突发恶性眼周肿瘤调查研究
2016-04-25ThabitOdatMohammadAlAqarbehAmeenAlKhateebMonsifAnaqrehAhmadAlDhoun
Thabit Odat, Mohammad Al-Aqarbeh, Ameen Al-Khateeb, Monsif Anaqreh, Ahmad Al-Dhoun
(作者单位:约旦,安曼 11855,约旦皇家医疗服务医院,眼科)
突发恶性眼周肿瘤调查研究
Thabit Odat, Mohammad Al-Aqarbeh, Ameen Al-Khateeb, Monsif Anaqreh, Ahmad Al-Dhoun
(作者单位:约旦,安曼 11855,约旦皇家医疗服务医院,眼科)
摘要
关键词:恶性的;眼周肿瘤;基底细胞癌
Abstract
•AIM: To study the incidence, epidemiology, and clinical characteristics of incidental malignant periocular tumors at the royal medical services hospitals of Jordan.
•METHODS: Retrospective medical charts of 327 patients with malignant periocular tumor diagnosis at Jordan military hospitals between 2004 and 2015 were reviewed. Study variables included age, gender, city where patient lived, the presenting complaint (not caused by or related to tumor), clinical and histological diagnosis, size of the tumor, location, and surgical procedure.
•RESULTS:A total of 327 charts reviewed, 46 (14.1%) patients were found to have incidental malignant periocular tumor. Males where affected more than females with a ratio of 2:1. The average age was 66.39±10.59 (22-83y). The most common presenting symptom or disease was blurring of vision secondary to cataract (44%), followed by combined cataract and other associated complaints such as epiphora in 21.7%.
Preliminary clinical diagnosis corresponded with histological diagnosis in 95.7% of skin cancer. The average size of the lesions was 1.04×0.85 mm2(0.2×0.2-3.0×3.0 mm2). There was no significant relationship between the maximum diameter of the tumor and age of the patient, (P=0.105). The most frequent location of tumors was the lower eyelid (30.4%) followed by the medial canthus (26.1%). The follow up period ranged between 6mo and 3y (average 9.3mo).
•CONCLUSION: Incidental malignant periocular malignant tumors were relatively common in this study, which urges excision of any suspicious lesion particularly young patients. A prospective study is needed to investigate the reasons why some patients neglect these lesions.
KEYWORDS:•malignant; periocular tumors; basal cell carcinoma
Citation:Odat T, Al-Aqarbeh M, Al-Khateeb A, Anaqreh M, Al-Dhoun A. Incidental malignant periocular tumors.GuojiYankeZazhi(IntEyeSci) 2016;16(4):610-613
INTRODUCTION

Malignant periocular tumors can arise primarily from any structures that surround the eyes such as the skin and its appendages, conjunctiva, and lacrimal gland, secondarily from distant organs by distant metastasis, or by invasion from the near structures such as the nasal cavity and sinuses[1]. The most common periocular tumors arise from the skin and usually related to direct sun exposure[2]. The risk of developing skin cancer is related to time and duration of sun exposure before the second decade of life[3-6]. The ultra-violet radiation exposure affects stratum basale; the only living layer of the epidermis, more than other layers and may lead toFigure 1Anatomic locations, clinical characteristics, and the presenting complaint or disease in patients with incidental malignant periocular tumorsA: Galbellar pigmented nodulo-ulcerative BCC in patient with bilateral brunescent cataract, bilateral blepharoptosis, and right corneal opacity; B: Right lower eyelid amelanotic nodulo-ulcerative BCC in patient with bilateral corneal dystrophy; C: Left lateral nasal wall pigmented nodulo-ulcerative BCC in patient with bilateral brunescent cataract, dermatochalasis, and upper lid retraction. D: Amelanotic nodular BCC in patient with left lower eyelid trichiasis and corneal opacity; E: Nodulo-ulcerative BCC in patient with diabetic retinopathy; F: Left lower eyelid pigmented BCC in patient with cataract; G: Right ala nasi pigmented nodulo-ulcerative BCC in patient with mild ectropion and epiphora; H: Pigmented nodular BCC in young patient.
malignant transformation[5-6]. Unless affecting vital structures and causing secondary symptoms such as epiphora when the tumor compresses the upper lacrimal drainage system small periocular lesions are usually neglected by elderly people and consider them as part of the aging process. Even asymptomatic big tumor may be unnoticed by blind patients. In young patients, primary skin cancer is rare and usually related to skin disease such as basal cell nevus syndrome (Gorlin-Goltz syndrome)[7]. With global radiation of 2080 kWh/m2and more than 300 sunny days a year, the risk of ultra-violet-related skin cancer may be relatively high in Jordan[8].
