Circulating microRNAs as potential biomarkers for diagnosis of congenital heart defects
2016-07-08WanqinXieLinZhouYongChenBinNiFamilyPlanningResearchInstituteofHunanProvinceChangsha410126ChinaCorrespondingAuthorBinNiEmailnibinjss126com
Wan-qin Xie, Lin Zhou, Yong Chen, Bin NiFamily Planning Research Institute of Hunan Province, Changsha 410126, ChinaCorresponding Author: Bin Ni, Email: nibinjss@126.com
Review Article
Circulating microRNAs as potential biomarkers for diagnosis of congenital heart defects
Wan-qin Xie, Lin Zhou, Yong Chen, Bin Ni
Family Planning Research Institute of Hunan Province, Changsha 410126, China
Corresponding Author: Bin Ni, Email: nibinjss@126.com
BACKGROUND: MicroRNAs are small non-coding RNAs of approximately 22 nucleotides in length, and play important regulatory roles in normal heart development and the pathogenesis of heart diseases. Recently, a few prospective studies have implicated the diagnostic role of microRNAs in congenital heart defects (CHD).
DATA RESOURCES: This review retrieved the research articles in PubMed focusing on the altered microRNAs in cardiac tissue or serum of patients with CHD versus healthy normal controls, as well as the studies exploring circulating microRNAs as potential biomarkers for (fetal) CHD.
RESULTS: Most of the studies of interest were conducted in recent years, implicating that the topic in this review is a newly emerging field and is drawing much attention. Moreover, a number of differentially expressed microRNAs between CHD specimens and normal controls have been reported.
CONCLUSION: Circulating microRNAs may serve as potential biomarkers for diagnosis of CHD in the future, with more efforts paving the road to the aim.
KEY WORDS:Congenital heart defects; Biomarkers; MicroRNA
World J Emerg Med 2016;7(2):85–89
INTRODUCTION
Congenital heart defects/diseases (CHD) refer to a broad range of heart development anomalies. Tetralogy of Fallot (TOF), ventricular septal defects (VSD), and atrial septal defects (ASD) are the most common CHD for newborn; other defects such as transposition of the great arteries (TGA) are less commonly seen. Congenital heart defects affect approximately 1% of live births,and are the leading cause of infant deaths.[1–4]Hence,early diagnosis of fetal CHD is of great signifi cance for timely postnatal surgical intervention or termination of pregnancy.[5,6]Accordingly, novel biomarkers for the improvement of efficiency and accuracy in the diagnosis of fetal CHD are needed in combination with conventional fetal echocardiography.[7,8]In the new era of non-invasive prenatal tests, potential biomarkers such as microRNAs,[9,10]proteins,[11]and the merging fetal cells[12]in maternal circulation that will cause minimum risk to fetus are easily accepted.[13]
MicroRNAs are a class of non-coding RNAs of approximately 22 nucleotides in length.[14]The posttranslational regulatory roles of microRNAs have been shown in almost all physiological processes via non-precise complementary binding to the 3'un-translated region of target mRNA, which results in translation repression or mRNA degradation.[14]Taking advantage of the remarkable stability of microRNAs in serum and body fluids[15]and the dysregulated expression of microRNAs under disease conditions,[16]many studies have proposed microRNAs as diagnostic and prognostic biomarkers.[17,18]
Recently, a few prospective studies have revealed the altered expression of microRNAs in heart tissue/ plasma of patients with CHD versus CHD-free controls (Table 1). These studies have highlighted the potential of circulating microRNAs as biomarkers for diagnosis of (fetal) CHD, and thus they are listed and discussed in this review.
