肾素-血管紧张素系统抑制剂对高血压患者脂代谢的改善作用
2016-03-23程军
程军
摘 要 据统计,超过半数的高血压患者合并脂代谢异常,两者并存时,冠心病的发病和死亡风险显著增加。不同降压药物对脂代谢的影响不尽相同。肾素-血管紧张素系统(RAS)在体内广泛分布,在血压调节、水电解质平衡及糖脂代谢等诸多方面发挥重要作用。RAS抑制剂(RASI)在有效降压的同时,在一定程度上对高血压患者的脂代谢具有改善作用。本文拟从RAS系统与脂代谢的相互作用以及RASI对高血压患者脂代谢的改善作用两个方面进行综述。
关键词 高血压 脂代谢 肾素-血管紧张素系统抑制剂
中图分类号:R972.4; R544.1; R543.5 文献标识码:A 文章编号:1006-1533(2016)03-0035-06
Effect of the inhibitors of renin-angiotensin system on the lipid metabolism of patients with hypertension
CHENG Jun*
(Kidney Disease Center , The First Hospital affiliated to Zhejiang University, Hangzhou 310006, China)
ABSTRACT Current data show that over half of hypertensive patients have lipid metabolic abnormalities. Coexistence of hypertension and lipid metabolic abnormality may significantly increase the morbidity and mortality of coronary heart disease. Effects of different kinds of antihypertensive agents on lipid metabolism vary. Renin-angiotensin system (RAS), widely distributed in human body, plays an important role in regulation of blood pressure, water-electrolyte balance as well as glucose and lipid metabolism. RAS inhibitors (RASI) can also improve lipid metabolism in hypertensive patients besides the effective reduction of blood pressure. This article reviews the interaction of RAS system and lipid metabolism and the improvement of lipid metabolism by RASI in hypertensive patients.
KEY WORDS hypertension; lipid metabolism; renin-angiotensin system inhibitors
