test)and the duration of exercise was increased from 30 to 60 min per session,and the frequency from 3 to 5 times a week. The exercise intensity was monitored by using heart rate monitor(M5;Suunto,Vantaa,Finland)in each supervised exercise session and monthly 1 time during unsupervised sessions. The exercise protocol was updated weekly in study I17and monthly in study II.18
3.Results
In study I,the changes of unsupervised participation in PA/IPA in terms of hours and times per week and hours per week in sitting and lying down,and body weight and FM are shown in Table 1.The unsupervised exercise sessions significantly increased during intervention(p<0.01)but reduced after the discontinuation of intervention.When taking into account the supervised sessions,the amount of exercise decreased after intervention at the 2 years follow-up.During the intervention,61.5%of the subjects increased the amount of unsupervised exercise and the remaining 38.5%did not change. After intervention,only 53.8%maintained their exercise participation as during intervention and the other 46.2%decreased their exercise time and frequency.
There were no significant changes in body weight and whole body and lower abdominal FM.Interestingly,the upper abdominal FM at the android region decreased significantly after intervention(-6.1%,p=0.021)but regained during the follow-up (12.8%,p<0.01,Fig.1D).The HOMA-IR decreased significantly after intervention(-18.9%,p=0.012)but attenuated during the follow-up(5.0%,p>0.05,Fig.1C).
A similar pattern was found in study II that after a short-term of 6-week AE,no significant changes were found in body weight and FM (Table 1),while HOMA-IR significantly decreased(-26.7%,p=0.046,Fig.2),but the benefit relapsed after 4 years(no significant difference between baseline and at the 4-year follow-up).

Table 1Body weight,fat mass,and physical activity/inactivity during aerobic exercise intervention and follow-up.
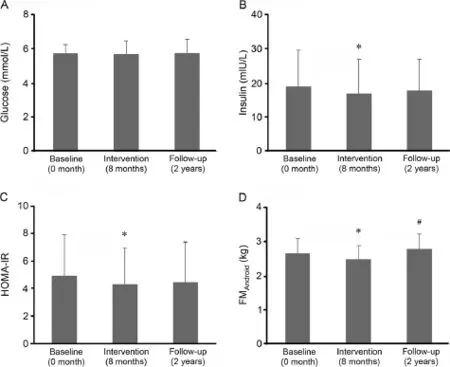
Fig.1.Comparison of glucose(A),insulin resistance(B-C),and central adiposity(D)during 8-month aerobic exercise intervention and 2-year follow-up in overweight/obese postmenopausal women with pre-diabetes(mean±SD).HOMA-IR=homeostasis model assessment of insulin resistance;FMAndroid=upper abdominal fat mass at the android region.*p<0.05,compared with baseline;#p<0.01,compared with 8-month intervention.
4.Discussion
Previous studies have shown that AE has not only a direct impact on body composition and weight6,7but also affects insulin resistance.2-4The results of the current report were in line with these studies.Our study further showed that in pre-or postmenopausal women,both short-and long-term AE were effective to improve the insulin resistance without significant change in body weight.In the long-term exercise intervention,body FM was lost from upper abdominal region. However,all the benefits were lost after discontinuation of the intervention.Thus the“medical effect”of AE on glucose metabolism13and reduction of central adiposity6,21would vanish if the“exercise medication”is stopped.
In study I,with 8-monthAE intervention and 2-year followup,over 60%of the participants increased their amount of exercise time and frequency during intervention regardless of the supervised part of exercise sessions,while about half of the participants decreased their amount of exercise time and frequency after intervention.The reduction in amount of exercise is likely to be the main reason for the relapsing of the benefits from exercise in insulin resistance and regain in central adiposity.Previous studies showed that more than half of the subjectsdid not maintain their level of PA after exercise interventions stopped.15,16Together,these results indicate that changing lifestyle from sedentary to active and maintaining the active lifestyle is needed to support long-term benefits.
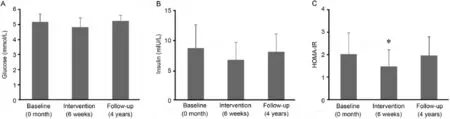
Fig.2.Comparison of glucose(A)and insulin resistance(B-C)during 6-week aerobic exercise intervention and 4-year follow-up in overweight/obese premenopausal women(mean±SD).HOMA-IR=homeostasis model assessment of insulin resistance.*p<0.05,compared with baseline value.
