成人冠状动脉扩张的临床特点及相关因素分析
2016-02-25陈建海季祥武张志会周鹏
陈建海 季祥武 张志会 周鹏
成人冠状动脉扩张的临床特点及相关因素分析
陈建海季祥武张志会周鹏
冠状动脉扩张(CAE)是指冠状动脉局部扩张超过正常邻近冠状动脉直径或者冠状动脉最大直径1.5倍[1]。在美国及欧洲一些国家的相关研究中,CAE的发病率在1%~5%之间,并可导致心肌梗死、心绞痛等疾病的发生[2-3]。Markis等[4]将CAE分为:Ⅰ型,两支或者三支冠状动脉弥漫性扩张;Ⅱ型,一支冠状动脉弥漫性扩张,另一支冠状动脉局限性扩张;Ⅲ型,单支冠状动脉弥漫性扩张;Ⅳ型,单支冠状动脉局限性扩张。随着冠状动脉造影(CAG)在我国广泛开展,越来越多的CAE患者被检测出来,其发病与动脉粥样硬化、炎症性疾病、结缔组织疾病或先天性因素有关[5]。Antoniadis等[6]认为CAE主要与动脉粥样硬化相关,但目前CAE的确切病因还不甚清楚。本文回顾性分析冠状动脉造影患者中CAE的检出率、临床特点及相关危险因素,旨在为心血管医师了解成人CAE提供准确的临床依据。
对象与方法
一、研究对象
2011年1月至2014年3月期间以胸闷、胸痛等症状收住潍坊市人民医院心内一科3 443例,根据2007年ACC/AHA不稳定心绞痛/非ST段抬高心肌梗死患者管理指南诊断为不稳定性心绞痛并行CAG的患者[7]。筛选标准:所有入选患者均在我院心内科导管室行CAG术,采用Seldinger法穿刺右侧桡动脉或者右股动脉,将6F Judkins导管送达左、右冠状动脉开口处,左冠状动脉采用头位、右肩位、右前斜、肝位及蜘蛛位投影,右冠状动脉采用左前斜位及头位等方位进行投影,并由两名以上有经验的临床心脏介入医师目测阅片,并详细记录患者CAG的结果。冠状动脉管径扩大超过正常邻近冠状动脉直径或者冠状动脉最大直径1.5倍即确定为CAE[1]。查阅其冠状动脉造影结果及住院病历,收集患者相关临床资料。从3 443例行CAG患者中筛选出存在CAE患者68例,作为观察组,其中男51例,女17例。排除标准:AMI,肺栓塞,主动脉夹层,心肌病,心脏瓣膜病,心功能不全,冠状动脉支架植入手术史,严重肝肾功能不全,外周血管病,血液病,恶性肿瘤病史,急性及慢性感染,自身免疫性疾病,以及脑卒中;所有研究对象收缩压均大于90 mm Hg (1 mm Hg=0.133 kPa),舒张压均大于60 mm Hg。采用随机数字表法选出72例阻塞性冠状动脉疾病(OCAD)患者及70例冠状动脉正常(NCA)患者作为对照组,其中男34例,女36例。本研究为观察性研究,不涉及伦理问题。
二、方 法
入选患者均详细记录性其别、年龄、吸烟史、糖尿病史、既往最高血压值,计算出脉压差,并于入院后次日清晨空腹 (采血时间于CAG前8 h以上)采集肘前空腹静脉血2 ml,置入有分离胶的试剂管中静置2 h,送检验科检测患者的尿酸、血尿素氮、血清肌酐、空腹血糖、总胆固醇、甘油三酯、HDL-C、LDL-C及脂蛋白a水平,详细记录以上检验结果。