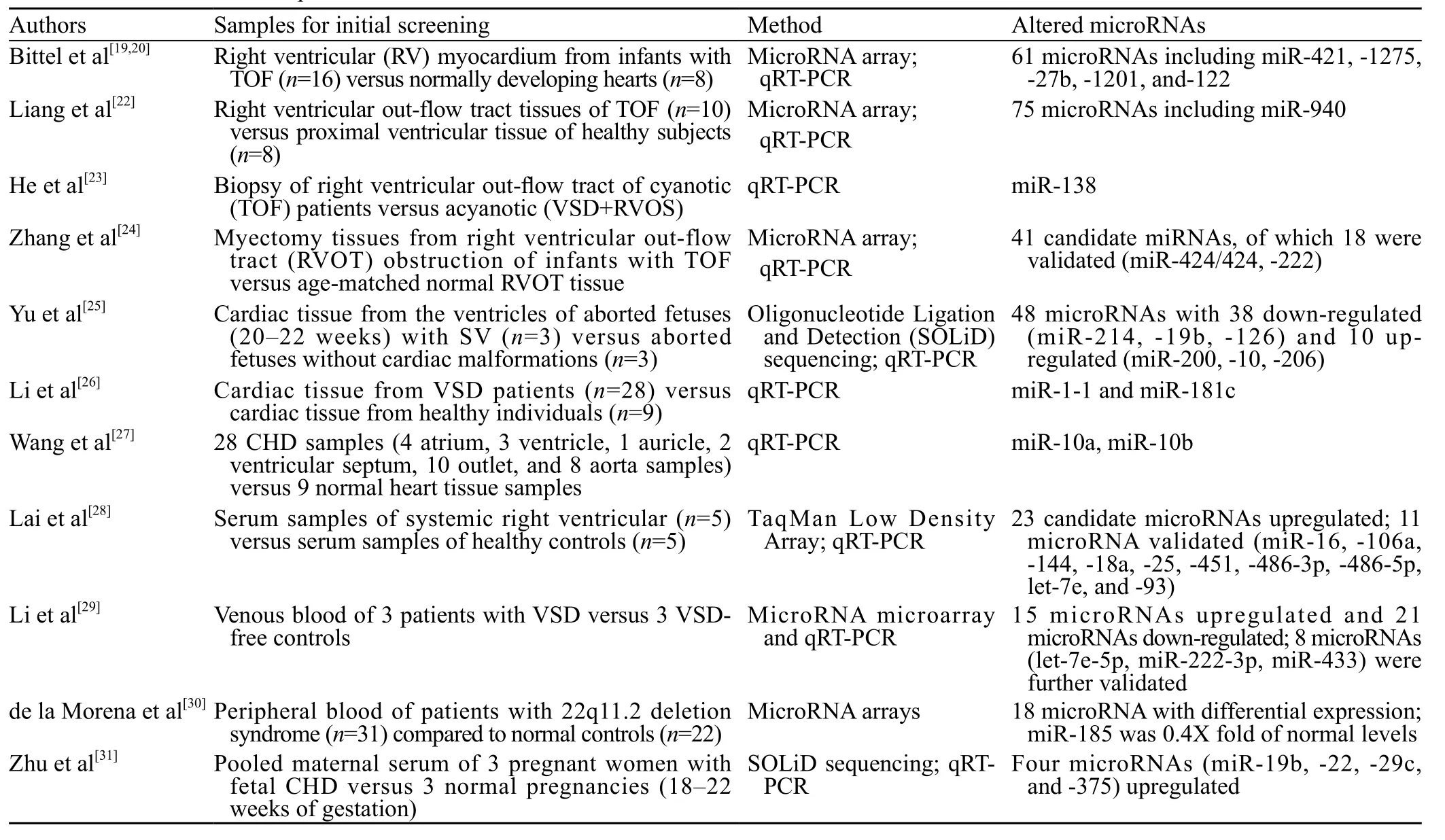
Table 1. Publications with respect to microRNAs in heart tissue/plasma of patients with CHD
Altered microRNAs in cardiac tissue of CHD Altered microRNAs in Tetralogy of Fallot
Tetralogy of Fallot is one of the most common CHD characterized by severe heart malformations. O'Brien and colleagues[19]performed microarray analyses to screen microRNAs differentially expressed in the right ventricular myocardium of infants with non-syndromic TOF (without a 22q11.2 deletion) compared with infants with normally developing hearts. Results showed that the levels of 61 microRNAs significantly changed and miR-1275, miR-27b, miR-421, miR-1201, and miR-122 exhibited the most appreciable alterations. Their followup studies focused on miR-421. By knocking down and over-expressing miR-421 in primary cells derived from the right ventricular of TOF heart, the authors found an inverse correlation between the level of miR-421 and that of SOX4.[20]As a key regulator in Notch pathway,SOX4 affects the cardiac outfl ow track.[21]Therefore, the interplay between miR-421 and SOX4 possibly suggests the association of miR-421 with congenital heart defects.
