移植肾急性排斥扩散加权成像早期诊断价值
2016-06-27梁世伟黄海波黄桂雄管俊杨建钧刘旭阳
梁世伟,黄海波,黄桂雄,管俊,杨建钧,刘旭阳
移植肾急性排斥扩散加权成像早期诊断价值
梁世伟1,黄海波2*,黄桂雄2,管俊2,杨建钧3,刘旭阳4
[摘要]目的 探讨移植肾急性排斥扩散加权成像早期诊断价值。材料与方法 应用3.0 T MR扩散加权成像序列(b=0、100、800 s/mm2),分别扫描原位正常肾51例(A组)、移植正常肾22例(B组)、急性排斥反应移植肾15例(C组)志愿者,数据导入自带工作站处理获得3组肾皮质、髓质、肌肉的表观扩散系数(apparent diffusion coefficient, ADC0-800)。比较原位肾组皮髓质ADC0-800值双侧差异,两组正常肾皮质与髓质差异,3组年龄、性别间以及肌肉、肾皮质、髓质ADC0-800值差异,以活检病理为“金标准”,评价肾皮质ADC0-800值诊断移植肾急性排斥效能。结果 3组间年龄、性别、肌肉ADC0-800值无统计学差异(P>0.05);原位肾皮髓质ADC0-800值双侧差异无统计学意义(P>0.05);正常肾皮质ADC0-800值高于髓质,差异有统计学意义(P<0.05);3组间肾皮质ADC0-800值差异有统计学意义(P<0.05),两两比较C组与A、B组间均有统计学差异(P<0.05),A组与B组间差异无统计学意义(P>0.05);髓质ADC值3组间无统计学差异(P>0.05)。以病理为标准,取1.76×10–3mm2/s为阈值,皮质ADC0-800值诊断急性排斥移植肾受试者工作特征曲线下面积为0.942,敏感度与特异性分别为86.7%和90.4%。结论 磁共振扩散加权成像对移植肾急性排斥早期诊断具有较高价值。
[关键词]肾移植;移植物排斥;弥散磁共振成像;扩散加权成像
作者单位:1. 武警广西总队医院放射科,南宁530003 2. 解放军第303医院医学影像科,南宁 530021 3. 解放军第303医院病理科,南宁530021 4. 解放军第303医院移植科,南宁530021
接受日期:2015-12-23
梁世伟, 黄海波, 黄桂雄, 等. 移植肾急性排斥扩散加权成像早期诊断价值.磁共振成像, 2016, 7(2): 90–95.
*Correspondence to: Huang HB, E-mail: jackie000528@163.com
Received 1 Nov 2015, Accepted 23 Dec 2015
ACKNOWLEDGMENTS This work was part of Guangxi scientific research and technology development project (No. GUIKEGONG1298003-8-6).
移植肾急性排斥是指供肾携带的异体抗原引起的受体内发生的免疫反应,细胞免疫类型在临床上最常见,通常术后4天至2周发生,病理组织学以大量单核和淋巴细胞浸润为特征,可通过激素冲击逆转大多数病例。急性排斥不仅是术后肾损害最常见和最重要的并发症,也是慢性排斥和功能丧失、缩短移植肾生存期的重要原因[1],因此急性排斥早期诊断具有重要意义。活检病理学作为急性排斥诊断金标准是一项有创性检查,且存在穿刺出血、破裂、感染、不易耐受等不足[2-3]。而临床血肌酐水平评估肾急性排斥亦无法达到早期、准确的诊断目的,因为该项指标只有明显组织损伤才升高[4]。因此找寻一种高敏感度和特异性的无创技术实现急性排斥早期诊断,一直为移植肾及相关医学研究所关注。笔者拟通过扩散加权成像扫描原位肾、移植正常肾和急性排斥移植肾3组志愿者,探索表观扩散系数(apparent diffusion coefficient, ADC)在移植肾急性排斥早期诊断的价值。
1 材料与方法
1.1志愿者资料