高血压患者合并脂代谢异常,可表现为总胆固醇(TC)、甘油三酯(TG)和低密度脂蛋白胆固醇(LDL-C)升高,而高密度脂蛋白胆固醇(HDL-C)降低。CONSIDER研究显示,高血压患者合并脂代谢异常比例为61.5%,在脂代谢异常患者中,50%患有高血压[1]。高血压和脂代谢异常均是重要的心血管危险因素,两者并存时,冠心病的发病和死亡风险明显升高[2-3]。为最大程度减少心血管终点事件风险,应对各种危险因素实施综合管理,当为合并脂代谢异常的高血压患者选择降压药物时,需充分考虑降压药物对脂代谢的影响。
1 RAS激活与脂代谢异常的相互影响
肾素-血管紧张素系统(renin-angiotensin system,RAS)在体内广泛分布,在血压调节、水电解质平衡及糖脂代谢等诸多方面发挥重要作用。RAS激活与胰岛素抵抗及糖脂代谢异常相互作用,促进粥样硬化性疾病的发生和发展。
1.1 胆固醇对RAS的影响
早期研究发现高胆固醇血症中LDL-C可增加血管平滑肌细胞血管紧张素II受体I型(angiotensin II type 1 receptor,AT1R)的基因表达[4] ,并且氧化的低密度脂蛋白也可以增加人冠状动脉内皮细胞AT1R的表达[5]。后续研究表明,高胆固醇血症可使家兔主动脉AT1R表达增加,使血管紧张素II(angiotensin II,ANG II)收缩血管的作用增强[6]。与给予标准饮食的C57BL/6小鼠相比,低密度脂蛋白受体缺乏(LDLR -/-)的小鼠经高脂和高胆固醇饮食后,血浆血管紧张素(angiotensin,AGT)和ANG II浓度显著升高[7]。血脂指标的改善可以缓解RAS在血管疾病中的影响,HDL-C可预防糖尿病所致的大鼠主动脉AT1R的表达增加[8]。
大脑胆固醇代谢的改变与大脑RAS的调控存在一定联系。研究表明,在大鼠原代神经元中,27-羟基胆固醇和24S-羟基胆固醇可通过肝脏X b受体(liver X receptor b,LXR-b)下调AGT、血管紧张素转化酶(angiotensin converting enzyme,ACE)和AT1R[9]。此外,高胆固醇饮食的大鼠大脑ACE和AGT表达增加[9]。与血浆胆固醇水平相关的胆固醇代谢物可致大脑RAS激活以及代谢综合征中的高血压。
胆固醇和/或其代谢产物激活RAS的机制尚不清楚,但可能涉及LXR或其他脂质传感核受体。然而,就LXR来说,LDLR- /-或载脂蛋白E缺乏(ApoE -/-)的小鼠给予LXR配体可显著降低动脉粥样硬化病变的形成[10],LXR配体激活RAS的能力并不与这些化合物对抗动脉粥样硬化的属性一致。目前尚需进一步研究来明确胆固醇和/或胆固醇代谢物调控RAS的机制。
1.2 RAS激活对胆固醇的影响
ANG II对胆固醇代谢产生一定的影响。AT1R缺乏的LDLR-/-小鼠血浆ANG II浓度较高,RAS激活促进LDL-C导致动脉粥样硬化[7];但是血清胆固醇没有因为AT1aR 缺乏而发生明显改变,随后的研究发现,给ApoE -/-或LDLR- /-的小鼠注射ANG II并不明显影响血清胆固醇[11]或脂蛋白胆固醇分布[12],这表明RAS对胆固醇浓度和分布的直接影响相对有限。
