Pathological clavicular fracture as first presentation of renal cell carcinoma: a case report and literature review
2015-12-29YanKongJinWangHuanLiPengGuoJianFaXuHeLinFeng
Yan Kong, Jin Wang, Huan Li, Peng Guo, Jian-Fa Xu, He-Lin Feng
1Department of Medical Oncology, the Fourth Hospital of Hebei Medical University, Shijiazhuang 050011, China;2Department of Orthopedics, the Fourth Hospital of Hebei Medical University, Shijiazhuang 050011, China;3Postgraduate School, Tianjin Medical University, Tianjin 300070, China
CASE REPORT
Pathological clavicular fracture as first presentation of renal cell carcinoma: a case report and literature review
Yan Kong1, Jin Wang2, Huan Li3, Peng Guo2, Jian-Fa Xu2, He-Lin Feng2
1Department of Medical Oncology, the Fourth Hospital of Hebei Medical University, Shijiazhuang 050011, China;2Department of Orthopedics, the Fourth Hospital of Hebei Medical University, Shijiazhuang 050011, China;3Postgraduate School, Tianjin Medical University, Tianjin 300070, China
Renal cell carcinoma (RCC) accounts for approximately 3% of all cancer cases. RCCs usually metastasize to the lungs, bones, liver, or brain. Only <1% of patients with bone metastases manifested clavicular RCC metastases. Tus, clavicular metastasis as the initial presentation of RCC is extremely rare. We report a patient with RCC metastasis to the lef clavicle, which was frst presented with pain caused by a pathological fracture. Magnetic resonance image revealed a renal tumor, and technetium-99m–methylene diphosphonate bone scintigraphy showed multiple osseous metastases. The patient eventually underwent surgery to remove the lateral end of the lef clavicle and right kidney. Histopathology revealed renal tumor and clear cell carcinoma in the clavicle. Finally, we review 17 cases of clavicular metastases originating from diferent malignancies.
Clavicle; metastasis; renal cell carcinoma (RCC); pathological fracture
Introduction
Bone metastasis of renal cell carcinoma (RCC) is not rare but usually located in the spine, the pelvic bones, or the ribs1. A solitary bone metastasis and presented with a pathological fracture in the clavicle is extremely rare, with only a few references in the literature. We report one case of RCC presenting with a solitary clavicular metastasis and review the related literatures, so as to add to knowledge about clavicular metastasis.
Case report
A 64-year-old man was admitted to the Fourth Hospital of Hebei Medical University in January 2014, due to constant pain in the left shoulder after a mild trauma. X-ray and magnetic resonance imaging (MRI) results revealed a pathological clavicular fracture (Figure 1) because no specific, high-energy trauma in the clavicular region was reported and the lesion was osteolytic. Contrast-enhanced computed tomography (CT) and MRI images indicated a tumor, measuring approximately 5 cm × 5 cm, in the right renal cortex. The tumor had spread to the renal capsule (Figure 2). Technetium-99m–methylene diphosphonate bone scintigraphy revealed multiple radioactive foci, indicating multiple osseous metastases in addition to the clavicular metastasis (Figure 3).
The patient underwent surgery to remove the lateral end of the lef clavicle. Histopathology of the clavicle revealed clear cell renal carcinoma (Figure 4). The patient then underwent right nephrectomy, and histopathology showed RCC. Tus, clavicular RCC metastasis was confirmed. The patient was referred to an oncologist and was prescribed sorafenib tosylate and zoledronic acid. The patient was alive and showed no symptoms during a 6-month follow-up period.
Discussion
RCC represents approximately 3% of all cancer cases. Classicsymptom triad comprising hematuria, abdominal mass, and flank pain is found in only 10% of patients. However, RCCs commonly metastasize widely before any symptom is observed1. RCCs typically metastasize to the lungs, bones, liver, or brain, but clavicular involvement is reported in only <1% of all bone metastases1-3. Clavicular metastases are seldom reported. A total of 17 cases of clavicular metastases between 1998 and 2014 are reviewed in this study (Table 1)4-8,10-18. Despite four RCC cases5,15,19which account for 25% of all documented cases, other malignancies rarely metastasize to the clavicle. Kim et al.20studied 4,953 patients with hepatocellular carcinoma, ofwhom only 37 presented bone metastases and only one patient manifested clavicular metastasis. Osseous metastases from primary gastrointestinal cancers are also uncommon, ranging from 5.6% to 7.9%, and they usually occur in the vertebrae, pelvis, sacrum, skull, femur, and humerus21. A single case of malignant epithelioid schwannoma from the trigeminal nerve with clavicular metastasis has been documented, whereas metastases of intracranial gliomas to bones other than the clavicle are more frequent13. Although primary uveal and adnexal cancers rarely metastasize to the clavicle4,13, prostate and thyroid cancers commonly metastasize to this area5,6,12.

