急性脑梗死阿替普酶静脉溶栓后血管再闭塞应用低分子肝素钙的价值
2015-03-24朱立勋耿瑞慧陆学胜李克良丁素菊
朱立勋,耿瑞慧,陆学胜,李克良,丁素菊
急性脑梗死阿替普酶静脉溶栓后血管再闭塞应用低分子肝素钙的价值
朱立勋1,耿瑞慧2,陆学胜1,李克良1,丁素菊3
目的 探讨低分子肝素钙对急性脑梗死阿替普酶静脉溶栓后血管再闭塞患者的应用价值。方法 收集2010-2014年上海市同仁医院神经内科收治的经阿替普酶静脉溶栓后血管再闭塞的44例急性脑梗死患者资料,根据是否采用低分子肝素钙,分为抗凝组和对照组,抗凝组23例,对照组21例。评价两组治疗后1、14、90 d的疗效,包括神经功能缺损评分(NIHSS)及mRS评分,同时观察90 d内再脑出血发生率及病死率。结果 抗凝组和对照组14 d总有效率分别为78.3%、42.9%,差异有统计学意义(P<0.05);90 d mRS评分分别为2.00±1.51、3.10±1.76,差异有统计学意义(P<0.05)。抗凝组和对照组脑出血(症状性脑出血+非症状性脑出血)发生率分别为17.4%、14.3%,病死率分别为8.7%、9.5%,两组比较,差异均无统计学意义。结论 低分子肝素钙治疗阿替普酶溶栓后血管再闭塞,可改善患者神经功能,效果满意。
急性缺血性卒中;阿替普酶;溶栓;再闭塞;低分子肝素钙
继欧洲心脏协会及美国卒中协会(ASA)之后,我国2010 年脑血管病防治指南,对于发病4.5 h以内的急性缺血性脑卒中患者建议使用重组组织型纤溶酶原激活物(阿替普酶)静脉溶栓治疗[1-3]。然而,静脉溶栓后早期再通血管中约有14%的病例会发生再闭塞而导致预后不良[2],而对溶栓患者是否联合应用抗凝药物治疗尚未取得一致意见[4]。低分子肝素钙是由普通肝素解聚而成,具有快速持续的抗血栓效果,不良反应少,广泛应用于急性脑梗死患者。本研究对行阿替普酶静脉溶栓过程中症状加重患者的临床资料进行回顾性分析,探索低分子肝素钙是否能够改善患者的预后。
1 资料与方法
1.1 资料来源 收集从2010-11至2014-11在上海市同仁医院神经内科住院并接受阿替普酶静脉溶栓治疗,且发生血管再闭塞的急性缺血性卒中患者资料。均符合全国第四届脑血管病会议制定的脑梗死诊断标准[5]。血管再闭塞的定义:静脉溶栓过程中起初获得部分或完全再通的血管,复查头颅或颈部MRA显示在其原闭塞的部位发生再次闭塞或头颅DWI显示分水岭区新出现点状脑梗死[5]。本试验疗效评价采用美国国立卫生研究院卒中量表(NIHSS) , 溶栓后评分减少3分以上为血管再通的标准, 症状加重后评分再次增高2分以上为血管再闭塞的标准[6]。
阿替普酶静脉溶栓的适应证及禁忌证综合采用2007年美国成人缺血性卒中急性期处理指南及2008年欧洲协作性急性卒中研究(European cooperative acute stroke study,ECASS) Ⅲ制定的标准[7]。溶栓入选标准:(1)年龄18~80岁;(2)发病至给药时间在4.5 h内;(3)NIHSS≥4分;(4)脑功能损害的体征持续存在超过1 h;(5)头颅CT排除颅内出血,且无早期大面积脑梗死影像学改变;(6)溶栓前/后均行头颅MRI、DWI、FLAIR检查;(7)均为TOAST分型中大动脉粥样硬化型;(8)患者或家属签署知情同意书。 溶栓排除标准:(1)有出血病史,包括既往有颅内出血病史或3个月之内有头颅外伤史、3周内有泌尿道或胃肠出血史、近2周内有外科手术病史、1周内有在不易压迫止血部位的动脉穿刺术;(2)近3个月内有心肌梗死或脑梗死病史,且mRS评分<2分,但不包括陈旧性腔隙性脑梗死;(3)严重心、肾、肝功能不全或严重糖尿病患者;(4)体检发现有外伤(如骨折)或活动性出血的证据;(5)已口服抗凝药,且INR>1.5,或48 h内接受过肝素治疗(APTT超出正常范围);(6)血小板计数低于100×1012;(7)血糖<2.7 mmol/L;(8)收缩压>180 mmHg,或舒张压>100 mmHg;(9)妊娠者;(10)卒中发作时伴有癫痫。
1.2 指标 收集年龄、性别、高血压史、糖尿病史、发病前是否有抗血小板药物应用、溶栓前血压、溶栓前血糖,以及溶栓前及溶栓后24 h、14 d的NIHSS评分,90 d改良Rankin量表(mRS)、脑出血及死亡例数,以及溶栓后症状加重是否应用低分子肝素钙等。根据NIHSS评分计算神经功能改善率:神经功能改善率(%)=(治疗前总分-治疗后总分)/治疗前总分×100%。14 d后疗效判定:(1)基本痊愈,神经功能改善率91%~100%;(2)显著进步,神经功能改善率46%~90%;(3)进步,神经功能改善率18%~45%;(4)无变化,神经功能改善率17%以内;(5)恶化,神经功能缺损评分增加18%以上;(6)死亡。总有效率(%)=(基本痊愈+显著进步+进步)/总例数×100%。脑出血发生率(%)=(3个月内发生的脑出血例数)/总例数×100%。病死率(%)=(3个月内死亡例数)/总例数×100%。3个月预后生活自理定义为mRS≤2分[2]。