三、统计学处理

结果
一、CAE患者病变冠状动脉血管分布情况
CAE患者中,右冠状动脉(RCA)扩张病例37例,占CAE患者总数的54.41%;前降支(LAD)扩张病例14例,占CAE患者总数的20.59%;回旋支(LCX)扩张病例5例,占CAE患者总数的7.35%;LAD合并LCX扩张及LAD合并RCA扩张均为2例,均占CAE患者总数的2.94%,LCX合并RCA扩张1例,占CAE患者总数的1.47%;LAD、LCX及RCA均扩张的患者为7例,占CAE患者总数的10.29%。
二、CAE组、OCAD组、NCA组一般资料的比较
CAE组与OCAD组比较中,年龄、性别、高血压病史、既往最高血压值、脉压差、吸烟史、糖尿病史差异无统计学意义(P>0.05);CAE组与NCA组在年龄及男性患者例数比较中,前者均大于后者,且差异有统计学意义(P分别为0.040、0.001),2组其他一般资料比较差异无统计学意义(P>0.05),见表1。
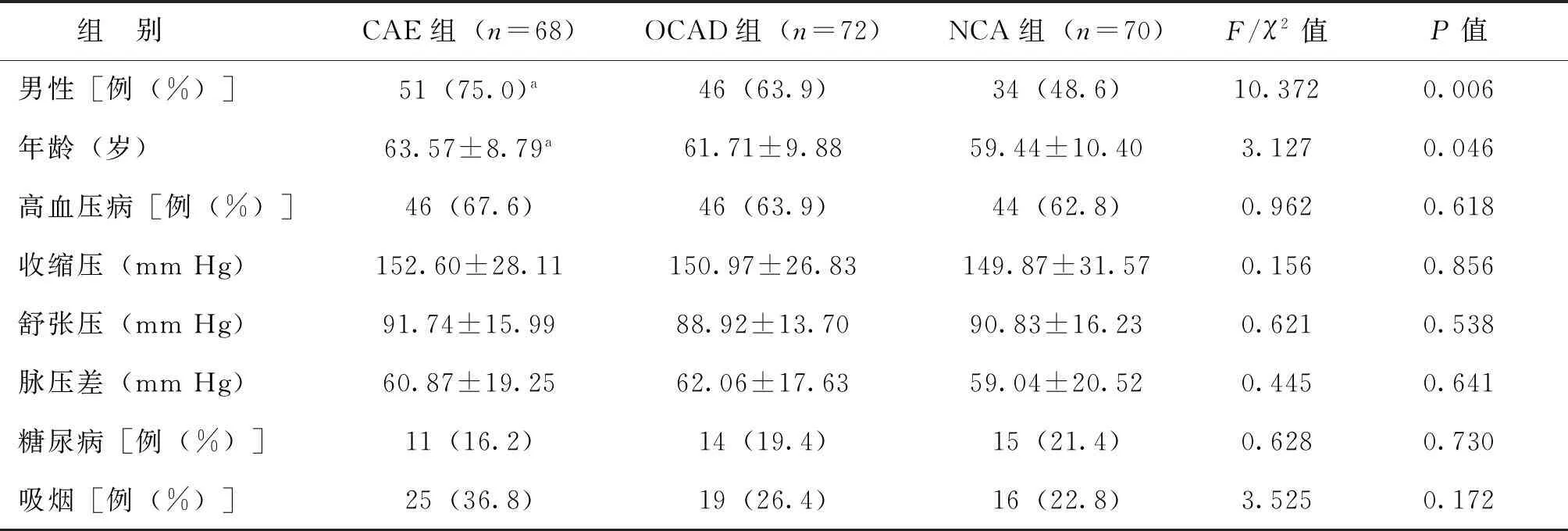
表1CAE组、OCAD组、NCA组一般资料的比较
注:CAE组与NCA组比较,aP<0.05
三、CAE组、OCAD组、NCA组生化指标的比较
CAE患者空腹血糖水平明显低于OCAD患者,差异有统计学意义(P=0.006),而2组尿酸、血尿素氮、血清肌酐、总胆固醇、甘油三酯、HDL-C、LDL-C及脂蛋白a比较,差异均无统计学意义(P>0.05);CAE组与NCA组在脂蛋白a水平比较中,前者高于后者,且差异有统计学意义(P=0.039),2组间其他各项生化指标比较差异均无统计学意义(P均>0.05),见表2。

表2
注:与CAE组比较,aP<0.05,bP<0.01;与OCAD组比较,cP<0.05
四、冠状动脉扩张相关性及危险因素分析
进行Logistic回归分析发现,男性、高年龄及高脂蛋白a水平为冠状动脉扩张的危险因素(性别:OR=3.299,95%CI1.529~7.119,P=0.002;年龄:OR=1.041,95%CI1.001~1.082,P=0.045;脂蛋白a:OR=1.020,95%CI1.003~1.037,P=0.023),见表3。
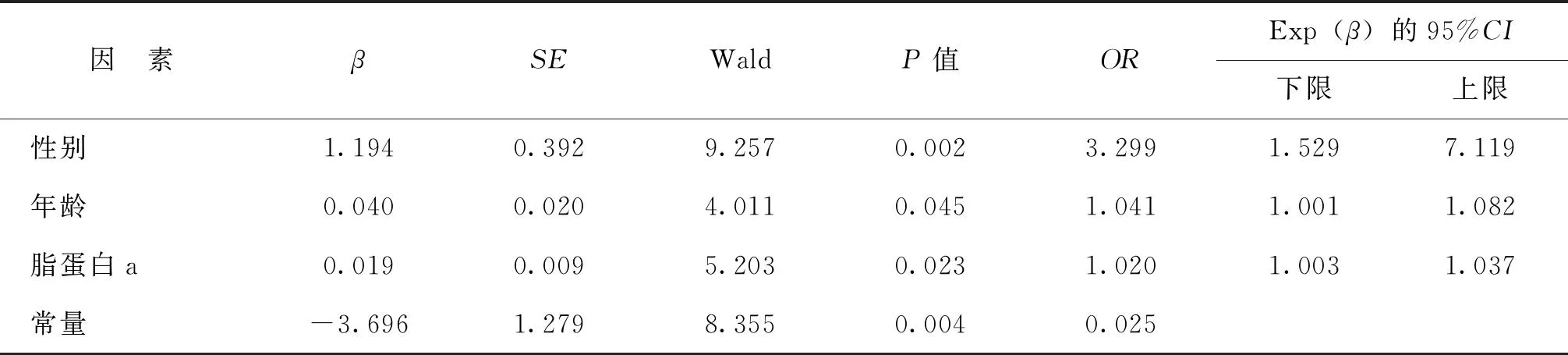
表3冠状动脉扩张相关危险因素的Logistic回归分析
讨论
CAE约50%是由动脉粥样硬化所致,20%~30%为先天性异常,而10%~20%与炎症性疾病或者结缔组织疾病相关,如硬皮病、Ehlers-Danlos综合征、ANCA相关性血管炎、梅毒性主动脉炎或者川崎病[5]。在欧美一些国家中,其发病率在1%~5%,CAE最常见于右冠状动脉,次之见于前降支,回旋支最不易受侵犯,与本研究中CAE发病情况一致[1-2,8]。但也有研究表明CAE最常见于前降支[9]。