Figure 1 X-ray and MRI results of a 64-year-old patient. (A) X-ray result displayed an osteolytic lesion in the lateral third of left clavicle. (B,C) T2-weight MRI to the left clavicle revealed high-intensity lesions.
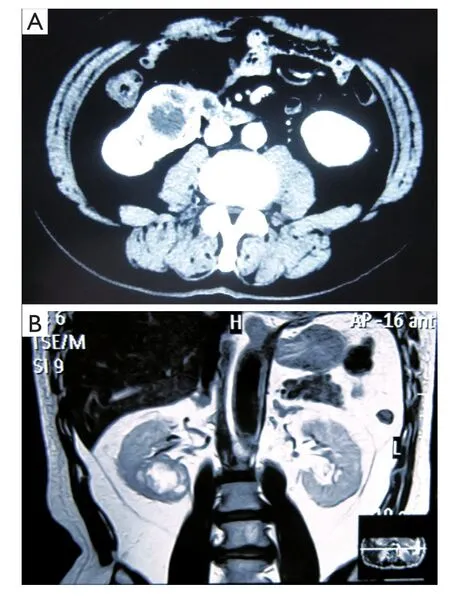
Figure 2 A tumor in the right renal cortex, spreading to the renal capsule. (A) CT. (B) MRI.

Figure 3 Technetium-99m–methylene diphosphonate bone scintigraphy revealed multiple radioactive foci.
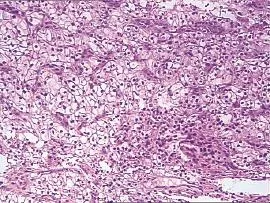
Figure 4 Histopathology of clavicle revealed clear cell carcinoma (H&E staining, 200×).

Table 1 Review of the previously reported cases of clavicular metastasis
Clavicular fractures represent 5% to 10% of all fractures1. Medial clavicular fractures are rare and are normally caused by high-energy traumas, which are frequently due to pathological causes22. Of the 17 cases, 11 had medial clavicular metastases4-7,9-11,13-15,18and two of them revealed clavicular fracture5,9. Clavicular fracture was presented as the frst symptom in four cases5,9,19. Swanson et al.23reported that symptoms caused by bone metastases led to subsequent diagnosis of RCC in 121 of 252 (48%) patients, 37 of whom presented with pathological fractures. Our patient was admitted after a mild trauma that could not have caused clavicular fracture. Tis fracture should be evaluated carefully by physicians and requires routine investigation for an underlying pathological condition. Laboratory tests for measuring prostate-specific antigen, α-fetoprotein, blood calcium, and alkaline phosphatase levels; imaging tests, including radiography, CT, MRI, bone scan, and positron emission tomography; and fine-needle aspiration are essential for the early detection of primary tumors.
In conclusion, clavicular symptoms may be manifested before the diagnosis of primary tumors, such as RCC. Clavicular fracture may be the frst symptom of tumor metastases to bones. Distinguishing pathological fractures from clavicular fractures due to other causes may help diagnose the primary tumors and necessitate whole-body scanning at an early stage.
Conflict of interest statement
No potential conficts of interest are disclosed.
1. Singh J, Baheti V, Yadav SS, Mathur R. Occult renal cell carcinoma manifesting as nasal mass and epistaxis. Rev Urol 2014;16:145-148.
2. Malik SS, Azad S, Malik S, Hing CB. Difculty in diagnosing the pathological nature of an acute fracture of the clavicle: a case report. J Orthop Surg Res 2009;4:21.
3. Ren K, Wu S, Shi X, Zhao J, Liu X. Primary clavicle tumors and tumorous lesions: a review of 206 cases in East Asia. Arch Orthop Trauma Surg 2012;132:883-889.
4. Vartanian SM, Colaco S, Orlof LE, Teodore PR. Oklahoma prosthesis: resection of tumor of clavicle and chest wall reconstructed with a custom composite graf. Ann Torac Surg 2006;82:332-334.
5. Tabuenca Dumortier J, Ortiz Cruz E, Olivas Olivas J. Total cleidectomy for a solitary metastasis of the clavicle. Acta Orthop Belg 2001;67:178-181.
6. Tozum H, Ozkan K, Reddy K, Turkmen I, Ciloglu U, Senol S, et al. Solitary secondary malignant melanoma of clavicle two years afer enuclation for ocular melanoma. Case Rep Orthop 2013;2013:591679.
