Path Exploration for Long-term Care of Rural Disabled Elderly: A Case Study of G Town in South Shaanxi
2016-01-12,
,
1. College of Humanities and Social Development, Northwest A&F University, Yangling 712100, China; 2. College of Marxism, Northwest A&F University, Yangling 712100, China
1 Introduction
China is a typical country with people getting old before getting rich. Rapidly increasing elderly population especially the disabled elderly brings about many new problems for both families and the society. At present, researches of disabled elderly focus on urban elderly. However, compared with urban elderly, rural elderly face more problems. G town is situated in Daba Mountain area of South Shaanxi. Its economic and traffic conditions are underdeveloped. Due to implementation of the policy of returning farmland to forest and immigration policy, farmland area of villagers is limited, and most young and middle aged villagers do migrant work. Therefore, in the situation of gradual weakening of family endowment function and serious lagging of rural social security, it is urgent to discuss solutions to the problem of long-term care of rural disabled elderly.
2 Definition of related concepts and data source
2.1ConceptdefinitionIn international academics, Activity of Daily Living (ADL) indicator or Instrumental Activities of Daily Living (IADL) indicator is applied to evaluate health condition of the elderly[1]. With reference to these two indicator systems, we defined the disabled elderly as people older than 60 years old having at least one obstacle of activity of daily living or instrumental activities of daily living, with such status lasting or expected to last 90 days or longer. In 7 indicators, namely, having a meal, wearing clothes, indoor walking, going to toilet, control of urine or stool, bath, shopping, and social communications, obstacle in one or two items deemed as "slightly disabled", obstacle in three or four items considered "moderately disabled", and obstacle in five or more items deemed as "seriously disabled".
2.2DatasourceIn this study, we applied interview method and semi-structural questionnaire method. Using the purposive sampling method, we selected three natural villages in G Town of South Shaanxi as sample communities, and make a field survey in July-August, 2015. Survey objects included rural elderly and their family caregivers. Here, caregivers refer to relatives of disabled elderly, including spouse, children, and relatives, and the care giving duration is 6 months or longer. We distributed 253 copies of semi-structural questionnaire to rural elderly older than 60, received 237 valid copies (93.7%), and interviewed 76 family caregivers. In data analysis, we carried out qualitative analysis on data of in-depth interview, and made a statistical analysis of valid samples with the aid of SPSS20.0 software.
3 Basic situations of disabled elderly in G Town
According to data of statistical yearbook, by the end of 2014, there were 37683 people older than 60 in G Town, accounting for 16.32% of total population of the whole county. Calculated at international standard, this county has entered the aging society. According to introduction of workers from G Town Working Committee Office on Aging, the rate of aging of G Town in 2014 was up to 16.8%, and many elderly people were disabled. Through our survey, basic situations of disabled elderly in G Town are as follows:
3.1DisabledpeoplearemanyandhavehighlevelofdisabilityWith constant extension of average life expectancy, rural elderly people in G Town gradually increases, accordingly presenting the constant increase in population size of rural disabled elderly. In the past literature, disabled elderly population in China was 2%-20%, showing near 10 times of gap, which is closely related to size and representatives of samples of past researches[2]. In our survey in G Town, there were 67 disabled elderly people, accounting for 28.3% of the elderly. Moderately and serious disabled elderly people accounted for 22.3% of the elderly. From the perspective of age structure, 70-79 years of people were the main part of disable elderly, accounting for 17.3% of the total, as listed in Table 1. They could not live independently and their self-assistance ability was low. Diseases leading to disability of elderly people mainly include hypertension, cerebral stroke, coronary heart disease, and bone and joint diseases.
Table1Distributionoflevelofdisability

LevelAgeSlightNumberPercentage∥%ModerateNumberPercentage∥%SeriousNumberPercentage∥%DisabilityNumberPercentage∥%60-69yearsold41.720.810.473.070-79yearsold93.8208.4125.14117.3Olderthan8010.473.0114.6198.0Total145.92912.22410.16728.3
3.2Left-behindelderlyaccountforalargerportionIn G Town, most disabled elderly are left-behind elderly, accounting for 77.3% of disabled elderly. Reasons for this are various. First, G Town belongs to a mountainous area, its farmland is little. Farming fails to support their livelihood, thus most young and middle aged labors choose to do migrant work. Second, most village-level primary schools are merged in recent years. Young parents go to cities or towns to accompany their children, then the elderly are left behind. Third, after implementation of relocation policy of immigrants in South Shaanxi, most relocated households have the situation of children living in new houses while the elderly still living in old houses. These factors lead to constant increase of left-behind elderly and the elderly living alone. In our survey, most left-behind elderly had excellent physical condition, and could live independently or partially independently. 61.2% elderly could live basically independently. They believed that as long as they are not paralyzed, they would insist on farming or engaging in breeding. Besides, about 37.6% elderly needed long-term care and their living were quite difficult.