2 结 果
2.1 一般情况 44例中,抗凝组23例,对照组21例。两组性别、年龄、吸烟史、高血压病史、糖尿病史、脑梗死病史、发病前服用抗血小板药物史、血生化及溶栓前NIHSS评分等基线资料比较,差异均无统计学意义(表1)。

表1 急性脑梗死阿替普酶静脉溶栓后是(抗凝组)否(对照组)采用低分子肝素钙患者溶栓前资料比较 ±s;(n,%)]
2.2 疗效 抗凝组与对照组溶栓后24 h NIHSS评分比较, 差异无统计学意义;14 d后两组NIHSS评分以及90 d后mRS评分比较,抗凝组均低于对照组,差异有统计学意义(P<0.05,表2)。14 d 后抗凝组疗效好于对照组,且总有效率高于对照组(表3),90 d抗凝组生活自理率78.26%,对照组47.61%,前者高于后者(χ2=4.45,P=0.035)。90 d内抗凝组脑出血4例(17.4),死亡2例(8.7);对照组脑出血3例(14.3),死亡2例(9.5);两组比较,差异均无统计学意义。

表2 急性脑梗死阿替普酶静脉溶栓后是(抗凝组)否(对照组)采用低分子肝素钙患者溶栓后评分情况 ±s)
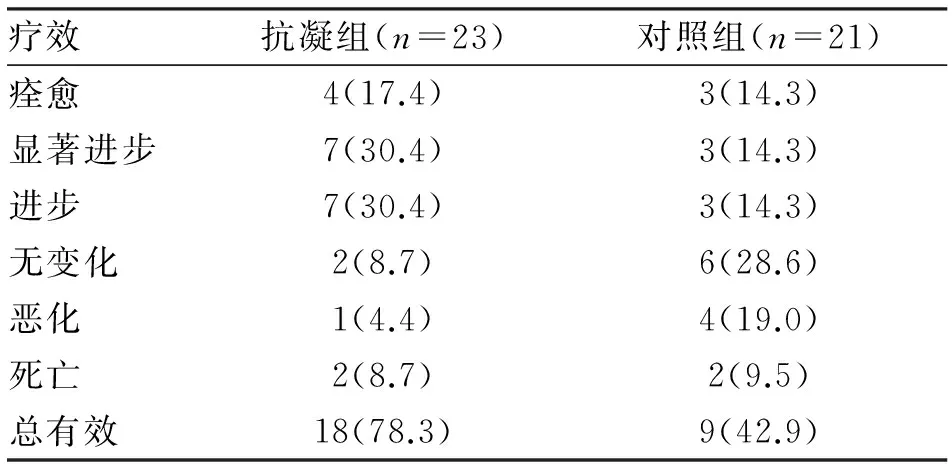
表3 急性脑梗死阿替普酶静脉溶栓后是(抗凝组)否(对照组)采用低分子肝素钙患者溶栓后14 d疗效比较 (n;%)
注:两组总有效率比较,χ2=5.803,P=0.016
3 讨 论
急性脑梗死在阿替普酶溶栓的同时,血管内溶栓局部形成高凝状态,并且随着栓子的“崩解”,容易形成脑分水岭区的动脉微栓子而堵塞远端血管,进而形成微循环障碍,使部分患者临床症状加重[8]。临床研究发现,脑梗死早期临床症状恶化的主要原因是血管再闭塞[9]。低分子肝素钙是由普通肝素解聚而成,不但有显著的抗凝血因子Xa 活性,而且有降低纤维蛋白原浓度,抑制红细胞聚集,从而降低血液黏度作用,以及促进侧支循环形成的作用[10]。可以推测,对于行阿替普酶溶栓后症状加重的患者,及时给予低分子肝素钙应能改善病情。
本研究发现,抗凝组和对照组溶栓前一般资料比较,均无统计学差异。两组14 d后NHISS评分均有改善,但抗凝组总体效果明显好于对照组。90 d后不管是mRS评分还是生活自理能力,抗凝组均优于对照组。说明抗凝组症状体征的改善与低分子肝素钙的抗凝作用相关。
在安全性方面,根据溶栓后症状性脑出血(symptomatic intracranial hemorrhage after stroke thrombolysis,SEDAN)评分系统[11]预测指标,脑梗死严重程度、高龄、高血压、入院时高血糖等是脑出血转化的预测指标。在试验设计上,上述基线资料两组患者无差异,而两组患者的脑出血发生率及脑死亡率无统计学差异。已有研究证实抗凝治疗是脑出血转化的独立危险因素之一[12,13],但本研究表明,抗凝治疗对溶栓后血管再闭塞患者的出血风险无明显增加,由于该试验样本量小,还需在后续研究中,扩大样本量进一步研究。
通过本研究,对于行阿替普酶静脉溶栓症状一过性加重,并排除其他因素后考虑动脉血管再闭塞的患者,行低分子肝素钙抗凝治疗可改善预后。由于本试验样本量小,应用抗凝药物在治疗血管再闭塞的安全性方面还需扩大样本量进一步研究。
[1] 中华医学会神经病学分会脑血管病学组指南协作组. 2010 中国急性缺血性卒中诊治指南[J]. 中华神经科杂志,2010,43(2):146-154.
[2] Hacke W, Kaste M, Bluhmki E,etal. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke [J]. New England Journal of Medicine, 2008,359(13):1317-1329.
[3] Furie K L, Kasner S E, Adams R J,etal. American Heart Association Stroke Council, Council on Cardiovascular Nursing, Council on Clinical Cardiology, and Interdisciplinary Council on Quality of Care and Outcomes Research. Guidelines for the prevention of stroke in patients with stroke or transient ischemic attack: a guideline for healthcare professionals from the American Heart Association/American Stroke Association [J]. Stroke, 2011, 42(1):227-276.
[4] Fulgham J R, Ingall T J, Stead L G,etal. Management of acute ischemic stroke [J]. Mayo Clin Proc, 2004,79(11):1459-1469.