7. Aliyev A, Ylmaz S, Ozhan M, Asa S, Halac M. FDG PET/CT in the detection of metastases in a patient with Tg and 131I WBS negative follicular thyroid cancer. Clin Nucl Med 2013;38:226-227.
8. Müller S, Khuri FR, Kono SA, Beitler JJ, Shin DM, Saba NF. HPV positive squamous cell carcinoma of the oropharynx. Are we observing an unusual patern of metastases? Head Neck Pathol 2012;6:336-344.
9. Mantonakis EI, Margariti TS, Petrou AS, Stofas AC, Lazaris AC, Papalampros AE, et al. A pathological fracture and a solitary mass in the right clavicle: an unusual frst presentation of HCC and the role of immunohistochemistry. World J Surg Oncol 2012;10:50.
10. Patel NN, Shah PR, Wilson E, Haray PN. An unexpected supraclavicular swelling. World J Surg Oncol 2007;5:90.
11. Sheen AJ, Drake D, Langton S, Sherlock DJ. Unusual bony colorectal metastases in post-hepatometastasectomy patients. J Hepatobiliary Pancreat Surg 2002;9:379-382.
12. Hoshi M, Taguchi S, Hayakawa K, Ieguchi M, Nakamura H. Evaluation of clinical problems associated with bone metastases from carcinoma from unknown primary sites. Arch Orthop Trauma Surg 2011;131:59-64.
13. Caronia FP, Fiorelli A, Zanchini F, Santini M, Lo Monte AI, Castorina S. Reconstruction with a pectoralis major myocutaneous fap afer lef frst rib and clavicular chest wall resection for a metastasis from laryngeal cancer. Gen Torac Cardiovasc Surg 2014. [Epub ahead of print].
14. Ohta M, Hiramoto M, Ohtsuka H. Metastatic microcystic adnexal carcinoma: an autopsy case. Dermatol Surg 2004;30:957-960.
15. Ganapathy K, Ghosh M. Clavicular metastasis from malignant trigeminal schwannoma. J Clin Neurosci 2003;10:485-492.
16. Ceneli O, Haznedar R. Solitary clavicle metastasis in prostate carcinoma. Hell J Nucl Med 2008;11:55-57.
17. Ramos I, González I, Martínez R, Trillo L, Sánchez J. Perioperative management of late metastasis of phaeochromocytoma in clavicle. Eur J Anaesthesiol 2008;25:79-80.
18. Bose SM, Ravindra N, Girdhar G, Bhatacharya A. Clavicular metastasis of insular carcinoma of the thyroid showing increased uptake in the presence of a functioning thyroid gland. Clin Nucl Med 1998;23:774-775.
19. Salapura V, Zupan I, Seruga B, Gasljevic G, Kavcic P. Osteoblastic bone metastases from renal cell carcinoma. Radiol Oncol 2014;48:243-246.
20. Kim SU, Kim do Y, Park JY, Ahn SH, Nah HJ, Chon CY, et al. Hepatocellular carcinoma presenting with bone metastasis: clinical characteristics and prognostic factors. J Cancer Res Clin Oncol 2008;134:1377-1384.
21. Kanthan R, Loewy J, Kanthan SC. Skeletal metastases in colorectal carcinomas: a Saskatchewan profle. Dis Colon Rectum 1999;42:1592-1597.
22. Akasbi N, Elidrissi M, Tahiri L, Elmrini A, Harzy T. An unusual cause of shoulder pain in an elderly woman: a case report. J Med Case Rep 2013;7:271.
23. Swanson DA, Orovan WL, Johnson DE, Giacco G. Osseous metastases secondary to renal cell carcinoma. Urology 1981;18:556-561.
Cite this article as: Kong Y, Wang J, Li H, Guo P, Xu JF, Feng HL. Pathological clavicular fracture as frst presentation of renal cell carcinoma: a case report and literature review. Cancer Biol Med 2015;12:409-412. doi: 10.7497/j.issn.2095-3941.2015.0033
He-Lin Feng
E-mail: fenghelin0311@126.com
Received May 6, 2015; accepted June 24, 2015.
Available at www.cancerbiomed.org
Copyright © 2015 by Cancer Biology & Medicine
杂志排行
Cancer Biology & Medicine的其它文章
- Dermatofibrosarcoma protuberans: from translocation to targeted therapy
- PI3K/Akt/mTOR inhibitors in breast cancer
- Advances in drug delivery system for platinum agents based combination therapy
- Upgrading the definition of early gastric cancer: better staging means more appropriate treatment
- Prognostic value of body mass index before treatment for laryngeal squamous cell carcinoma
- Synergistic suppression of the PI3K inhibitor CAL-101 with bortezomib on mantle cell lymphoma growth