MiR-940 is another microRNA that has been associated with TOF. Liang et al[22]identified 75 dysregulated microRNAs in TOF tissue relative to heart tissue of healthy subjects. Among the 75 microRNAs,miR-940 was the most down-regulated one.[22]Mechanism studies showed that miR-940 negatively regulates the proliferation and migration of human cardiomyocyte progenitor cells, possibly via modulating the endogenous level of JARID2.[22]
He et al[23]studied miR-138, a microRNA involved in hypoxia response of cardiomyocytes. They showed that the expression of miR-138 in myocardial samples of patients in the cyanotic group (TOF) was as almost two-fold as that of patients in the acyanotic group (VSD combined with RVOS).[23]This finding suggests that miR-138 might be used to discriminate TOF from other subtypes of CHD.
Zhang and colleagues[24]initially identified 41 candidate microRNAs with differential expression between TOF tissue and normal heart tissue. After validation in another independent population of patients with TOF, 18 out of the 41 microRNAs were found to have significant alterations at their expression levels.[24]In the study, miR-424/424*and miR-222 were shown to affect cardiomyocyte proliferation and differentiation.[24]
MicroRNAs associated with ventricular defects
Yu et al[25]profi led the microRNAs in cardiac tissue of aborted fetus with single ventricle defects (VD) by using deep sequencing. As a result, 48 microRNAswere identified with differential expression in VD tissue compared with normal cardiac tissue. Of these microRNAs, 38 microRNAs were downregulated, and 10 microRNAs were upregulated. The increase of miR-214,miR-19b, and miR-126 and decrease of miR-200, miR-10, and miR-206 were further confirmed by qRT-PCR analysis.[25]
Li et al[26]selected a set of 25 candidate microRNAs based on the initial microarray data and analyzed the relative levels of the microRNAs in heart tissue of patients with ventricular septal defects (VSD) to those in heart tissue of healthy controls by using qRT-PCR. They found that miR-1-1 and miR-181c were the most differentially expressed microRNAs for their samples. Moreover, they showed that the decrease of miR-1-1 expression was associated with the increased levels of GJA1 and SOX9, and that the increased miR-181c expression was linked with the down-regulation of BMPR2 in VSD samples.[26]
MiR-10a and miR-10b in CHD
Wang et al[27]first found that TBX5, which is a key transcription factor playing a role in heart development,was a target gene of both miR-10a and miR-10b. This finding encouraged them to determine the miR-10a and miR-10b expression levels in heart tissues of CHD relative to healthy controls. Results showed that the average levels of miR-10a and miR-10b in heart tissue of CHD (n=28) were as approximately 3-fold high as those in controls (n=9).[27]However, the subtypes of heart defects were not specified in this study. A stratification analysis on the expression levels of miR-10a and miR-10b in terms of the subtypes of heart defects would be of more pathobiological signifi cance.