As there are no studies in the literature about the incidence of incidental malignant periocular tumors we retrospectively studied the incidence, epidemiology, and clinical characteristics of these tumors at the royal medical services hospitals of Jordan.
SUBJECTS AND METHODS
Retrospective medical charts of 327 patients with malignant periocular tumor diagnosis at Jordan military hospitals between 2004 and 2015 were reviewed. The Directorate of the Royal Medical services Institutional Review Board (IRB) prospectively granted ethical approval. Informed consent was not obtained because the data were collected retrospectively from the medical charts. Each patient was assigned a case number, so no personal identifiers were used in the data for statistical analysis. The data were then transferred to electronic excel spreadsheet for statistical analysis. Study variables included age, gender, city where patient lived, the presenting complaint (not caused by or related to tumor), clinical and histological diagnosis, size of the tumor, location, and surgical procedure.
Exclusion criteria included patients who had inadequate information, patients with a complaint related to or caused by the lesion, patients with a previously excised malignant periocular tumor, patients with a skin disorder that predisposes to cancer.

Figure 2The presenting complaint or disease of malignant periocular tumors.
Statistical analysis simple statistical analysis and parameters were used such as average, range, and standard deviation, andP.
RESULTS
Of the 327 charts reviewed, 46 (14.1%) patients were found to have incidental malignant periocular tumor. Males (30) outnumbered females (16) with a ratio of 2∶1. The average age was 66.39±10.59 (22-83y). The most common presenting symptom or disease was blurring of vision secondary to cataract 20 (44%), followed by combined cataract and other associated complaints such as epiphora in 10 (21.7%) (Figure 1). One patient, who was 22-year-old male and works as an anesthesia technician, had basal cell carcinoma (BCC) noticed by the surgeon incidentally (Figure 2).
Most of the patients lived in Irbid city in the north of Jordan 41.3%, followed by Amman city in the middle of Jordan 30.4%, Karak city south of Jordan 23.9%, Mafraq city east of Jordan 2.2%, and Aqaba city south of Jordan 2.2%. Preliminary clinical diagnosis corresponded with histological diagnosis in 95.7% of skin cancer while in 2 cases the preliminary clinical diagnoses were molluscum contagiosum and sebaceous cyst and the histological diagnoses were basal cell carcinoma(Figure 3). One patient was complaining of dermatochalasis and during follow up visits she was noticed to have proptosis secondary to lacrimal gland lymphoma.
The average size of the lesions was 1.04×0.85 mm (0.2×0.2-3.0×3.0 mm). Both the smallest and largest lesions were on the lateral side of the nose close to the medial canthus. There was no significant relationship between the maximum diameter of the tumor and age of the patient, (P=0.105). The most frequent location of tumors was the lower eyelid (30.4%) followed by the medial canthus (26.1%) (Figure 4).
Incisional biopsy is usually done to prove the diagnosis if the lesion is big or if excision may need major reconstruction, while excisional biopsy is done if the tumor is small and highly suspicious of malignancy. Most of small lesions in elderly patients can be excised and repaired by direct closure as they usually had skin laxity. Excisional biopsy and direct closure was done in about one fifth of patients (Table 1).The follow up period ranged between 6mo and 3y (average 9.3mo).
DISCUSSION
Malignant periocular tumors are usually painless and the presenting complaint is either related to the size, bleeding, or recurrent infection of the tumor or related to their effects on near structures such as upper lacrimal drainage system that lead to epiphora. Incidental periocular tumor was relatively common 14.1% in this study, which reflects the ignorance of these tumors by elderly patients, especially small ones, or because of visual impairment. Review of literature revealed that the most common incidental periocular tumor is the benign orbital cavernous hemangioma, which is usually found incidentally when imaging for other indication but there are no reports on the frequency of incidental malignant periocular tumors[9-10]. In our study the most common malignant tumor was basal cell carcinoma (97.8%) with its different clinical subtypes and this is due to the high ultraviolet radiation and frequent sunny days in Jordan[8]. Other reasons are the clinical nature of small BCC, which are usually subtle, and the high incidence of BCC (95%) in the general population in comparison with other skin cancer. Review of literature revealed that basal cell carcinoma is more common than all other human malignancies combined[11].