其他数据显示的ANG II促进动脉粥样硬化的作用是因为其对胆固醇修饰和泡沫细胞形成的影响,而不必直接影响血清胆固醇浓度。已经证实在原代培养的人单核巨噬细胞中,ANG II可下调酰基辅酶A(acyl coenzyme A,Acyl-CoA)的表达,这可能增加动脉粥样硬化病变的胆固醇含量[13]。几项研究已经报道,在巨噬细胞系小鼠腹腔巨噬细胞中,ANG II可能通过激活NADPH氧化酶而增加低密度脂蛋白的氧化[14-15]。值得注意的是,注射了ANG II的ApoE-/-小鼠给予他汀类药物可降低动脉粥样硬化[16]。他汀类药物减少ANG II诱导的动脉粥样硬化的能力独立于血清胆固醇浓度。ANG II可影响胆固醇致动脉粥样硬化的特性而不一定必然改变其在血液中的浓度。大多数研究RASI影响血脂异常的临床试验主要量化了LDL、HDL和TGs的血液浓度,而不是可促进动脉粥样硬化形成的胆固醇代谢产物(如氧化的低密度脂蛋白)。因此,血脂水平可能并不是衡量RASI对抗脂代谢异常最重要的直接指标。
1.3 RAS激活与胰岛素抵抗
ANG II是RAS的主要效应分子,可调节胰岛素的生物学功能,其机制主要有:① ANG II和胰岛素有一段共同的细胞信号转导途径,即激活磷酯酰肌醇-3-羟激酶(phosphatidylinositol 3-hydroxy kinase,PI3K)。胰岛素经其受体介导PI3K途径激活,而ANG II却抑制PI3K途径。因此,RAS激活可抑制胰岛素通过PI3K途径介导的葡萄糖转运、糖原合成和脂质代谢,引起胰岛素抵抗。②ANG II抑制脂肪形成,过多的TG不能在脂肪中贮存,而沉积在肝脏、肌肉等胰岛素敏感组织,从而促进外周胰岛素抵抗的发生。
RAS激活引起的胰岛素抵抗可进一步导致脂代谢异常。胰岛素抵抗时,脂肪组织中的激素敏感性TG脂肪酶的活性增加,促进脂肪分解,引起血液中游离脂肪酸升高;胰岛素抵抗还可导致继发性高胰岛素血症,抑制脂肪酸的合成,使肝脂释放减少,肝脏发生脂肪蓄积。同时,胰岛素抵抗时,极低密度脂蛋白合成和释放增多,使LDL、TG生成增加[17]。
2 RASI改善高血压患者脂代谢
2.1 不同降压药物对高血压患者脂代谢的不同影响
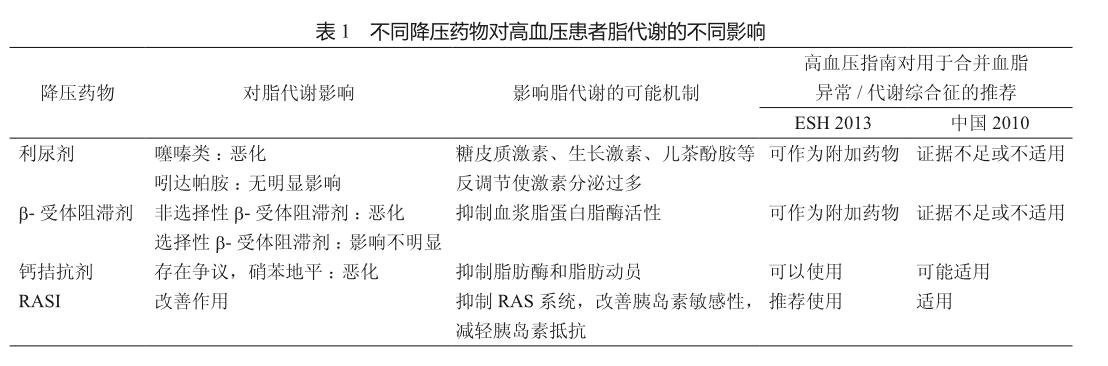
利尿剂、钙通道拮抗剂(calcium channel antagonist,CCB)、b-受体阻滞剂、血管紧张素转化酶抑制剂(angiotensin-converting enzyme inhibitors,ACEIs)和血管紧张素Ⅱ受体拮抗剂(angiotensin receptor II blocker,ARB)均为常用降压药物[18]。这些药物对于合并不同临床情况的高血压患者有不同的应用。不同类别的降压药物,对脂代谢的影响不尽相同(表1)。噻嗪类利尿剂可引起TC、TG、LDL-C升高。袢利尿剂同样可干扰糖脂代谢。氨苯蝶啶和螺内酯则对脂代谢无明显影响。利尿剂对脂质代谢的不利影响,可能与糖皮质激素、生长激素、儿茶酚胺等的反调节使激素分泌增多,进而使TC、LDL-C及TG合成增多有关。非选择性b-受体阻滞剂可使血清LDL-C、TG升高、HDL-C降低,对TC作用甚微。选择性b-受体阻滞剂对血脂影响不明显[19]。不同b-受体阻滞剂对脂代谢的不同影响,可能与其对血浆脂蛋白脂酶(lipoprotein lipase,LPL)活性的抑制作用强弱有关[20]。CCB对脂代谢的影响存在争议。有研究发现 CCB可改善脂代谢,使HDL升高,TG降低[21],而亦有研究提示CCB可升高TG和TC水平。其机制可能与抑制脂肪酶和脂肪动员有关。ACEI可抑制ANG II的合成,ARB可削弱ANG II的作用。RASI可促进胰岛素介导的葡萄糖转运和代谢,改善胰岛素抵抗,增强胰岛素敏感性,进而改善糖脂代谢,表现为TG、TC及LDL-C降低和HDL-C升高[22]。
