代谢综合征对40 ~ 50岁男性人群前列腺体积的影响
2015-04-11李聪然石炳毅金海龙詹胜利陈昌庆李州利
李聪然,蔡 明,石炳毅,金海龙,詹胜利,陈昌庆,李州利
解放军第309医院 全军器官移植研究所,北京 100091
代谢综合征(metabolic syndrome,MS)是心血管疾病的多种代谢危险因素在个体内集结的状态,包括5个组分:腹型肥胖、高密度脂蛋白降低、高三酰甘油血症、高血压、空腹血糖升高,符合上述4项组成成分中的3项或全部者即可诊断为MS[1-3]。已有研究认为良性前列腺增生(benign prostatic hyperplasia,BPH)和MS存在相关性,这两种疾病都被认为与年龄增大有关,但BPH与MS孰因孰果仍有争议[4-8]。良性前列腺增生的病因尚无定论,目前认为代谢因素可促使BPH的发生和发展。国内外研究者对BPH与生活方式(吸烟、饮酒)[9-11]、肥胖(腰围、臀围及体质量指数)[12-13]、高血压、高密度脂蛋白胆固醇(high-density lipoprotein cholesterol,HDL-C)、低密度脂蛋白胆固醇及高三酰甘油血症)[14-17]的关系进行了广泛性研究,但报道结果不一。前列腺体积(prostate volume,PV)的变化常始于男性40岁后,至50岁时BPH发病率可达40%[18-20]。然而40 ~ 50岁男性前列腺体积与代谢综合征的关系少有报道。我们通过分析本院体检中心438例男性体检数据,进一步揭示MS对前列腺体积的影响,为临床治疗提供依据。
资料和方法
1 一般资料 选取2010年1月- 2013年12月本院体检中心40 ~ 50岁男性438例,回顾性分析体检数据,包括经腹部前列腺超声所测体积、血糖、血脂、血压、腰围、体质量指数、高密度脂蛋白等。
2 入组标准及分组 MS诊断依据中华医学会糖尿病学分会2004年标准,即具备以下4项中的3项或4项者:1)腹型肥胖:腰围>90 cm或体质量≥25.0 kg/m2;2)高血糖:空腹血糖(fasting blood glucose,FBG)≥6.1 mmol/L和(或)餐后2 h血糖≥7.8 mmol/L,和(或)确诊为糖尿病并接受治疗的患者;3)高血压:收缩压/舒张压≥140/90 mmHg(1 mmHg=0.133 kPa),和(或)已确诊高血压并接受治疗的患者;4)血脂水平紊乱:空腹血三酰甘油(triglyceride,TG)≥1.7 mmol/L,和(或)空腹血糖HDL-C≤1.04 mmol/L。根据上述标准将438例体检者分为MS组及非MS组;FBG≥6.1 mmol/L为FBG异常组,FBG<6.1 mmol/L为FBG正常组;HDL-C≤1.04 mmol/L为HDL-C异常组,HDL-C>1.04 mmol/L为HDL-C正常组;腰围>
90 cm为腰围异常组,腰围≤90 cm为腰围正常组;根据血压分为高血压组与正常血压组。
3 前列腺体积检查 在询问受检者既往史基础上经腹部超声测量前列腺体积,患者于空腹憋尿状态下,采用彩色多普勒超声诊断仪(SSD-4000SV型)经腹测定前列腺的最大左右径、上下径及前后径,根据公式得到前列腺体积:PV=前列腺纵径×横径×前后径×0.52。
4 统计学方法 用SPSS V11.0统计学软件处理,计量资料以±s表示。组间样本采用t检验或方差分析,多组间的多个样本均数比较采用Kruskal-Wills检验,双变量相关分析采用Pearsonχ2检验。Logistic回归分析检验MS各组分对PV的影响。P<0.05为差异有统计学意义。
结 果
1 一般资料比较 438例体检者平均年龄(46.65± 3.29)岁。其中40 ~ 45岁男性198例,46 ~ 50男性240例。所有体检者PV平均值为(18.60±6.26) cc,MS各组分相关指标见表1。