选取2012年4月至2014年10月于解放军第303医院医学影像科申请肾扫描原位正常肾51例(A组),男35例、女16例,年龄18~55岁,平均(34.9±10.9)岁;移植正常肾22例(B组),男16例、女6例,年龄16~57岁,平均(35.9±11.4)岁;急性排斥移植肾15例(C组),男10例、女5例,年龄25~53岁,平均(35.5±5.6)岁为志愿者入组研究。入组标准:原位正常肾无临床症状,血肌酐、尿素氮及超声无阳性指征;移植正常肾满足术后3个月至5年,余标准同原位肾;急性排斥移植肾为术后1周~4周,临床低热、全身不适及尿量进行性减少,血肌酐>186.0 μmol/L、尿素氮>7.14 mmol/L并MR扫描后至治疗前经穿刺活检证实。研究实验获我院伦理委员会批准,志愿者知情并签署同意书。
1.2设备与方法
Philips Achieva 3.0 T TX MR扫描仪,使用SENSE XL TORSO 16 coils配合呼吸门控,扫描前严格匀场和参考扫描,扫描序列包括横断位T1WI、T2WI、扩散加权成像(diffusion weighted imaging, DWI)与冠状T2WI,扫描20层,5 mm/层,间隔0.5 mm,DWI序列扩散敏感梯度场在3个正交方向施加,b=0、100、800 s/mm2,EPI_factor=45,所有序列均为呼吸门控或呼吸触发采集,余参数设置见表1,完成扫描保存原始数据。

表1 肾脏扫描序列参数设置Tab. 1 Protocol parameters for renal coronal & transverse scanning
1.3数据处理
肾扫描数据由受过良好培训医师使用工作站EWSv2.6.3软件处理、校正获得横断位ADC0-800图,以ADC0-800图为基础定位肾皮质、肾髓质、同层肌肉,放置1~5个感兴趣区(region of interest,ROI)(15~30 mm2)且避开伪影,软件自动计算相应ADC值,取3次测量平均值为最终结果且将原位右肾测量值用于3组比较。
1.4统计分析
2 结果
3组间性别与年龄无统计学意义(χ2性别=0.123,F年龄=0.342,P性别/年龄=0.426/0.734),组间具有可比性。
原位肾(右)、移植正常肾、急性排斥移植肾皮髓质及肌肉ADC0-800值(×10–3mm2/s)见表2。原位左肾皮髓质ADC0-800值分别为(1.97±0.22)及(1.67± 0.15),双侧皮质-皮质、髓质-髓质差值与0比较无统计学差异(t皮质/髓质=1.067/1.025,P皮质/髓质=0.812/0.833),见图1。原位肾、移植正常肾皮质ADC0-800值高于髓质(图1、2),其差值分别为(0.234±0.129)和(0.263±0.153),与总体0比较有统计学差异(t原位肾/移植肾=12.929/8.026,P均=0.000)。3组间肾皮质ADC值差异有统计学意义(P<0.05),3组肾髓质间、肌肉间ADC0-800值均无统计学意义(P>0.05),进一步两两比较发现肾皮质C组与A组、C组与B组间有统计学差异(P<0.05),而A组与B组间无统计学差异(P>0.05),见图1~3。以病理为标准,取1.76×10–3mm2/s为阈值,皮质ADC0-800诊断移植肾急性排斥ROC曲线下面积为0.942,敏感度、特异性分别为86.7%和90.4%(图4)。
志愿者肾脏高b值(0、800 s/mm2)ADC图均满足定量要求,正常组肾脏无肿胀渗出,T1WI肾皮髓质分辨清晰,DWI及高b值ADC图髓质信号低于皮质;急性排斥肾实质肿胀渗出,T1WI图皮髓质分辨不清,皮质扩散受限导致ADC图皮髓质信号趋于一致(图3A)。与低b值比较,高b值ADC图更稳定、信噪比适中、肾边界清楚,但皮髓质对比稍下降。

表2 3组肾皮髓质ADC值(单位:×10–3 mm2/s)Tab. 2 Kidney cortical & medullary ADC values(×10–3mm2/s) in the three groups
3 讨论