The other interesting finding in the report is that there was no significant weight loss in both studies.The body weight kept relatively stable even after 4 years.Early study showed that a short-term(4 weeks)AE decreased hepatic and visceral lipids without weight loss in previously sedentary obese men and premenopausal women.22In our short-term exercise intervention study,we did not measure the central abdominal fat mass,thus we cannot know whether such short-term exercise could reduce the central adiposity.However,with 8-month AE intervention,central body FM declined significantly albeit without noticeable changes in body weight and whole body FM.These results indicate that short-term AE can mitigate metabolic risk and it may not be contingent of weight loss.Nonetheless,the regain of FM was even more substantial with 12.8%regain after intervention stopped.This observation is in agreement with a previous study which showed that reduction of level of PA would induce weight loss rebound.23
Despite similar observations from both studies,we acknowledged the sample sizes for both studies are relatively small and cannot entirely rule out type II error.However,the advantage of this report lies on the fact that the studies’subjects are from 2 completely populations.The results from one study could be considered as validation for another study.In addition,the exercise programs used in both studies are the same in type and intensity albeit with different duration.This indicates that the health benefit already can be reached even with a short-term of 6 weeks exercise,i.e.,longer programs are not required to reap benefits.This result,to some extent,could encourage participants to keep on with interventions since the most difficult lifestyle intervention is sustaining in the beginning for overweight/obese people.24Nonetheless,as we have robustly shown in the present 2 intervention/follow-up studies,maintenance of PA long-term is needed to sustain these benefits.
To sum up,aerobic exercise is effective to reduce insulin resistance and central body FM without noticeable whole body weight loss(albeit some shifts in body composition with long-term AE).However,when exercise is discontinued,the beneficial effects are lost both short-term in premenopausal and long-term in postmenopausal women.Thus maintaining exercise seems to be required if one wants to reap the benefits of exercise in the long-term.
Acknowledgments
This study was financially supported by the China State Sport General Administration(No.2013B040,2015B039),the University of Jyväskylä Wellness program and the Shanghai Jiao Tong University Zhiyuan Foundation(No.CP2014013). We would like to thank the researchers involved in both studies for their valuable work and technical assistance on this project.
Authors’contributions
SLconceivedofanddesignedtheexperiments,performedthe experiments,analyzed the data,contributed reagents/materials/ analysis tools,and drafted the manuscript.LM conceived of and designed the experiments,performed the experiments,and drafted the manuscript.DL conceived of and designed the experiments and performed the experiments.YY performed the experiments,analyzed the data and contributed reagents/ materials/analysis tools.XT performed the experiments,analyzedthedata,andcontributedreagents/materials/analysistools. PW performed the experiments and analyzed the data.SC conceived of and designed the experiments,performed the experiments,analyzedthedata,anddraftedthemanuscript.Allauthors have read and approved the final version of the manuscript and agree with the order of presentation of the authors.
Competing interests
None of the authors declare competing financial interests.
References
1.Halpin HA,Morales-Suárez-Varela MM,Martin-Moreno JM.Chronic disease prevention and the new public health.Public Health Rev 2010;32:120-54.
2.Kadoglou NPE,Iliadis F,Sailer N,Athanasiadou Z,Vitta I,Kapelouzou A,et al.Exercise training ameliorates the effects of rosiglitazone on traditional and novel cardiovascular risk factors in patients with type 2 diabetes mellitus.Metabolism 2010;59:599-607.
3.Desch S,Sonnabend M,Niebauer J,SixtS,SarebanM,EitelI,etal.Effects of physical exercise versus rosiglitazone on endothelial function in coronary artery disease patients with prediabetes.Diabetes Obes Metab 2010;12:825-8.
4.Sénéchal M,Slaght J,Bharti N,Bouchard DR.Independent and combined effect of diet and exercise in adults with prediabetes.Diabetes Metab Syndr Obes 2014;7:521-9.
5.Tuomilehto J,Lindstrom J,Eriksson JG,Valle TT,Hamalainen H,Ilanne-Parikka P,et al.Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance.N Engl J Med 2001;344:1343-50.
6.Yaffe MJ.Adiposity changes after a 1-year aerobic exercise intervention among postmenopausal women:a randomized controlled trial.Int J Obes (Lond)2010;35:427-35.
7.Sarwer DB,Amy VSG,Vetter ML,Wadden TA.Behavior therapy for obesity:where are we now?Curr Opin Endocrinol Diabetes Obes 2009;16:347-52.
8.Ramachandran A,Snehalatha C,Mary S,Mukesh B,Bhaskar AD,Vijay V. TheIndian DiabetesPrevention Programme showsthatlifestyle modification and metformin prevent type 2 diabetes in Asian Indian subjects with impaired glucose tolerance(IDPP-1).Diabetologia 2006;49: 289-97.
9.Kosaka K,Noda M,Kuzuya T.Prevention of type 2 diabetes by lifestyle intervention:a Japanese trial in IGT males.Diabetes Res Clin Pract 2005;67:152-62.