在本研究中,CAE患者空腹血糖水平明显低于OCAD患者,差异有统计学意义(P<0.05),而2组患者年龄、性别、高血压病史、既往最高血压值、脉压差、血压分级、吸烟史、糖尿病史、尿酸、血尿素氮、血清肌酐、总胆固醇、甘油三酯、HDL-C、LDL-C及脂蛋白a比较,差异均无统计学意义;CAE组与NCA组在年龄、男性患者数及脂蛋白a水平比较中差异有统计学意义,以上研究结果支持CAE与冠状动脉粥样硬化有关的观点,且本研究结果与国际相关研究相符[5-6]。Logistic回归分析表明,男性、高龄及高脂蛋白a水平为CAE的危险因素,这与Giannoglou等[10]研究结果相一致,而且Giannoglou等还报道CAE患者与冠心病患者相比,糖尿病及AMI患病率低,在性别比例上,男女患病比例为2∶1;新加坡地区的相关研究显示其CAE男女患病比率为3∶1[11]。
Antoniadis等[6]认为CAE与动脉粥样硬化在组织病理学方面有许多相似之处,主要表现为冠状动脉扩张节段内可见中层胶原和弹性纤维明显分解,以及内、外弹力层的破坏,但Boles等[1]认为粥样硬化难以解释以下问题:①糖尿病患者中CAE低发病率;②右冠状动脉易受侵犯;③冠状动脉中层弹性成分缺失;④在基质金属蛋白酶-2(MMP-2)、MMP-3、MMP-9及MMP-12启动子区域发现潜在的基因多态性。Dogan及Dahi等[12-13]同样发现MMP-2、MMP-3及MMP-9水平增高与CAE有关。Pinar Bermúdez等[14]认为糖尿病主要影响血管内膜层,而非血管中层膜,因此糖尿病对血管重构起抑制作用。该观点可解释CAE患者较OCAD患者糖尿病发病率低的现象,但仍缺乏相关临床证据。
临床上CAE主要引起心绞痛及AMI,有研究表明CAE合并OCAD患者较单纯冠状动脉扩张患者病死率高,但在远期预后方面无明显差异[15]。该病目前仍无统一有效的管理方案,若一旦确诊应积极抗凝、抗血小板,预防因扩张所致血栓形成,并且应用β受体阻断药降低心肌氧耗量,钙离子拮抗剂抑制冠状动脉痉挛,ACEI及他汀类药物抑制冠状动脉重构、抑制炎症反应等;此外外科手术治疗及经皮介入方法在小儿川崎病治疗方面疗效确切,但对于成人CAE疗效尚不明确。根据不同的扩张类型(如扩张大小、扩张部位、冠状动脉阻塞程度及分支型扩张的起始部位),成人CAE在切除术、结扎术及冠状动脉搭桥术上曾取得显著疗效,但仍无最佳手术方法[16]。
由于本研究样本量相对较少,因此样本代表性不强。冠状动脉扩张的确切机制目前在国际上还无统一观点,也无统一行之有效的管理方案,与该疾病相关的危险因素及治疗方法还需大样本的进一步研究。
参考文献
[1]Boles U, Zhao Y, David S, Eriksson P, Henein MY. Henein. Pure coronary ectasia differs from atherosclerosis: morphological and risk factors analysis. Int J Cardiol,2012,155(2):321-323.