肾脏具有解剖与生理功能特殊性,其血流量占心输量约25%,皮质灌注约为髓质10倍[5]。皮质由肾小体以及弯曲走行的近曲小管和远曲小管组成表现为扩散各向同性,髓质则因肾小管及直小血管等结构而具有沿放射状条纹方向扩散自由、垂直方向明显扩散受限的各向异性[6]。同时肾小球每日可滤过180 L血浆,肾小管对滤过原尿重吸收和再分泌,通过逆流倍增等机制稀释浓缩形成尿液,以维持体内电解质和酸碱平衡使肾脏成为含水丰富的器官[7]。肾脏这种高血流灌注、高水分子代谢的生理特点以及特殊的解剖结构成为DWI和扩散张量成像(diffusion tensor imaging, DTI)应用的理想器官。DWI[8]是目前活体测量组织水分子布朗运动的惟一技术,通过两个以上b值扫描,采用单或双指数模型计算ADC可反映组织微循环灌注和水分子活动状态。单指数模型具有计算简便、易用且只需要2个b值扫描,为目前应用最广泛模型,但不能区分组织水分子真实扩散及微循环灌注。而双指数模型基于Le Bihan等[9]提出的体素内无规律运动(intravoxel incoherent motion,IVIM)计算,能够将组织内真实水分子扩散与微循环灌注假性扩散分离,精确地描述组织微观结构及功能改变,在无外源性对比剂情况下反映组织微灌注信息,缺点是扫描时间长且计算繁杂。王雪元等[10]证实双指数函数比单指数模型更适合于描述肾实质DWI信号强度随b值的变化规律。DTI则赋于观察者三维重组影像—扩散张量示踪图,用于显示髓质放射状纤维束样结构走行、方向及排列疏密情况[11]。
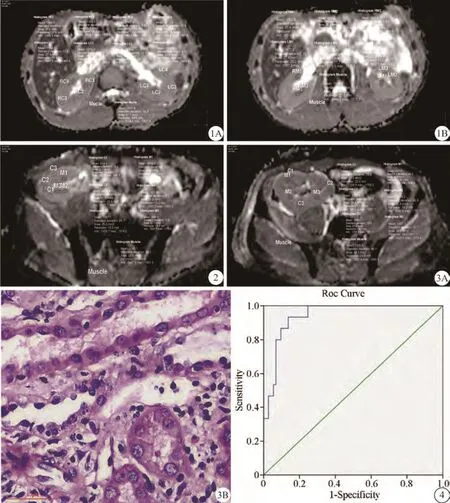
图1 男,22岁健康志愿者,原位肾。皮质(A)、髓质(B) ADC0-800值(×10–6mm2/s) 左右侧分别为1990.7、1917.4,1637.5、1634.3,同层肌肉为1547.8 图2 男,45岁患者,术后145天髂窝移植肾。皮髓质分辨尚清、ADC0-800值分别为2008.5和1667.7,肌肉为1543.1 图3 女,26岁患者,髂窝移植肾10天。肾肿胀渗出,皮质扩散受限导致皮髓质对比不清,皮髓质ADC0-800分别为1713.2、1651.2,肌肉为1591.5(A),穿刺活检提示T细胞免疫急性排斥(B) 图4 ROC曲线。以肾皮质ADC0-800<1.76×10–3mm2/s预测移植肾急性排斥,敏感度和特异度分别为86.7%和90.4%,准确度为94.2%Fig. 1 Male, 22 years old healthy volunteer, a kidney in situ. The values of ADC0-800calculated were respectively 1990.7, 1917.4(A), 1637.5, 1634.3(B) on cortex, medulla of the left and right, and muscle ADC was 1547.8 at the same slice. Fig. 2 Male, 45 years old patient, a normal renal in iliac fossa after 145 d from operation. ADC0-800were 2008.5, 1667.7 respectively on cortex, medulla, Corticomedullary differentiation(CMD) was clear yet and muscle ADC was 1543.1. Fig. 3 Femal, 26 years old patient, a 10-day transplanted kidney with acute rejection. It showed swelling and exudation, CMD was dim resulting from the cortex disorder, ADC0-800were 1713.2, 1651.2 respectively on cortex, medulla, muscle ADC was 1591.5(A), Pathology showed the acute rejection with T cellular immunity(B). Fig. 4 The ROC curve. To predict acute rejection with ADC0-800<1.76×10–3mm2/s, the AUC was 94.2%, the sensibility was 86.7%, the specificity was 90.4%.