2.2 RASI对高血压患者脂代谢的影响
2013 ESH/ESC高血压指南、2014日本高血压指南以及2010中国高血压防治指南均推荐RASI为血脂/代谢异常患者的优选降压药[23-25]。
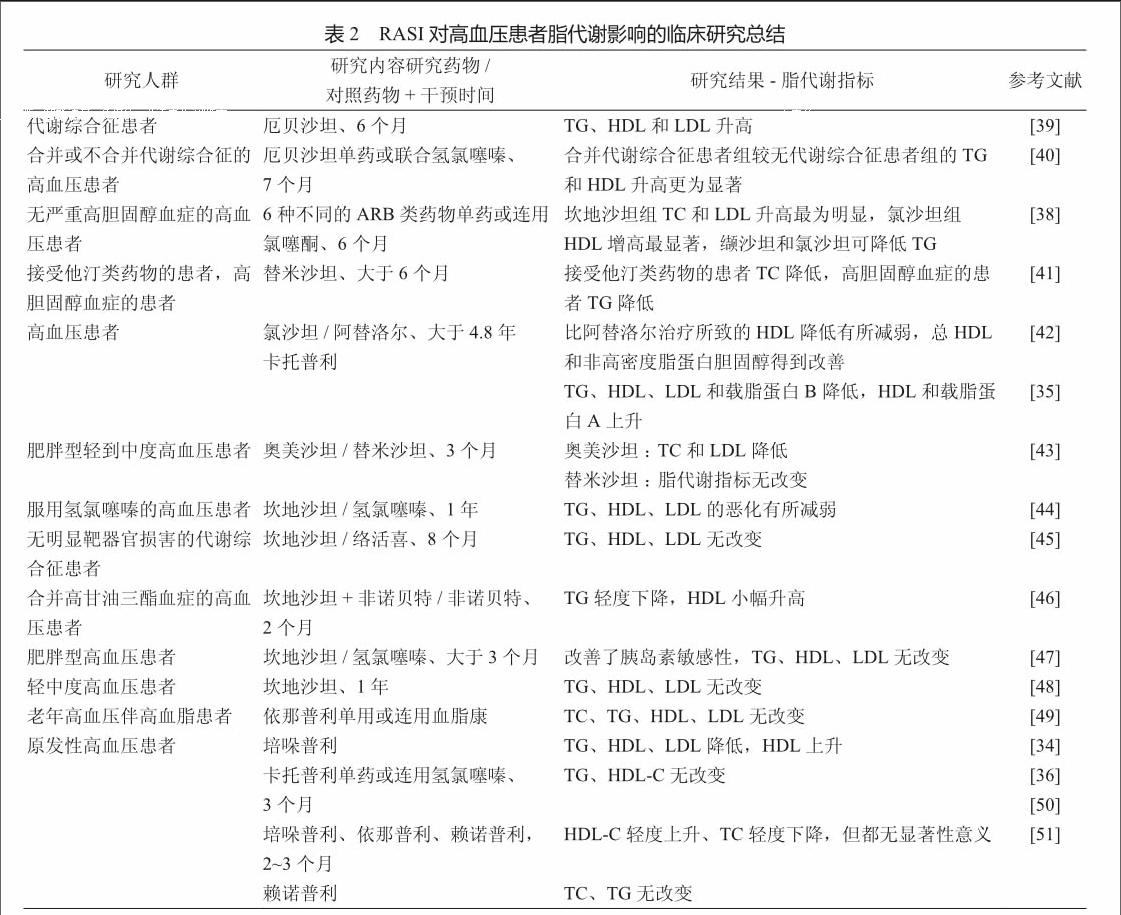
研究表明,ACEI和ARB可削弱ANGⅡ的促脂作用,减小脂肪细胞的体积,增加胰岛素敏感性。ACEI及ARB对高血压患者脂代谢影响的有关研究见表2。ACEI既可抑制ANGⅡ的生成[26],也可抑制激肽酶Ⅱ,使缓激肽水平升高[27],改善胰岛素敏感性。ARB可使胰岛素抵抗的肥胖小鼠TG和非酯化脂肪酸水平降低[28]。较早被发现具有改善胰岛素抵抗作用的ARB有替米沙坦和厄贝沙坦,因其可激活PPAR-g系统[29]。然而,后有研究提示,缬沙坦(不激活PPAR-g)与替米沙坦(激活PPAR-g)对胰岛素敏感性的改善作用相似,PPAR-g介导的刺激在替米沙坦改善胰岛素敏感性方面仅发挥很小的作用[30]。Meta分析结果显示,与CCB相比,ARB(包括缬沙坦、氯沙坦和替米沙坦)能显著改善非糖尿病患者胰岛素抵抗[31]。LIFE[32]和VALUE [33]的结果也提示,ARB可能通过改善胰岛素抵抗在代谢方面发挥有益作用,其可能机制是ARB通过阻断AT1受体而改善内皮功能,抑制氧化应激和炎症反应,提高组织对胰岛素的敏感性。
陈源源等[34]研究发现,培哚普利可使原发性高血压患者的胆固醇、TG、LDL降低,而HDL升高。王秀英等[35]的结果亦发现卡托普利能降低高血压患者的胆固醇、TG、LDL以及载脂蛋白B,并升高HDL和载脂蛋白A,而这一结果在研究间并不一致[36]。
Hanefeld等[37]在缬沙坦治疗高血压合并血脂异常患者的多中心、随机、双盲、安慰剂对照试验中发现,缬沙坦在有效降压的同时,可以改善高血压患者脂代谢指标LDL-C和TC。另有在高血压人群比较6种不同ARB类药物的研究发现,ARB总体对TC、LDL-C、HDL-C及TG等脂代谢指标具有改善作用,而不同ARB在降压作用相似的情况下,对各脂代谢指标的改善作用不尽相同,伊普罗沙坦和替米沙坦对多个指标的改善作用未见统计学意义,而缬沙坦和氯沙坦在各项指标的改善方面均具有统计学意义[38]。
综上,高血压合并脂代谢异常的患者其冠心病发病和死亡风险明显增加,应尽早全面干预。RASI在改善高血压患者脂代谢方面较其他类别降压药物具有优势,并被国内外高血压管理指南推荐用于高血压合并代谢综合征/高脂血症。在该类患者合理规范应用RASI有望在降压的同时促进其他代谢危险因素的改善,进而最大程度地降低心血管事件风险。
参考文献
[1] 刘军, 王薇, 刘静, 等. 门诊高血压病患者合并心血管病危险因素及血压控制现状[J]. 中华心血管病杂志, 2013, 41(12): 1050-1054.