Circulating microRNAs as potential biomarkers for diagnosis of CHD
Altered circulating microRNAs in patients with CHD
The potential of circulating microRNAs as biomarkers for diagnosis and prognosis of patients with CHD has drawn attention. Lai et al[28]did the prof iling of circulating microRNAs of serum samples from 5 patients late after atrial switch operation for complete transposition of the great arteries (TGA) and 5 healthy controls, which resulted in 23 microRNAs identified with differential expression between the two groups. Subsequent validation in 26 patients and 20 controls confirmed the up-regulation of 11 of the 23 microRNAs.[28]
In the study by Li et al,[29]microRNA array initially was employed to determine the differential microRNAs between 3 patients with VSD and 3 VSD-free controls,which yielded a total of 36 candidate microRNAs, of which 15 were upregulated and 21 downregulated. The results of subsequent validation experiment confi rmed the up-regulation of miR-498 and down-regulation of miR-let-7e-5p, miR-155-5p, miR-222-3p, miR379-5p, miR-433,and miR-487b, and miR-409-3p in plasma samples of patients (n=20) compared with the controls (n=15).[29]
By using microRNA array, de la Morena and colleagues[30]showed that 18 microRNAs were differentially expressed in peripheral blood of patients with CHD (associated with 22q11.2 deletion syndrome) relative to normal controls. The level of miR-185 in patient blood was found to be about 0.4 fold of normal level.[30]
Characteristic circulating microRNAs in maternal plasma of pregnant women with fetal CHD
Zhu and colleagues[31]first reported the study using circulating microRNAs for prenatal prediction of fetal CHD. In their discovery experiment, maternal serum samples of 3 pregnant women with fetal CHD were pooled, as well as the control serum samples (n=3),to screen the differential microRNAs. Eventually, 4 microRNAs (miR-19b, miR-22, miR-29c, and miR-375) were found to be elevated in maternal plasma of pregnant women with fetal CHD.[31]This study highlights the potential of circulating microRNAs as biomarkers in non-invasive prenatal test for fetal CHD.
Limitations and future studies
Congenital heart defects include a series of heart development malformations. The etiology of CHD is complex and remains largely unknown.[1,32]This review concentrated a series of pilot studies exploring the differentially expressed microRNAs in cardiac tissue or plasma of patients with (fetal) CHD compared with the normal healthy controls. The altered microRNAs identifi ed might become biomarkers for diagnosis of CHD in the future.[18,33]Meantime, the regulatory network and signaling pathways implicated by the altered microRNAs provide new insights into our understanding of CHD.
However, so far, we perhaps have just seen the tip of the iceberg, because we have little knowledge about the profiles of microRNAs in other subtypes of CHD rather than TOF and ventricular septal defects. Further,the altered microRNAs are quite heterogeneous between the studies, even the studies of the same subtype of heart defects (TOF or VSD). This may faithfully reflect the complex etiology of CHD and the great heterogeneitybetween patients with CHD, or technically be caused by the small sample size of patient pool for initial screening in these studies. There is a possibility that the microRNAs screened were biased by patients' age,gender, and category of heart defects, complications associated with CHD, or other factors, in particular when the initial sample size was very small. Additionally, it should be noted that the cardiac tissue and maternal blood samples in most of the studies are of Chinese (Asian) genetic background. Therefore, more studies are anticipated in a diverse set of ethnic backgrounds. The observations from diversified genetic backgrounds are necessary for discovery of microRNAs that will be applied to a broad range of ethnic populations. Meantime,more efforts are called for searching reliable microRNA biomarkers for CHD. The performance of candidate microRNAs should be evaluated strictly in large populations of patients and controls. We can expect that one microRNA may not give the best performance for prediction. However, a comprehensive evaluation via a panel of microRNA biomarkers is feasible and acceptable.
It is easily understood that verification of the existence of fetus microRNA in maternal circulation will support the use of maternal circulating microRNAs as biomarkers for diagnosis of fetal CHD. Actually, it has been reported that placental microRNAs can be detected in maternal circulation.[15]Therefore, the fetal microRNAs that are indicative of CHD might be released into maternal circulation and captured for analysis. Alternatively, the microRNAs could be maternally originated, but they might serve as biomarkers for fetal CHD with high sensitivity and specifi city.
In a "new era" of microRNAs, the pathobiology of microRNAs in CHD is being extensively investigated. We believe this will greatly add new knowledge to the etiology of CHD and also promote the development of circulating microRNAs as biomarkers for diagnosis of CHD and prenatal screening.
Funding: None.
Ethical approval: Not needed.
Conflicts of interest: The authors declare there is no competing interest related to the study, authors, other individuals or organizations. Contributors: Xie WQ proposed the study and wrote the first draft. All authors read and approved the fi nal version of the paper.