课题组应用3个正交方向施加扩散敏感梯度场的DWI(b=0、100、800 s/mm2)扫描,因低b值ADC图像欠稳定、肾轮廓不清故以研究高b值ADC图作为对象研究。结果发现,原位肾双侧比较无统计学差异(图1 A、B),这是右肾代表原位肾与其余两组比较的基础。肾皮质ADC值(单位:× 10–3mm2/s)急性排斥组(1.68±0.14)明显小于原位肾(1.92±0.13)及移植正常肾组(1.93±0.15),但正常组肾皮质间、3组髓质间均无统计学差异(P>0.05)。笔者分析原因可能为急性排斥发生时炎性效应、氧化应激、细胞因子释放使肾皮质灌注降低、缺血肿胀,导致皮质含水减少及细胞外间隙缩小,最终造成水分子扩散受限、ADC值下降;而髓质小管结构排布相对疏松、炎症渗出及血液向髓质分流引起含水量增加、部分抵消灌注降低作用使ADC值变化不明显。实验结果与国内外移植肾急性排斥研究[11-14]报告基本一致,Heusch[11]和Sadowski[14]研究发现,急性排斥肾皮质和髓质血流灌注均降低且血流重新分布,皮质ADC值明显减低但髓质ADC值无明显变化。同时以DWI[15]、IVIM-DWI[16]和DTI[17]研究亦证实移植肾实质ADC值与灌注、肾功能具有显著相关性。课题中A组与B组间肾皮质、髓质无明显差异和Blondin等[18]报道一致,但与Thoeny等[19]研究认为移植肾ADC值低于正常人不完全相同,可能与本组移植正常肾均为术后3个月以上病例,其功能状态已经或基本恢复有关。实验还同时显示,A组和B组肾皮质ADC值均高于肾髓质(P<0.05),这与秦卫和[20]报道一致,分析可能与皮质灌注和含水量高、扩散各向同性而髓质小管状结构各向异性扩散、含水量较低等有关。以1.76×10–3mm2/s为阈值,皮质ADC诊断急性排斥准确率分别为0.942,敏感度与特异性分别为86.7%、90.4%,提示肾皮质ADC值对急性排斥早期诊断具有较高价值,这也与国外研究[21]结论类似。
针对同层较稳定的肌肉进行分析,笔者发现表观扩散系数3组间无统计学差异(P>0.05),这可大致认为磁体稳定性良好,进而证明不同组别和时间3组肾扫描数据有较高可信度,这是研究课题的一个创新点。
本研究尚存不足:(1)扫描仅采用一种机型完成,结论可能不完全适用其它型号或不同厂商、场强设备;(2)仅纳入术后1周至4周急性排斥移植肾且病例数量相对较少,结果可能有所偏倚及无法准确反映更大时间跨度的急性排斥肾脏;(3)术后1周至4周且穿刺病理组织学证实的非急性排斥移植肾与急性排斥肾的诊断实验评价尚未全部完成,这部分研究工作目前正在进行;(4)未能结合缺血、肾小管急性坏死、糖尿病肾损害等弥漫性肾病探讨,不同原因肾病诊断与鉴别价值尚有待进一步实验。
综上所述,DWI扫描可基本实现移植肾急性排斥早期诊断,异常变化主要位于肾皮质。笔者推荐临床3.0 T MRI应用中,DWI(b=800 s/mm2)扫描肾皮质ADC<1.76×10–3mm2/s可作为阈值用于移植肾急性排斥早期诊断。
参考文献[References]
[1]Womer KL, Kaplan B. Recent developments in kidney transplantation: a critical assessment. Am J Transplant, 2009,9(6): 1265-1271.