[2]Sultana R, Sultana N, Ishaq M, Samad A. The prevalence and clinical profile of angiographic coronary ectasia. J Pak Med Assoc,2011,61(4):372-375.
[3]汤昔康, 覃丽君, 范毅敏. 川崎病并发心肌梗塞5例报告. 新医学, 2013,44(4):243-246.
[4]Markis JE, Joffe CD, Cohn PF, Feen DJ, Herman MV, Gorlin R. Clinical significance of coronary artery ectasia. Am J Cardiol,1976,37(2):217-222.
[5]Tony H, Meng K, Wu B, Zeng Q. Among ectasia patients with coexisting coronary artery disease, TIMI frame count correlates with ectasia size and markis type IV is the commonest. Cardiol Res Pract,2015,2015:282170.
[6]Antoniadis AP, Chatzizisis YS, Giannoglou GD. Pathogenetic mechanisms of coronary ectasia. Int J Cardiol,2008,130(3):335-343.
[7]Anderson JL, Adams CD, Antman EM, Bridges CR, Califf RM, Casey DE Jr, Chavey WE 2nd, Fesmire FM, Hochman JS, Levin TN, Lincoff AM, Peterson ED, Theroux P, Wenger NK, Wright RS, Smith SC Jr, Jacobs AK, Adams CD, Anderson JL, Antman EM, Halperin JL, Hunt SA, Krumholz HM, Kushner FG, Lytle BW, Nishimura R, Ornato JP, Page RL, Riegel B; American College of Cardiology; American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction); American College of Emergency Physicians; Society for Cardiovascular Angiography and Interventions; Society of Thoracic Surgeons; American Association of Cardiovascular and Pulmonary Rehabilitation; Society for Academic Emergency Medicine. ACC/AHA 2007 guidelines for the management of patients with unstable angina/non-ST-Elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction) developed in collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine. J Am Coll Cardiol,2007,50(7):e1-e157.
[8]Amirzadegan AR, Davoodi G, Soleimani A, Lotfi Tokaldany M, Hakki Kazazi E, Shabpiray H, Khorsand Askari M. Association between Traditional Risk Factors and Coronary Artery Ectasia: A Study on 10057 Angiographic Procedures among Iranian Population. J Tehran Heart Cent,2014,9(1):27-32.
[10]Giannoglou GD, Antoniadis AP, Chatzizisis YS, Damvopoulou E, Parcharidis GE, Louridas GE. Prevalence of ectasia in human coronary arteries in patients in northern Greece referred for coronary angiography. Am J Cardiol,2006,98(3):314-318.
[11]Lam CS, Ho KT. Coronary artery ectasia: a ten-year experience in a tertiary hospital in Singapore. Ann Acad Med Singapore,2004,33(4):419-422.
[12]Dogan A, Tuzun N, Turker Y, Akcay S, Kaya S, Ozaydin M. Matrix metalloproteinases and inflammatory markers in coronary artery ectasia: their relationship to severity of coronary artery ectasia. Coron Artery Dis,2008, 19(8):559-563.
[13]Dahi S, Karliner JS, Sarkar R, Lovett DH. Transgenic expression of matrix metalloproteinase-2 induces coronary artery ectasia. Int J Exp Pathol,2011,92(1):50-56.
[14]Pinar Bermúdez E, López Palop R, Lozano Martínez-Luengas I, Cortés Sánchez R, Carrillo Sáez P, Rodríguez Carreras R, Picó Aracil F, Valdés Chávarri M. Coronary ectasia: prevalence, and clinical and angiographic characteristics. Rev Esp Cardiol,2003,56(5):473-479.