3.3FamiliesofdisabledelderlyhaveeconomichardshipEconomic situation is an essential factor restricting living standards and care giving quality of rural disabled elderly families. In our survey, income of rural disabled elderly mainly came from farming, endowment insurance, old age allowance, minimum living security and government subsidies, and doing odd jobs, accounting for 37.3%, 29.1%, 14.1% and 9.2% respectively. Their expenditure was mainly medicines and living cost. About 79.3% elderly had monthly expenditure lower than 500 yuan, showing most families of elderly were poor and there was the problem of disability leading to poverty. In our survey, caregivers generally provided food and clothes for the elderly, and the expenditure of care giving was mainly medicines and living cost, accounting for more than 90% of the surveyed elderly, as shown in Table 2. In rural areas, few families use health products or employ nurse. Due to economic difficulty, the elderly worried about no money when fall ill. As many as 97.5% elderly hoped to get financial support and various government subsidies and welfare.
Table2Itemsofexpenditureofelderlycaregivers

ItemsofexpenditureCaregiversNumberPercentage∥%ElderlyNumberPercentage∥%Medicines7598.715866.7Livingcost(foodandothers)76100.012452.3Healthproducts1114.5229.2Operationfee810.52410.1Nursingexpenses45.241.7
3.4MostelderlyfeellonelyIn families of disabled elderly, most children did migrant work and seldom went home, and some children even seldom made a call. They thought it reasonable that no call is needed as long as there is no matter. Vacancy of children will make the elderly feel unsafe and lonely. In addition to the situation of inconvenient movement, rural elderly seldom communicate with other villagers or feel having nothing to talk. As a result, they may generate the thought of "no using when getting old". In our interview, some disabled elderly liked talking and hoping to solve some practical problems, while some talked little. Long time of loneliness has seriously affected their physical and mental health. Without children living beside, some elderly even felt desperate.
4 Analysis on difficulties of long-term care of rural disabled elderly
At present, family endowment is still the dominant endowment mode in rural areas of China. In our interview, 93.8% elderly depended on family endowment, partly because rural families do not have the ability of purchasing endowment services, and partly because the thought of "bringing up children for the purpose of being looked after in old age" and "spend the remaining years in hometown" are still widespread in rural society. However, the actual foundation for adhering to such filial doctrine is gradually declining and shaking. Our survey indicated that there are still many actual problems in long-term care of rural disabled elderly, and these problems have posed serious challenges to their families.
4.1Ruralendowmentsecuritylagsbehind
4.1.1Scope of social welfare is narrow. At present, the supply of rural social welfare is inconsistent with rural endowment demand. In G Town of South Shaanxi, social welfare facilities are far to satisfy demands. First, welfare of rural elderly remains the living security of households enjoying the 5 guarantees. In other words, only elderly people without family may enjoy the minimum living security, and the security level is relatively low. Therefore, except little people who can enjoy high age subsidies, most elderly are not included into the institutional arrangement of rural disabled elderly below the living standards. Secondly, in existing social welfare organizations, public organizations such as homes for the aged accept only those disabled elderly without children. Thirdly, there is still a large gap of endowment funds in rural endowment. Besides, working methods are not perfect. The mechanism for reimbursement of medical assistance expenses is not reasonable. In consequence, expenses incurred by some elderly people from chronic diseases fail to be reimbursed.
4.1.2Development of rural endowment service industry is backward. At present, the market development of rural long-term care service system is backward, and there is a wide gap in socialization between urban and rural endowment[3]. In the first place, development of endowment service organizations lags far behind. In the county of G Town, there is only one apartment for the elderly and it only has 27 beds, so the reception ability is relatively limited. There is still no mature endowment organization. The only elderly service center basically stagnates due to lack of funds and human resources. Besides, limited to economic level of disabled families, it is impossible to implement market-oriented care services. In our survey, few families could afford the expenses of formal care. Except few families having once employed nurses when the elderly were hospitalized, most elderly were looked after by their children or relatives. In addition, there is no professional team.