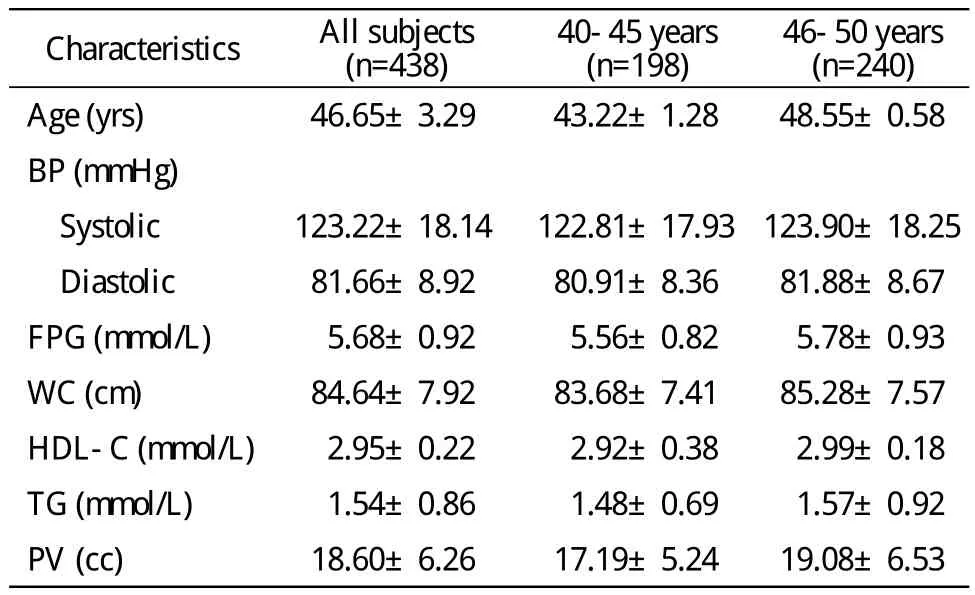
表1 不同年龄组代谢因素和前列腺体积Tab.1 Comparison of metabolic factors and prostate volume according to different age groups

表2 代谢综合征及其相关因素对前列腺体积的影响Tab. 2 Comparison of prostate volume according to MS and MS parameters
2 MS对PV的影响 438例中MS 89例,非MS 349例,MS患病率20.32%。MS组前列腺体积明显大于非MS组(P<0.05)。根据受检者年龄分亚组示:40 ~ 45岁MS组前列腺体积与非MS组差异无统计学意义(P>0.05),46 ~ 50岁MS组前列腺体积大于非MS组(P<0.05)。MS不同年龄组的腹型肥胖、空腹血糖异常与前列腺体积增大显著相关(P<0.05),而BP、HDL-C、TG等组分与前列腺体积无相关性。见表2。
3 Logistic多因素分析 以参检者PV体积>20 cc为因变量,不同年龄段MS所有组分为自变量,分析各组分与PV关系。Logistic分析发现,空腹血糖异常与腹型肥胖与前列腺体积>20 cc显著相关。见表3。

表3 不同年龄组中前列腺体积>20 cc情况下Logistic回归分析Tab. 3 Independent predictors of enlarged prostate volume (>20 cc) using multiple logistic regression analysis according to different age groups
讨 论
良性前列腺增生是全球老年男性的常见疾病,根据前列腺增生发生的部位不同,出现的临床症状也不同[8]。随着人民生活水平及卫生保健条件的不断提高,人们的人均寿命随之延长,人口的老龄化使得与年龄相关的BPH患病率逐年增高。研究表明,前列腺增生发病率将随着年龄增长而升高,其中80 ~ 90岁男性发病率高达80%以上,是泌尿外科最常见疾病之一[3-4]。
有报道表明,MS成年人发病率为2.4% ~ 43.5%,与BPH一样随年龄增长发病率呈增高趋势,且MS与BPH相关[4-8]。BPH流行病学研究结果显示,年龄与生活方式的改变所造成的内环境紊乱,即代谢紊乱,能促成BPH的发病增加[21-23]。BPH始于男性40岁左右,然而40 ~ 50年龄段男性的PV与MS有无相关性及相关程度如何少有研究。
我们的研究结果发现,在46 ~ 50岁男性中,MS与PV具有相关性,尤其MS组分FPG、WC与40~50岁男性前列腺体积显著相关。以往研究同样发现糖尿病患者或肥胖患者PV较对照组明显增大,我们的研究结果同样显示了这样的相关性。因此对于血糖异常或肥胖的40 ~ 50岁男性而言,要注意BPH。
1 Halpern A, Mancini MC, Magalhães ME, et al. Metabolic syndrome,dyslipidemia, hypertension and type 2 diabetes in youth: from diagnosis to treatment[J]. Diabetol Metab Syndr, 2010, 2:55.
2 Roberts CK, Hevener AL, Barnard RJ. Metabolic syndrome and insulin resistance: underlying causes and modification by exercise training[J]. Compr Physiol, 2013, 3(1): 1-58.