[2] Neaton JD, Wentworth D. Serum cholesterol, blood pressure, cigarette smoking, and death from coronary heart disease. Overall findings and differences by age for 316, 099 white men. Multiple Risk Factor Intervention Trial Research Group[J]. Arch Intern Med, 1992, 152(1): 56-64.
[3] 武阳丰, 赵冬, 周北凡, 等. 中国人群血脂异常诊治和危险分层方案的研究[J]. 中华心血管病杂志, 2007, 35(5): 428-33.
[4] Nickenig G, Sachinidis A, Michaelsen F, et al. Upregulation of vascular angiotensin II receptor gene expression by lowdensity lipoprotein in vascular smooth muscle cells[J]. Circulation, 1997, 95(2): 473-478.
[5] Li D, Saldeen T, Romeo F, et al. Oxidized LDL upregulates angiotensin II type 1 receptor expression in cultured human coronary artery endothelial cells: the potential role of transcription factor NF-kappaB[J]. Circulation, 2000, 102(16): 1970-1976.
[6] Nickenig G, Jung O, Strehlow K, et al. Hypercholesterolemia is associated with enhanced angiotensin AT1-receptor expression[J]. Am J Physiol, 1997, 272 (6 Pt 2): H2701-H2707.
[7] Daugherty A, Rateri DL, Lu H, et al. Hypercholesterolemia stimulates angiotensin peptide synthesis and contributes to atherosclerosis through the AT1A receptor[J]. Circulation, 2004, 110(25): 3849-3457.
[8] Van Linthout S, Spillmann F, Lorenz M, et al. Vascularprotective effects of high-density lipoprotein include the downregulation of the angiotensin II type 1 receptor[J]. Hypertension, 2009, 53(4): 682-687.
[9] Mateos L, Ismail MA, Gil-Bea FJ, et al. Side chain-oxidized oxysterols regulate the brain renin-angiotensin system through a liver X receptor-dependent mechanism[J]. J Biol Chem, 2011, 286(29): 25574-25585.
[10] Joseph SB, McKilligin E, Watson MA, et al. Synthetic LXR ligand inhibits the development of atherosclerosis in mice[J]. Proc Natl Acad Sci U S A, 2002, 99(11): 7604-7609.
[11] Cassis LA, Gupte M, Thayer S, et al. ANG II infusion promotes abdominal aortic aneurysms independent of increased blood pressure in hypercholesterolemic mice[J]. Am J Physiol Heart Circ Physiol, 2009, 296(5): H1660-H1665.
[12] Henriques TA, Huang J, DSouza SS, et al. Orchidectomy, but not ovariectomy, regulates angiotensin II-induced vascular diseases in apolipoprotein E-deficient mice[J]. Endocrinology, 2004, 145(8): 3866-3872.
[13] Kanome T, Watanabe T, Nishio K, et al. Angiotensin II upregulates acyl-CoA: cholesterol acyltransferase-1 via the angiotensin II Type 1 receptor in human monocytemacrophages[J]. Hypertens Res, 2008, 31(9): 1801-1810.
[14] Keidar S, Attias J, Smith J, et al. The angiotensin-II receptor antagonist, losartan, inhibits LDL lipid peroxidation and atherosclerosis in apolipoprotein E-deficient mice[J]. Biochem Biophys Res Commun, 1997, 236(3): 622-625.
[15] Keidar S, Kaplan M, Hoffman A, et al. Angiotensin II stimulates macrophage-mediated oxidation of low density lipoproteins[J]. Atherosclerosis, 1995, 115(2): 201-215.