4.2Changesinrurallivingenvironment
4.2.1Rural hollowing in the condition of migrant work economy. Empty nest of the elderly has become a concentrated manifestation of rural hollowing. At present, China has about 50 million rural left-behind elderly[4]. High age, disability and disease have become major concerns of long-term care of the elderly. Situated in mountain areas, G Town has little farmland, and each household only has 2-3 mu farmland after returning farmland to forest. When farming fails to support their living, young and middle aged farmers will do migrant work. In the dilemma of obtaining higher income and caring the elderly, most people choose the former. Besides, about 86.7% caregivers fall into enormous debt due to building houses. Under such huge pressure, they have to leave the elderly behind.
4.2.2Changes in rural interpersonal relationship. Rural interpersonal relationship is undergoing profound changes. Many caregivers said that they have to employ people to harvest crops in busy farming season, let alone caring the elderly. In answering the question "if village committee and neighbors can provide assistance in caring the elderly", 35.5% people chose "disagree", and 27.6% chose "neither disagree nor agree", showing that neighbors and village committees could provide limited care for the elderly. Our interview also indicated that most families of disabled elderly hope the elderly take care of themselves. However, once there is accident or they get ill, there may be difficulty of first aid and care. Although most families of disabled elderly have low income, their primary concern is no person to look after the elderly.
4.3Shrinkageoffamilycarefunction
4.3.1Family gravity moves downward. Shortage of rural education resources and changes in farmers’ education concept promote more families to invest more funds in children education. This leads to downward movement of family gravity, from respecting the elderly in the past to loving the children at present. Most families focus their effort on education of the next generation, so the input in the elderly care will be lower, and traditional family endowment mode is suffering dramatic impact. However, rural endowment at current stage is still mainly supported by children. After families become smaller, young families prefer living alone to living together with their parents. Especially when young parents live far from original home, their support for the elderly will significantly decline.
4.3.2Huge pressure of caregivers. (i) Heavy duty feeling of long-term care. The feeling is different in the elderly care between short-term care and long term care (longer than 5 years). Long-term care brings huge pressure to caregivers and such pressure increases by geometric progression, as shown in Table 3. (ii) Helplessness in individual care. In our survey, 60.5% individual caregivers felt pressure of long-term care, indicating that there is positive correlation between the feeling of pressure and the number of family member participating in the elderly care. (iii) High input of care renders caregivers not able to arrange their families and work. (iv) Not optimistic prospect of the elderly care. Most caregivers said the physical condition of the elderly is weakening, which makes families face problems of "economic strain", "feeling tire and exhausted", "decline of health condition of caregivers", and "failure to find out effective solutions". Researches have shown that more serious disability of the elderly will bring about greater influence on care time, expenses and daily life, rise of pressure feeling, and depression[5]. Such pressure will in turn exert a great influence of the elderly care.
In sum, due to backward development of rural social endowment security system, changes in rural living environment, weakening of family care function, and vacancy of care, it is necessary and urgent to introduce social support.