REFERENCES
1 Bruneau BG, Srivastava D. Congenital heart disease: entering a new era of human genetics. Circ Res 2014; 114: 598–599.
2 Hoffman JI, Kaplan S. The incidence of congenital heart disease. J Am Coll Cardiol 2002; 39: 1890–1900.
3 Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ,Cushman M, et al. Heart disease and stroke statistics–2015 update: a report from the American Heart Association. Circulation 2015; 131: e29–322.
4 van der Linde D, Konings EE, Slager MA, Witsenburg M,Helbing WA, Takkenberg JJ, et al. Birth prevalence of congenital heart disease worldwide: a systematic review and meta-analysis. J Am Coll Cardiol 2011; 58: 2241–2247.
5 Panni RZ, Ashfaq A, Amanullah MM. Earlier surgical intervention in congenital heart disease results in better outcome and resource utilization. BMC Health Serv Res 2011; 11: 353.
6 Tararbit K, Bui TT, Lelong N, Thieulin AC, Goffinet F,Khoshnood B. Clinical and socioeconomic predictors of pregnancy termination for fetuses with congenital heart defects: a population-based evaluation. Prenat Diagn 2013; 33: 179–186.
7 Liu H, Zhou J, Feng QL, Gu HT, Wan G, Zhang HM, et al. Fetal echocardiography for congenital heart disease diagnosis: a metaanalysis, power analysis and missing data analysis. Eur J Prev Cardiol 2015; 22: 1531–1547.
8 van Velzen CL, Clur SA, Rijlaarsdam ME, Pajkrt E, Bax CJ,Hruda J, et al. Prenatal diagnosis of congenital heart defects;accuracy and discrepancies in a multi-center cohort. Ultrasound Obstet Gynecol. 2015 Sep 9. doi: 10.1002/uog.15742. [Epub ahead of print]
9 Lim JH, Lee da E, Kim SY, Kim HJ, Kim KS, Han YJ, et al. MicroRNAs as potential biomarkers for noninvasive detection of fetal trisomy 21. J Assist Reprod Genet 2015; 32: 827–837.
10 Tsochandaridis M, Nasca L, Toga C, Levy-Mozziconacci A. Circulating microRNAs as clinical biomarkers in the predictions of pregnancy complications. Biomed Res Int 2015;2015: 294954.
11 Yao Y, Jiang Y, Han M, Xia Y, He Y, Wang Y, et al. Screening and identifi cation of potential predictive biomarkers for Down's syndrome from second trimester maternal serum. Expert Rev Proteomics 2015; 12: 97–107.
12 Hatt L, Brinch M, Singh R, Moller K, Lauridsen RH, Schlutter JM, et al. A new marker set that identifi es fetal cells in maternal circulation with high specifi city. Prenat Diagn 2014; 34: 1066–1072.
13 Rose NC, Eller AG. The impact of noninvasive fetal evaluation: its effect on education, training, and the maintenance of clinical competence in prenatal diagnosis. Curr Opin Obstet Gynecol 2014; 26: 117–123.
14 Ameres SL, Zamore PD. Diversifying microRNA sequence and function. Nat Rev Mol Cell Biol 2013; 14: 475–488.
15 Chim SS, Shing TK, Hung EC, Leung TY, Lau TK, Chiu RW,et al. Detection and characterization of placental microRNAs in maternal plasma. Clin Chem 2008; 54: 482–490.
16 Thum T, Condorelli G. Long noncoding RNAs and microRNAs in cardiovascular pathophysiology. Circ Res 2015; 116: 751–762.
17 He Y, Lin J, Kong D, Huang M, Xu C, Kim TK, et al. Current state of circulating microRNAs as cancer biomarkers. Clin Chem 2015; 61: 1138–1155.
18 Kondkar AA, Abu-Amero KK. Utility of circulating microRNAs as clinical biomarkers for cardiovascular diseases. Biomed Res Int 2015; 2015: 821823.