3 Weiss R, Bremer AA, Lustig RH. What is metabolic syndrome, and why are children getting it?[J]. Ann N Y Acad Sci, 2013, 1281:123-140.
4 Abdollah F, Briganti A, Suardi N, et al. Metabolic syndrome and benign prostatic hyperplasia: evidence of a potential relationship,hypothesized etiology, and prevention[J]. Korean J Urol, 2011,52(8):507-516.
5 Parsons JK, Carter HB, Partin AW, et al. Metabolic factors associated with benign prostatic hyperplasia[J]. J Clin Endocrinol Metab, 2006, 91(7):2562-2568.
6 Stamatiou K, Lardas M, Kostakos E, et al. The impact of diabetes type 2 in the pathogenesis of benign prostatic hyperplasia: a review[J/ OL]. http://www.hindawi.com/journals/au/2009/818965.
7 Corona G, Vignozzi L, Rastrelli G, et al. Benign prostatic hyperplasia: a new metabolic disease of the aging male and its correlation with sexual dysfunctions[J/OL]. http://www.hindawi. com/journals/ije/2014/329456.
8 Park YW, Min SK, Lee JH. Relationship between Lower Urinary Tract Symptoms/Benign Prostatic Hyperplasia and Metabolic Syndrome in Korean Men[J]. World J Mens Health, 2012, 30(3):183-188.
9 Williams PT. Effects of running distance and performance on incident benign prostatic hyperplasia[J]. Med Sci Sports Exerc, 2008, 40(10): 1733-1739.
10 Simpson RJ, Lee RJ, Garraway WM, et al. Consultation patterns in a community survey of men with benign prostatic hyperplasia[J]. Br J Gen Pract, 1994, 44(388):499-502.
11 St Sauver JL, Jacobsen SJ, Jacobson DJ, et al. Statin use and decreased risk of benign prostatic enlargement and lower urinary tract symptoms[J]. BJU Int, 2011, 107(3):443-450.
12 Yoo TK, Cho HJ. Benign prostatic hyperplasia: from bench to clinic[J]. Korean J Urol, 2012, 53(3):139-148.
13 Patel ND, Parsons JK. Epidemiology and etiology of benign prostatic hyperplasia and bladder outlet obstruction[J]. Indian J Urol,2014, 30(2):170-176.
14 Sarma AV, St Sauver JL, Hollingsworth JM, et al. Diabetes treatment and progression of benign prostatic hyperplasia in community-dwelling black and white men[J]. Urology, 2012, 79(1): 102-108.
15 Lee SH, Oh CY, Park KK, et al. Comparison of the clinical efficacy of medical treatment of symptomatic benign prostatic hyperplasia between normal and obese patients[J]. Asian J Androl, 2011, 13(5):728-731.
16 Gorbachinsky I, Akpinar H, Assimos DG. Metabolic syndrome and urologic diseases[J]. Rev Urol, 2010, 12(4):e157-e180.
17 Parsons JK. Benign Prostatic Hyperplasia and Male Lower Urinary Tract Symptoms: Epidemiology and Risk Factors[J]. Curr Bladder Dysfunct Rep, 2010, 5(4):212-218.
18 Nicholson TM, Ricke WA. Androgens and estrogens in benign prostatic hyperplasia: past, present and future[J]. Differentiation,2011, 82(4-5):184-199.
19 Emberton M, Cornel EB, Bassi PF, et al. Benign prostatic hyperplasia as a progressive disease: a guide to the risk factors and options for medical management[J]. Int J Clin Pract, 2008, 62(7):1076-1086.
20 Skolarus TA, Wei JT. Measurement of benign prostatic hyperplasia treatment effects on male sexual function[J]. Int J Impot Res,2009, 21(5): 267-274.
21 Hatzimouratidis K. A review of the use of tadalafil in the treatment of benign prostatic hyperplasia in men with and without erectile dysfunction[J]. Ther Adv Urol, 2014, 6(4):135-147.
22 Manchanda PK, Kibler AJ, Zhang M, et al. Vitamin D receptor as a therapeutic target for benign prostatic hyperplasia[J]. Indian J Urol, 2012, 28(4):377-381.
23 Nakanishi Y, Masuda H, Kawakami S, et al. A novel equation and nomogram including body weight for estimating prostate volumes in men with biopsy-proven benign prostatic hyperplasia[J]. Asian J Androl, 2012, 14(5): 703-707.