Table3Pressureofcaregivers
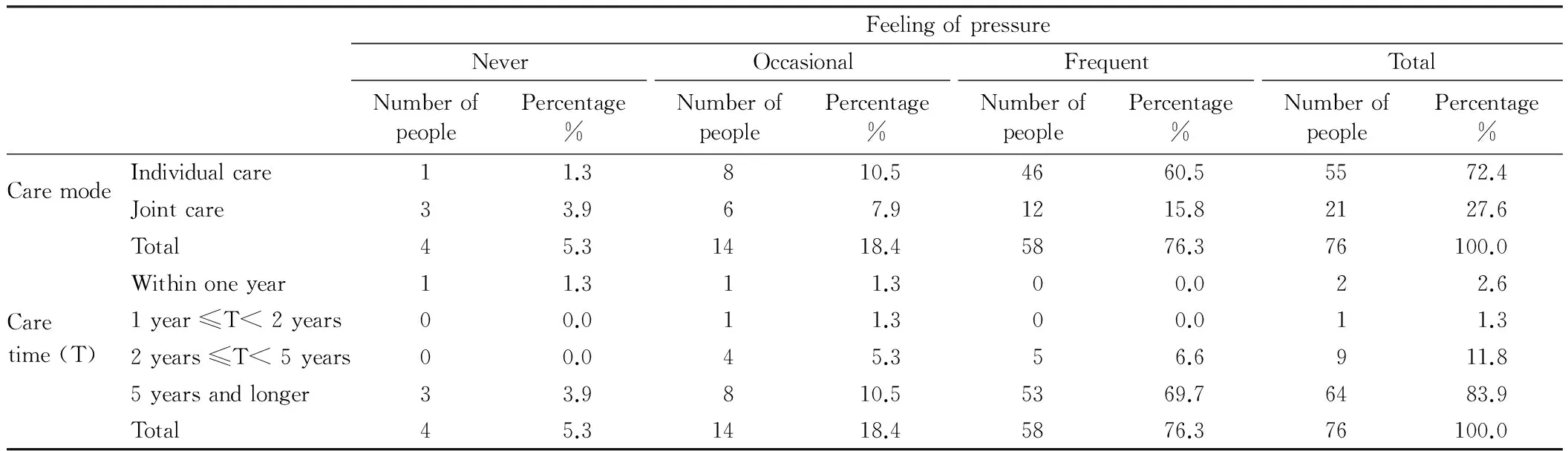
FeelingofpressureNeverNumberofpeoplePercentage%OccasionalNumberofpeoplePercentage%FrequentNumberofpeoplePercentage%TotalNumberofpeoplePercentage%CaremodeCaretime(T)Individualcare11.3810.54660.55572.4Jointcare33.967.91215.82127.6Total45.31418.45876.376100.0Withinoneyear11.311.300.022.61year≤T<2years00.011.300.011.32years≤T<5years00.045.356.6911.85yearsandlonger33.9810.55369.76483.9Total45.31418.45876.376100.0
5 Recommendations
The concept of welfare pluralism was developed in western countries in the 1970s. In the context of rapid developing industrialization and state crisis of welfare, the welfare pluralism is jointly implemented by different departments[6]. Supply of rural endowment services can be jointly implemented by government, market and families. Therefore, it is an effective approach to build a socialized endowment system with joint participation of government, enterprises, non-profit organizations, families and communities.
5.1IncreasinggovernmentinputandspeedingupconstructionofruralendowmentservicesystemGovernment is main supplier of social welfare, so it should be responsible for improving rural endowment environment. The construction of rural endowment service facilities should accord with local situations and be promoted step by step. Firstly, it is recommended to build rural happiness elderly house. Local government should take full advantage of rural community service centers, farmer houses, and idle schools to accelerate the construction of community-based family endowment services. Secondly, it is recommended to extend functions of rural endowment services. For example, it is expected to improve functions of "5 guarantee" endowment service organizations. Under the premise of concentrated endowment of "5 guarantee" endowment in rural areas, it is recommended to support endowment organizations to improve facilities and make them open to the public. Thirdly, we recommend social financing. Relying on local tourist resources and ecological resources, it is recommended to actively build ecological and healthy endowment brands, and attract social capital to enter the endowment service industry. Fourthly, it is recommended to implement preferential taxation system. For example, taxation authorities may exempt endowment organizations from endowment service business taxes, and exempt non-profit endowment organizations from land taxes, and exempt non-profit endowment organizations from business income taxes.
5.2StrengtheningcommunitymanagementandimprovingruralhealthandmedicalsecurityabilityThe endowment of rural disabled elderly lies mainly in solving the problem of medical care. According to provisions of current rural medical insurance, higher reimbursement may only be obtained in the condition of hospitalization. In fact, many disabled elderly can not live without medicines every day. Therefore, it is recommended to improve functions of rural community medical care centers, regularly undertake physical examination, to find out and diagnose diseases as early as possible, control development of diseases, reduce occurrence rate of common diseases and elderly diseases. Secondly, it is recommended to actively promote medical care and endowment combined mode. Health management department should support qualified rural community endowment organizations to set up medical care work stations, to realize prevention, control and care of some common elderly diseases and chronic diseases. Thirdly, it is recommended to establish files of elderly. Community health service organizations should establish health files for the elderly within the community.