[2]Schwarz A, Gwinner W, Hiss M, et al. Safety and adequacy of renal transplant protocol biopsies. Am J Transplant, 2005, 5(8): 1992-1996.
[3]Masin-Spasovska J, Spasovski G, Dzikova S, et al. Do we have to treat subclinical rejections in early protocol renal allograft biopsies?. Transplant Proc, 2007, 39(8): 2550-2553.
[4]Zhang JL, Rusinek H, Chandarana H, et al. Functional MRI of the kidneys. J Magn Reson Imaging, 2013, 37(2): 282-293.
[5]Chou SY, Porush JG, Faubert PF. Renal medullary circulation: hormonal control. Kidney Int, 1990, 37(1): 1-13.
[6]Fukuda Y, Ohashi I, Hanafusa K, et al. Anisotropic diffusion in kidney: apparent diffusion coefficient measurements for clinical use. J Magnetic Resonance Imaging, 2000, 11(2): 156-160.
[7]Wang HY. Nephrology(V2). Beijing: People's Medical Publishing House, 1996: 3-50.王海燕. 肾脏病学(第2版). 北京: 人民卫生出版社, 1996: 3-50.
[8]Yang ZH, Feng F, Wang XY. A guide to technique of magnetic resonance imaging. Beijing: People's Military Medical Press,2014: 263-264.杨正汉, 冯逢, 王霄英. 磁共振成像技术指南-检查规范、临床策略及新技术应用. 北京: 人民军医出版社, 2014: 263-264.
[9]Le Bihan D. Intravoxel incoherent motion perfusion MR imaging: a wake-up call. Radiology, 2008, 249(3): 748-752.
[10]Wang XY, Xin W, Hu CH, et al. Comparison of fitting degree in monoexponential and biexponential model used to assess multi b-value DWI of renal parenchyma and CCRCC. Chin J Magn Reson Imaging, 2014, 5(2): 102-106.王雪元, 刑伟, 胡春洪, 等. 肾及肾透明细胞癌多b值扩散成像的单双指数拟合比较. 磁共振成像, 2014, 5(2): 102-106.
[11]Heusch P, Wittsack HJ, Krpil P, et al. Impact of blood flow on diffusion coefficients of the human kidney: a time-resolved ECG-triggered diffusion-tensor imaging(DTI) study at 3 T. J Magn Reson Imaging, 2013, 37(1): 233-236.
[12]Xu JJ, Xiao WB, Zhang L, et al. Value of diffusion-weighted MR imaging in diagnosis of acute rejection after renal transplantation. J Zhejiang Univ(Medical Sci), 2010, 39(2): 163-167.许晶晶, 肖文波, 张雷, 等. 磁共振扩散加权成像诊断移植肾急性排斥的应用研究. 浙江大学学报, 2010, 39(2): 163-167.
[13]Abou-El-Ghar ME, El-Diasty TA, El-Assmy AM, et al. Role of diffusion- weighted MRI in diagnosis of acute renal allograft dysfunction: a prospective preliminary study. Br J Radiol, 2012,85(1014): e206-211.
[14]Sadowski EA, Djamali A, Wentland AL, et al. Blood oxygenlevel-dependent and perfusion magnetic resonance imaging: detecting differences in oxygen bioavailability and blood flow in transplanted kidneys. Magn Reson Imaging, 2010, 28(1): 56-64.
[15]Wypych-Klunder K, Adamowicz A, Lemanowicz A, et al. Diffusion-weightedMR imaging of transplanted kidneys:Preliminary report. Pol J Radiol, 2014, 79: 94-98.
[16]Heusch P, Wittsack HJ, Heusner T, et al. Correlation of biexponential diffusion parameters with arterial spin-labeling perfusion MRI: results intransplanted kidneys. Invest Radiol,2013, 48(3): 140-144.