[16] Wang JA, Chen WA, Wang Y, et al. Statins exert differential effects on angiotensin II-induced atherosclerosis, but no benefit for abdominal aortic aneurysms[J]. Atherosclerosis, 2011, 217(1): 90-96.
[17] 金思思, 汪春湖, 吴金明. 胰岛素抵抗与脂代谢紊乱[J].临床内科杂志, 2008, 25(9): 647-648.
[18] James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8)[J]. JAMA, 2014, 311(5): 507-520.
[19] 戸塚光哉, 宮下洋, 伊藤嘉晃, et al. Celiprolol hydrochlorideの脂質代謝に及ぼす影響特にlow density lipoproteinのサイズ変化について[J]. 日本老年医学会雑誌, 2001, 38(3): 352-359.
[20] 彭健. 高血压与血脂代谢紊乱[J]. 中国实用内科杂志, 2002, 22(4): 202-204.
[21] Ahaneku JE, Sakata K, Urano T, et al. Influence of baseline values on lipids, lipoproteins and fibrinolytic parameters during amlodipine treatment of hypertension in Japanese patients[J]. Pharmacol Res, 2000, 41(1): 75-79.
[22] Goldberg AI, MC Dunlay, CS Sweet. Safety and tolerability of losartan compared with atenolol, felodipine and angiotensin converting enzyme inhibitors[J]. J Hypertens Suppl, 1995, 13(1): S77-S80.
[23] Shimamoto K, Ando K, Fujita T, et al. The Japanese Society of Hypertension Guidelines for the management of hypertension (JSH 2014)[J]. Hypertens Res, 2014, 37(4): 253-390.
[24] Mancia G, Fagard R, Narkiewicz K, et al. 2013 ESH/ESC Guidelines for the management of arterial hypertension: the task force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC)[J]. J Hypertens, 2013, 31(7): 1281-1357.
[25] 中国高血压防治指南修订委员会. 中国高血压防治指南2010[J]. 中华心血管病杂志, 2011, 39(7): 579-616.
[26] Furuhashi M, Ura N, Higashiura K, et al. Blockade of the renin-angiotensin system increases adiponectin concentrations in patients with essential hypertension[J]. Hypertension, 2003, 42(1): 76-81.
[27] Jandeleit-Dahm KA, Tikellis C, Reid CM, et al. Why blockade of the renin-angiotensin system reduces the incidence of new-onset diabetes[J]. J Hypertens, 2005, 23(3): 463-273.
[28] Okada K, Hirano T, Ran J, et al. Olmesartan medoxomil, an angiotensin II receptor blocker ameliorates insulin resistance and decreases triglyceride production in fructose-fed rats[J]. Hypertens Res, 2004, 27(4): 293-299.
[29] Schupp M, Janke J, Clasen R, et al. Angiotensin type 1 receptor blockers induce peroxisome proliferator-activated receptor-gamma activity[J]. Circulation, 2004, 109(17): 2054-2057.
[30] Ushijima K, Takuma M, Ando H, et al. Effects of telmisartan and valsartan on insulin sensitivity in obese diabetic mice[J]. Eur J Pharmacol, 2013, 698(1-3): 505-510.
[31] Yang Y, Wei RB, Xing Y, et al. A meta-analysis of the effect of angiotensin receptor blockers and calcium channel blockers on blood pressure, glycemia and the HOMA-IR index in nondiabetic patients[J]. Metabolism, 2013, 62(12): 1858-1866.
[32] Dahlof B, Devereux RB, Kjedsen SE, et al. Cardiovascular morbidity and mortality in the Losartan Intervention For Endpoint reduction in hypertension study (LIFE): a randomised trial against atenolol[J]. Lancet, 2002, 359(9311): 995-1003.
[33] Julius S, Kjeldsn SE, Weber M, et al. Outcomes in hypertensive patients at high cardiovascular risk treated with regimens based on valsartan or amlodipine: the VALUE randomised trial[J]. Lancet, 2004, 363(9426): 2022-2031.
[34] 陈源源, 孙宁玲, 唐建平, 等. 三种长效缓释降压药对血脂代谢的影响[J]. 心肺血管病杂志, 1996, 115(3): 169-171.
[35] 王秀英, 张道东. 卡托普利对高血压病患者血糖、胰岛素脂蛋白水平影响的研究[J]. 高血压杂志, 1999, 7(3): 242-244.