10.Diabetes Prevention Program Research Group,Knowler WC,Fowler SE,Hamman RF,Christophi CA,Hoffman HJ,et al.10-year follow-up of diabetes incidence and weight loss in the Diabetes Prevention Program Outcomes Study.Lancet 2009;374:1677-86.
11.Li G,Zhang P,Wang J,Gregg EW,Yang W,Gong Q,et al.The long-term effect of lifestyle interventions to prevent diabetes in the China Da Qing Diabetes Prevention Study:a 20-year follow-up study.Lancet 2008;371: 1783-9.
12.Lindström J,Ilanne-Parikka P,Peltonen M,Aunola S,Eriksson JG,Hemiö K,et al.Sustained reduction in the incidence of type 2 diabetes by lifestyle intervention:follow-up of the Finnish Diabetes Prevention Study.Lancet 2008;22:1673-9.
13.Sanz C,Gautier JF,Hanaire H.Physical exercise for the prevention and treatment of type 2 diabetes.Diabetes Metab 2010;36:346-51.
14.Amati F,Barthassat V,Miganne G,Hausman I,Monnin DG,Costanza MC,et al.Enhancing regular physical activity and relapse prevention through a 1-day therapeutic patient education workshop:a pilot study. Patient Educ Couns 2007;68:70-8.
15.King H,Kriska AM.Prevention of type II diabetes by physical training. Epidemiological considerations and study methods.Diabetes Care 1992;15:1794-9.
16.McGuire MT,Wing RR,Klem ML,Lang W,Hill JO.What predicts weight regain in a group of successful weight losers?J Consult Clin Psychol 1999;67:177-85.
17.Wiklund P,Alen M,Munukka E,Cheng M,Yu B,Pekkala S,et al. Metabolic response to 6-week aerobic exercise training and dieting in previously sedentary overweight and obese pre-menopausal women: a randomized trial.J Sport Health Sci 2014;3:217-24.
18.Liu WY,Lu da J,Du XM,Sun JQ,Ge J,Wang RW,et al.Effect of aerobic exercise and low carbohydrate diet on pre-diabetic non-alcoholic fatty liver disease in postmenopausal women and middle aged men—the role of gut microbiota composition:study protocol for the AELC randomized controlled trial.BMC Public Health 2014;14:48.doi:10.1186/1471 -2458-14-4
19.Blomain ES,Dirhan DA,Valentino MA,Kim GW,Waldman SA. Mechanisms of weight regain following weight loss.ISRN Obes 2013;2013:210524.doi:10.1155/2013/210524
20.Garber CE,Blissmer B,Deschenes MR,Franklin BA,Lamonte MJ,Lee IM,et al.,American College of Sports Medicine.American College of Sports Medicine position stand.Quantity and quality of exercise for developing and maintaining cardiorespiratory,musculoskeletal,and neuromotor fitness in apparently healthy adults:guidance for prescribing exercise.Med Sci Sports Exerc 2011;43:1334-59.
21.Friedenreich CM,Neilson HK,O’Reilly R,Duha A,Yasui Y,Morielli AR,et al.Effects of a high vs moderate volume of aerobic exercise on adiposity outcomes in postmenopausal women:a randomized clinical trial.JAMA Oncol 2015;1:766-76.
22.Johnson NA,Sachinwalla T,Walton DW,Smith K,Armstrong A,Thompson MW,et al.Aerobic exercise training reduces hepatic and visceral lipids in obese individuals without weight loss.Hepatology 2009;50:1105-12.
23.Jakicic JM,Marcus BH,Lang W,Janney C.Effect of exercise on 24-month weight loss maintenance in overweight women.Arch Intern Med 2008;168:1550-9,discussion 1559-60.
24.Yackobovitch-Gavan M,Steinberg DM,Endevelt R,Benyamini Y.Factors associated with dropout in a group weight-loss programme:a longitudinal investigation.J Hum Nutr Diet 2015;28(Suppl.2):S33-40.
Peer review under responsibility of Shanghai University of Sport. *Corresponding authors.
E-mailaddress:maolijuan@sus.edu.cn (L.Mao);ludajiang2000@ aliyun.com(D.Lu).
http://dx.doi.org/10.1016/j.jshs.2016.04.003
2095-2546/©2016 Production and hosting by Elsevier B.V.on behalf of Shanghai University of Sport.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
杂志排行

Journal of Sport and Health Science的其它文章
- Exercise is recreation not medicine
- High-intensity interval training(HIIT)for patients with chronic diseases
- The role of physical activity and exercise in obesity and weight management:Time for critical appraisal
- Targeting mitochondrial phenotypes for non-communicable diseases
- Exercise is more than medicine:The working age population’s well-being and productivity
- Beneficial effects of fenugreek glycoside supplementation in male subjects during resistance training:A randomized controlled pilot study