[17]Lanzman RS, Ljimani A, Pentang G, et al. Kidney transplant:functional assessment with diffusion-tensor MR imaging at 3 T. Radiology, 2013, 266(1): 218-225.
[18]Blondin D, Lanzman RS, Klasen J, et al. Diffusion-attenuated MRI signal of renal allografts: comparison of two different statistical models. AJR Am J Roentgenol, 2011, 196(6): 701-705.
[19]Thoeny HC, Dekeyzer F, Oyen RH, et al. Diffusion-weighted MR imaging of kidneys in healthy volunteers and patients with parenchymal diseases: initial experience. Radiology, 2005,235(3): 911-917.
[20]Qin W, Fu FX, Chen YJ, et al. Diffusion weighted MR Imaging in normal human kidney. Chin J Med Imaging, 2012, 20(4): 244-247.
秦卫和, 付飞先, 陈艳姣, 等. 正常成人肾脏磁共振扩散成像研究. 中国医学影像学杂志, 2012, 20(4): 244-247.
[21]Palmucci S, Mauro LA, Failla G, et al. Magnetic resonance with diffusion-weighted imaging in the evaluation of transplanted kidneys:updating results in 35 patients. Transplant Proc, 2012,44(7): 1884-1888.
Value of DWI to transplanted renals with early acute rejection: a preliminary study
LIANG Shi-wei1, HUANG Hai-bo2*, HUANG Gui-xiong2, GUAN Jun2, YANG Jianjun3, LIU Xu-yang41Department of Radiology, Guangxi CAPF Hospital, Nanning 530003, China2Department of Medical Imaging, 303rdHospital of PLA, Nanning 530021, China3Department of Pathology, 303rdHospital of PLA, Nanning 530021, China4Department of Pathology, 303rdHospital of PLA, Nanning 530021, China
Key wordsKidney transplantation; Graft rejection; Diffusion magnetic resonance imaging; Diffusion weighted imaging
AbstractObjective: To explore the value of DWI on transplanted renals with early acute rejection. Materials and Methods: Study protocol was approved by local ethics committee; informed consent was obtained. A total of 88 velunteers were enrolled and divided into three groups, as follows: Group A, 51 cases with healthy kidneys in situ;group B, 22 transplantation with stable renal function for at least 3 months after operating; and group C, 15 iliac allograft renals with early acute rejection from 1 week to 4 weeks after operating. T2W, T1W axial/coronal, and a transverse fat-saturated echo-planar DWI with 3 b-values(0, 100, 800 s/mm2) were performed on a 3.0 T scanner during normal breathing. EWS2.6.3 workstation was used to calculate the apparent diffusion coefficient(ADC) value of renal cortex, medulla, muscle respectively based on ADC0-800maps. Receiver operating characteristic(ROC) curve was used to predict the kidneys with early acute rejection. Results: No statistic significances were found for gender, age, ADC0-800of muscle among three groups(P>0.05), nor did ADC0-800values reveal a significant difference for left and right kidneys in situ(P>0.05). It showed renal cortex mean(+/-SD) ADC0-800values of (1.92±0.13), (1.93±0.15), (1.68±0.14)×10–3mm2/s for group A, B and C, respectively. Group C was significantly higher than both group A and B(P<0.05); however no statistic significance was found between group A and B(P>0.05); Nor did medullary ADC0-800values reveal a significant difference for 3 groups. While the differencebetween cortex and medulla was statistically significant for both groups A and B(P<0.05). With an ADC0-800<1.76×10–3mm2/s as diagnose critical points compared to biopsy, the sensibility was 86.7%, the specificity was 90.4%, and the accuracy was 0.942 in the prediction of the kidneys with early acute rejection. Conclusion: DWI is of important value in transplanted renals with early-stage acute rejection, it can provide reliable imaging evidence for treatment.
基金项目:广西科学研究与技术开发计划项目(编号:桂科攻1298003-8-6)
通讯作者:黄海波,E-mail: jackie000528@163. com
收稿日期:2015-11-01
中图分类号:R445.2;R617
文献标识码:A
DOI:10.12015/issn.1674-8034.2016.02.002