Basal cell carcinoma has characteristic clinical signs that aid in diagnosis but it can masquerade any benign lesions such ascutaneous leishmaniasis[12], BCC masqueraded contagious molluscum and sebaceous cyst in 2 cases in our study.
Although the BCCs is usually associated with advancing age but its incidence was increasing progressively among young adults (20-40y) over the last 2 decades[13]. This increase could be related to changes in sun exposure habits, environmental changes, migration patterns, and to a lesser extent, increased prevalence of immunosuppressant use[14].

Figure 3Clinical diagnosis of malignant periocular tumors.
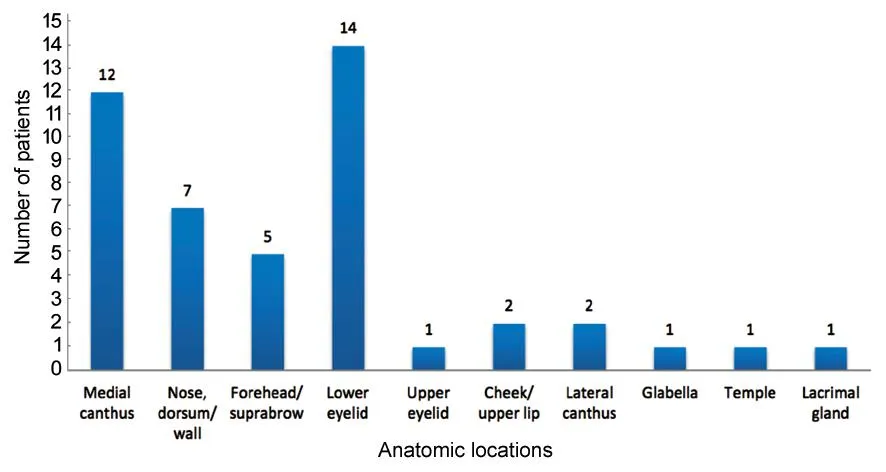
Figure 4Anatomic locations of malignant periocular tumors.
Table 1Surgical procedures used for malignant periocular tumors

SurgeryNumber(%)Incisionalbiopsy19(41.3%)Directclosurewithorwithoutcantholy-sis10(21.7%)Rhomboidflap6(13.0%)Slidingflaps3(6.5%)Rotationalflap3(6.5%)Tenzelsemicircularflap2(4.3%)Hughesflap1(2.2%)Glabellarflap1(2.2%)Lateralorbitotomy1(2.2%)Total46(100%)
Although there are more than 300 practicing ophthalmologists in Jordan, most of them do cataract surgery but the incidence of cataract is still high, which explain why most of the patients with incidental malignant periocular tumors, especially small size, presented for cataract (44%) treatment[14].
Because there were 2 oculoplastic clinics, one in Amman (Al Hussein hospital) and one in Irbid (Prince Rashid Bin Al Hassan hospital), the biggest military hospitals, this may explain the high incidence of malignant periocular tumors in these 2 cities. Most of the people in Irbid city live in rural areas, where many of them had outdoor activities; this may explain the high frequency of affected patients in this city.
While big tumors arising from the orbit are usually symptomatic, small tumors are usually discovered incidentally by radio-imaging studies for other indications[10]. In this study one patient had bilateral upper eyelids dermatochalasis and the subtle proptosis was noticed during follow up visit. Radio-imaging studies showed lacrimal gland mass and excisional biopsy revealed malignant non-Hodgkin lymphoma. Clinical examination and radiological investigations including PET scan showed no systemic involvement. Adjunctive radiotherapy and chemotherapy were given and the patient is under follow up over the last 3y.
The location of the tumors was similar to symptomatic periocular malignant tumors with regard to lower eyelids and medial canthus, (30.4% and 26.1% respectively)[15], but different with regard to other locations. The dorsum of the nose (15.2%) was more frequently affected than the forehead (10.7%) and upper eyelids (2.2%).
Slightly more than one fifth of the tumors were small enough to be completely excised and closed directly without any other adjuvant surgical procedure and one tumor was big that required upper eyelid sharing procedure.
Overall,the incidence of incidental periocular malignant tumor is significant and any patients, particularly young adults, with a suspicious lesion should have a biopsy to rule out malignancy as early diagnosis decreases patient morbidity and mortality. A prospective study is needed to investigate the reasons why some patients neglect these lesions.