[36] 王翠平. ACEI对高血压病患者糖脂代谢的影响[J]. 中国实用医药杂志, 2007, 2(14): 111-112.
[37] Hanefeld M, Abletshauser C. Effect of the angiotensin II receptor antagonist valsartan on lipid profile and glucose metabolism in patients with hypertension[J]. J Int Med Res, 2001, 29(4): 270-279.
[38] Kyvelou SM, Vyssoulis GP, Karpanou EA, et al. Effects of antihypertensive treatment with angiotensin II receptor blockers on lipid profile: an open multi-drug comparison trial[J]. Hellenic J Cardiol, 2006, 47(1): 21-28.
[39] Parhofer KG, Münzel F, Krekler M. Effect of the angiotensin receptor blocker irbesartan on metabolic parameters in clinical practice: the DO-IT prospective observational study[J/OL]. Cardiovasc Diabetol, 2007, 6: 36. doi:10.1186/1475-2840-6-36.
[40] Kintscher U, Bramlage P, Paar WD, et al. Irbesartan for the treatment of hypertension in patients with the metabolic syndrome: a sub analysis of the Treat to Target post authorization survey. Prospective observational, two armed study in 14, 200 patients[J/OL]. Cardiovasc Diabetol, 2007, 6: 12. doi:10.1186/1475-2840-6-12.
[41] Inoue T, Morooka T, Moroe K, et al. Effect of telmisartan on cholesterol levels in patients with hypertension-Saga Telmisartan Aggressive Research (STAR)[J]. Horm Metab Res, 2007, 39(5): 372-376.
[42] Olsen MH, Qachtell K, Beevers G, et al. Effects of losartan compared with atenolol on lipids in patients with hypertension and left ventricular hypertrophy: the Losartan Intervention For Endpoint reduction in hypertension study[J]. J Hypertens, 2009, 27(3): 567-574.
[43] de Luis DA, Conde R, Gaozalez-Saqrado M, et al. Effects of telmisartan vs olmesartan on metabolic parameters, insulin resistance and adipocytokines in hypertensive obese patients[J]. Nutr Hosp, 2010, 25(2): 275-279.
[44] Lindholm LH, Persson M, Alaupovic P, et al. Metabolic outcome during 1 year in newly detected hypertensives: results of the Antihypertensive Treatment and Lipid Profile in a North of Sweden Efficacy Evaluation (ALPINE study)[J]. J Hypertens, 2003, 21(8): 1563-1574.
[45] Tomiyama H, Yambe M, Yamada J, et al. Discrepancy between improvement of insulin sensitivity and that of arterial endothelial function in patients receiving antihypertensive medication[J]. J Hypertens, 2007, 25(4): 883-889.
[46] Koh KK, Quon MJ, Han SH, et al. Additive beneficial effects of fenofibrate combined with candesartan in the treatment of hypertriglyceridemic hypertensive patients[J]. Diabetes Care, 2006, 29(2): 195-201.
[47] Grassi G, Seravalle G, DellOro R, et al. Comparative effects of candesartan and hydrochlorothiazide on blood pressure, insulin sensitivity, and sympathetic drive in obese hypertensive individuals: results of the CROSS study[J]. J Hypertens, 2003, 21(9): 1761-1769.
[48] Nishida Y, Takahashi Y, Nakayama T, et al. Effect of candesartan monotherapy on lipid metabolism in patients with hypertension: a retrospective longitudinal survey using data from electronic medical records[J/OL]. Cardiovasc Diabetol, 2010, 9: 38. doi:10.1186/1475-2840-9-38.
[49] 黄炜. 依那普利对老年高血压伴高脂血症患者血脂水平影响的观察[J]. 中国误诊学杂志, 2003, 3(4): 532-532.
[50] Oksa A, Gajdoes, M, Fedelesova V, et al. Effects of angiotensin-converting enzyme inhibitors on glucose and lipid metabolism in essential hypertension[J]. J Cardiovasc Pharmacol, 1994, 23(1): 79-86.
[51] Thurig C, Bohlen L, Schneider M, et al. Lisinopril is neutral to insulin sensitivity and serum lipoproteins in essential hypertensive patients[J]. Eur J Clin Pharmacol, 1995, 49(1-2): 21-26.