5.3Bringingintoplayfunctionsofnon-profitorganizationsandestablishingsupportandassistancesecuritymechanismVolunteer organizations, colleges and universities, and elderly organizations should play an important role in support and assistance. (i) Setting service stations. Non-profit organizations can set up the elderly service center relying on community elderly service center, village elderly activity room, farm book house, to provide medical assistance and catering assistance services for the disabled elderly and provide a platform for communication with the elderly. (ii) Building the endowment service team. It is recommended to encourage various volunteer organizations to develop service activities for rural disabled elderly. First, colleges and universities may take the participation in endowment service volunteer activities as an indicator of overall performance assessment. Second, vocational schools can increase disciplines and courses about endowment services, and accelerate cultivating talents of elderly service management, medical care, nursing and rehabilitation, nutrition matching, and psychological consultation. Third, it is recommended to support elderly team and retired personnel to regularly participation in assistance of disabled elderly. (iii) Realizing network-based management of endowment services. Rural elderly have deep-rooted feeling of home and land, so the family endowment becomes the endowment mode widely accepted by the rural elderly. Gradually promoting network platform of family service is an effective path for realizing family endowment of the elderly. Finally, it is recommended to establish normalized service system. Firstly, setting up information file. Service center may carry out survey on health conditions of rural people older than 60 and establish rural elderly information file. Secondly, establishing contact system. Members of service center should regularly contact disabled elderly and care about physical and psychological conditions of the elderly through interview and visit.
6 Conclusions and discussions
Family is the basic guarantee for the elderly endowment. However, with transformation of economy and society and living style, the whole society is facing with the problem of weakening family endowment functions, and such problem is particularly outstanding in G Town in South Shaanxi. Family endowment needs joint effort of public services and children affection. (i) Local government should undertake the responsibility of providing social welfare, improving community endowment facilities, implementing financial subsidy policy of public welfare endowment, and promote construction of socialized endowment organizations with positive policies. (ii) Communities should strengthen public medical care services and focus on solving problems of endowment and medical care. (iii) It is recommended to encourage non-profit organizations to actively participate in care and services of rural elderly, especially students of colleges and universities, volunteer organizations, elderly teams, and strengthen management and innovation in service type and service system, to provide spiritual consolation and family love. (iv) It is recommended to make effort to promote "simulated family" mode. Volunteers and the elderly establish relatively fixed families. Through effectively consolidating social kindness resources, it is expected to integrate nurses, volunteers, family members, and the elderly, to establish a new endowment mode with "family love service" as basic principle and "happy endowment" as the objective.
[1] XIONG B, SHI RB. The study of decision-making in the care of long time disabled elderly in the personal capital perspective [J]. South China Population, 2012(5): 17-23. (in Chinese).
[2] PAN JH,SHUAI YL, SUN TS,etal. Disability rate and prevalence of China’s elder population [J]. Journal of Nanjing College for Population Programme Management, 2012(4): 3-6. (in Chinese).
[3] ZHAO XH. On the solutions of long-term tending of urban disabled elders [J]. Social Sciences in Guizhou, 2012(10): 129-132. (in Chinese).
[4] HUANG J. On evaluation system of livable communities for the elderly [J]. China Opening Herald, 2016(2): 75-79. (in Chinese).
[5] DU J,QIAN CG,XU W,etal. Depressive symptoms in family caregivers of disabled elderly in Beijing urban[J].Chinese Mental Health Journal, 2014(7): 506-511.(in Chinese).
[6] LU CL, HAN XF. Analysis on the feasibility of rural social endowment under the perspective of welfare pluralism [J].Journal of Hubei Institute for Nationalities(Philosophy and Social Sciences), 2015(1): 52-56.(in Chinese).
杂志排行

Asian Agricultural Research的其它文章
- Empirical Study on the Relationship between Organizational Flexibility and Performance of Agricultural Enterprise
- Correlation between Employment Quality and Skill Training of Land-expropriated Farmers
- A Study on Spatial Distribution of Commercial Housing Prices in Xiangtan City
- Design and Experiment of Fluid Dynamic Ultrasonic Water Aerator
- The Relation between Age Structure of Population and Resident Consumption Based on Endogenous Growth Theory
- Effect of Different Pretreatments on Explosion Puffing Drying of Hami Melon at Modified Temperature and Pressure in Xinjiang