REFERENCES
1 Mulay K, Aggarwal E, White VA. Periocular sebaceous gland carcinoma: A comprehensive review.SaudiJOphthalmol2013;27(3):159-165
2 Malhotra R, Huilgol SC, Huynh NT, Selva D. The Australian Mohs database, part II: periocular basal cell carcinoma outcome at 5-year follow-up.Ophthalmology2004;111(4):631-636
3 Cummins DL, Cummins JM, Pantle H, Silverman MA, Leonard AL, Chanmugam A. Cutaneous malignant melanoma.MayoClinicProc2006,81(4):500-507
4 English DR, Armstrong BK, Kricker A, Winter MG, Heenan PJ, Randell PL. Case-control study of sun exposure and squamous cell carcinoma of the skin.IntJCancer1998;77(3):347-353
5 Balk SJ; Council on Environmental Health; Section on Dermatology. Ultraviolet radiation: a hazard to children and adolescents.Pediatrics2011;127(3):e791-817
6 D'Orazio J, Jarrett S, Amaro-Ortiz A, Scott T. UV Radiation and the Skin.IntJMolSci2013;14(6):12222-12248
7 Bala Subramanyam S, Naga Sujata D, Sridhar K, Pushpanjali M. Nevoid Basal cell carcinoma syndrome: a case report and review.JMaxillofacOralSurg2015;14(Suppl 1):11-15
8 Etier I, Al Tarabsheh A, Ababneh M. Analysis of Solar Radiation in Jordan.JJMIE2010;4(6):733-738
9 Boari N, Gagliardi F, Castellazzi P, Mortini P. Surgical treatment of orbital cavernomas: clinical and functional outcome in a series of 20 patients.ActaNeurochir(Wien) 2011;153:491-498
10 LeBedis CA, Sakai O. Nontraumatic orbital conditions: diagnosis with CT and MR imaging in the emergent setting.Radiographics2008;28(6):1741-1753
11 Wong CS, Strange RC, Lear JT.Basal cell carcinoma.BMJ2003;327(7418):794-798
12 Jaouni T, Deckel Y, Frenkel S, Ilsar M, Pe'er J. Cutaneous leishmaniasis of the eyelid masquerading as basal cell carcinoma.CanJOphthalmol2009;44(5):e47
13 Delfino S, Innocenzi D, Di Lorenzo G, Scalvenzi M, Montesarchio V, Feroce F, Baldi A, Persichetti P. An increase in basal cell carcinoma among the young: an epidemiological study in a middle-south Italian population.AnticancerRes2006;26(6C):4979-4983
14 Mohan SV, Chang AL. Advanced Basal Cell Carcinoma: Epidemiology and Therapeutic Innovations.CurrDermatolRep2014;3:40-45
15 Arlette JP, Carruthers A, Threlfall WJ, Warshawski LM. Basal cell carcinoma of the periocular region.JCutanMedSurg1998;2(4):205-208
DOI:10.3980/j.issn.1672-5123.2016.4.05
通讯作者:Thabit Odat. thabitodat@hotmail.com
目的:研究约旦皇家医疗服务医院中突发恶性眼周肿瘤的发病率、流行病学及临床特征。
方法:回顾性研究。回顾分析我院在2004~2015年收治的327例诊断为恶性眼周肿瘤患者的病历资料。研究参数包括年龄、性别、患者所在城市、现病史(非肿瘤引起或与肿瘤相关的)、临床与病理诊断、肿瘤大小、位置及手术方式等。
结果:在327例患者中,46例(14.1%)患者诊断出患有突发恶性眼周肿瘤。男性与女性的患病比例为2:1。平均年龄为66.39±10.59(22-83)岁。最常见的临床疾病或症状为白内障致视觉模糊(44%),其次为白内障合并其他相关症状类似泪溢症等(21.7%)。初步临床诊断联合病理诊断95.7%为皮肤癌。平均病变大小为1.04×0.85(0.2×0.2~3.0×3.0)mm2。肿瘤的最大直径和患者年龄无明显关系(P=0.105)。最常见的肿瘤位于下眼睑(30.4%),其次为内眦处(26.1%)。随访时间6mo至3a(平均9.3mo)。
结论:突发恶性眼周肿瘤在本研究中较为常见,任何可疑病灶须尽快切除。一些患者忽视这些病变的原因需要进一步的前瞻性研究分析。
引用:Odat T, Al-Aqarbeh M, Al-Khateeb A, Anaqreh M, Al-Dhoun A. 突发恶性眼周肿瘤调查研究.国际眼科杂志2016;16(4):610-613