[15]Shakerian F, Sanati H, Kiani R, Khezerlou N, Firouzi A, Zahedmehr A. Comparison of outcomes of diseased coronary arteries ectasia, stenosis and combined. Res Cardiovasc Med,2015,4(1):e25206.
[16]Dahhan A. Coronary artery ectasia in atherosclerotic coronary artery disease, inflammatory disorders, and sickle cell disease. Cardiovasc Ther,2015,33(2): 79-88.
(本文编辑:杨江瑜)

·临床研究论著·
261000 潍坊,潍坊医学院(陈建海,张志会,周鹏);261000 潍坊,潍坊医学院附属潍坊市人民医院(季祥武)
【摘要】目的研究冠状动脉扩张发病的临床特点、发生率及相关的危险因素。方法从3 443例住院并行选择性冠状动脉造影术的患者中筛选出68例冠状动脉扩张患者作为CAE组,并采用随机数字表法随机选出72例阻塞性冠状动脉疾病患者(OCAD组)及70例冠状动脉正常患者(NCA组)作为对照,对比分析3组的临床特点及生化指标。结果冠状动脉扩张的发生率为1.98%,其中右冠状动脉发生率最高,占所有冠状动脉扩张患者总数的54.41%;其次为前降支,为20.59%;冠状动脉两支扩张的发生率为7.35%,冠状动脉三支同时发生扩张的概率为10.29%。通过分析发现,CAE患者空腹血糖水平明显低于OCAD患者,差异有统计学意义(P<0.05)。CAE组与NCA组比较冠状动脉扩张男性比例高,CAE组患者在年龄及脂蛋白a水平明显高于NCA组患者,差异均有统计学意义(P<0.05)。Logistic回归分析表明,男性、高龄及高脂蛋白a水平为冠状动脉扩张的危险因素(性别:OR=3.299,95%CI 1.529~7.119,P=0.002;年龄:OR=1.041,95%CI 1.001~1.082,P=0.045;脂蛋白a:OR=1.020,95%CI 1.003~1.037,P=0.023)。结论成人冠状动脉扩张在右冠状动脉发生率最高,男性、高龄及高脂蛋白a水平是成人冠状动脉扩张发生的危险因素。
【关键词】冠状动脉扩张;成人;危险因素;粥样硬化
Clinical characteristics and risk factors of coronary artery ectasia in adultsChenJianhai,JiXiangwu,ZhangZhihui,ZhouPeng.DepartmentofGraduateFaculty,WeifangMedicalCollege,Weifang261000,China
Correspondingauthor,JiXiangwu,E-mail:jxwwf@126.com
【Abstract】ObjectiveTo investigate the clinical characteristics, incidence and risk factors of coronary artery ectasia (CAE). MethodsIn total, 3 443 hospitalized patients undergoing elective coronary angiography were retrospectively analyzed. Among them, 68 patients diagnosed with CAE were selected and assigned into the observation group. Seventy two patients with obstructive coronary artery disease (OCAD) and 70 with normal coronary artery (NCA) were allocated into the control group by random number table method. Clinical characteristics and biochemical indexes were statistically compared between three groups. ResultsThe incidence of CAE was 1.98%, mainly in the right coronary artery with an incidence rate 54.41% among all patients, followed by anterior descending branch (20.59%). The incidence of CAE in two branches of the coronary artery was 7.35%, and 10.29% for three branches of the coronary artery. The level of fasting plasma glucose (FPG) in patients with CAE was significantly lower than that in OCAD counterparts (P< 0.05). In CAE group, we found that the incidence of male of coronary artery ectasia was significantly higher than NCA group. The age of CAE patients was significantly older and the lipoprotein a level was considerably higher compared with those of NCA counterparts (P<0.05). Logistic regression analysis revealed that the risk factors of CAE were male(OR=3.299, 95%CI 1.529-7.119, P=0.002), old age (OR=1.041, 95%CI 1.001-1.082, P=0.045) and high level of LP(a) (OR=1.020, 95%CI 1.003-1.037, P=0.023). Conclusions The incidence of CAE is the highest in the right coronary artery. Male gender, old age and high level of lipoprotein a are risk factors of the incidence of CAE in adults.
【Key words】Coronary artery ectasia; Adult; Risk factors;Atherosclerosis
收稿日期:(2015-08-06)
通讯作者,季祥武,E-mail: jxwwf@126.com
DOI:10.3969/j.issn.0253-9802.2016.01.012