19 O'Brien JE Jr, Kibiryeva N, Zhou XG, Marshall JA, Lofl and GK,Artman M, et al. Noncoding RNA expression in myocardium from infants with tetralogy of Fallot. Circ Cardiovasc Genet 2012; 5: 279–286.
20 Bittel DC, Kibiryeva N, Marshall JA, O'Brien JE. MicroRNA-421 dysregulation is associated with tetralogy of fallot. Cells 2014; 3: 713–723.
21 Schilham MW, Oosterwegel MA, Moerer P, Ya J, de Boer PA, van de Wetering M, et al. Defects in cardiac outflow tract formation and pro-B-lymphocyte expansion in mice lacking Sox-4. Nature 1996; 380: 711–714.
22 Liang D, Xu X, Deng F, Feng J, Zhang H, Liu Y, et al. miRNA-940 reduction contributes to human Tetralogy of Fallot development. J Cell Mol Med 2014;18: 1830–1839.
23 He S, Liu P, Jian Z, Li J, Zhu Y, Feng Z, et al. miR-138 protects cardiomyocytes from hypoxia-induced apoptosis via MLK3/ JNK/c-jun pathway. Biochem Biophys Res Commun 2013; 441: 763–769.
24 Zhang J, Chang JJ, Xu F, Ma XJ, Wu Y, Li WC, et al. MicroRNA deregulation in right ventricular outflow tract myocardium in nonsyndromic tetralogy of fallot. Can J Cardiol 2013; 29: 1695–1703.
25 Yu ZB, Han SP, Bai YF, Zhu C, Pan Y, Guo XR. microRNA expression profiling in fetal single ventricle malformation identifi ed by deep sequencing. Int J Mol Med 2012; 29: 53–60.
26 Li J, Cao Y, Ma XJ, Wang HJ, Zhang J, Luo X, et al. Roles of miR-1-1 and miR-181c in ventricular septal defects. Int J Cardiol 2013; 168: 1441–1446.
27 Wang F, Yang XY, Zhao JY, Yu LW, Zhang P, Duan WY, et al. miR-10a and miR-10b target the 3'-untranslated region of TBX5 to repress its expression. Pediatr Cardiol 2014; 35: 1072–1079.
28 Lai CT, Ng EK, Chow PC, Kwong A, Cheung YF. Circulating microRNA expression profile and systemic right ventricular function in adults after atrial switch operation for complete transposition of the great arteries. BMC Cardiovasc Disord 2013;13: 73.
29 Li D, Ji L, Liu L, Liu Y, Hou H, Yu K, et al. Characterization of circulating microRNA expression in patients with a ventricular septal defect. PloS One 2014; 9: e106318.
30 de la Morena MT, Eitson JL, Dozmorov IM, Belkaya S, Hoover AR, Anguiano E, et al. Signature microRNA expression patterns identifi ed in humans with 22q11.2 deletion/DiGeorge syndrome. Clin Immunol 2013; 147: 11–22.
31 Zhu S, Cao L, Zhu J, Kong L, Jin J, Qian L, et al. Identifi cation of maternal serum microRNAs as novel non-invasive biomarkers for prenatal detection of fetal congenital heart defects. Clin Chim Acta 2013; 424: 66–72.
32 Bruneau BG. The developmental genetics of congenital heart disease. Nature 2008; 451: 943–948.
33 Li M, Zhang J. Circulating microRNAs: potential and emerging biomarkers for diagnosis of cardiovascular and cerebrovascular diseases. Biomed Res Int 2015; 2015: 730535.
Received Ocotber 26, 2015
Accepted after revision March 20, 2016
DOI:10.5847/wjem.j.1920–8642.2016.02.001
杂志排行
World journal of emergency medicine的其它文章
- Evaluation of preventable trauma death in emergency department of Imam Reza hospital
- Application of scoring systems with point-of-care ultrasonography for bedside diagnosis of appendicitis
- A scoring system for assessing the severity of acute diarrhea of adult patients
- Emergency medicine providers' opioid prescribing practices stratifi ed by gender, age, and years in practice
- Instructions for Authors
- An incidental case of Wellens' syndrome in a community emergency department