[5] Heo J H, Lee K Y, Kim S H,etal. Immediate re-occlusion following a successful thrombolysis in acute stroke: a pilot study [J]. Neurology, 2003,60(10):1684-1687.
[6] Grotta J C, Welch K M A, Fagan S C,etal. Clinical deterioration following improvement in the NINDS rt-PA Stroke Trial [J]. Stroke, 2001,32(3):661-668.
[7] Adams H P, Del Zoppo G, Alberts M J,etal. Guidelines for the Early Management of Adults With Ischemic Stroke A Guideline From the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: The American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists[J]. Circulation, 2007,115(20):e478-e534.
[8] Toyoda K, Okada Y, Kobayashi S. Early recurrence of ischemic stroke in Japanese patients: the Japan standard stroke registry study [J]. Cerebrov Dis, 2006,24(2-3):289-295.
[9] Alexandrov A V, Grotta J C. Arterial re-occlusion in stroke patients treated with intravenous tissue plasminogen activator[J]. Neurology, 2002,59(6):862-867.
[10] Straub S, Junghans U, Jovanovic V,etal. Systemic thrombolysis with recombinant tissue plasminogen activator and tirofiban in acute middle cerebral artery occlusion[J]. Stroke, 2004,35(3):705-709.
[11] Lyden P D. Stroke: Haemorrhage risk after thrombolysis—the SEDAN score [J]. Nature Reviews Neurology, 2012,8(5):246-247.
[12] Group I S T C. The International Stroke Trial (IST): a randomised trial of aspirin, subcutaneous heparin, both, or neither among 19 435 patients with acute ischaemic stroke [J]. Lancet, 1997,349(9065):1569-1581.
[13] Chen Z M. CAST: randomised placebo-controlled trial of early aspirin use in 20,000 patients with acute ischaemic stroke. CAST (Chinese Acute Stroke Trial) Collaborative Group [J]. Lancet, 1997,349(9066):1641-1649.
(2015-02-20收稿 2015-04-08修回)
(责任编辑 武建虎)
Application value of low molecular weight heparin calcium in treatment of re-occlusion patients in process of thrombolysis with alteplase
ZHU Lixun1, GENG Ruihui2, LU Xuesheng1, LI Keliang1, and DING Sujv3.
1.Department of Neurology, Shanghai Tongren Hospital, Shanghai 200336, China;2.Department of Neurology, Hospital of Corps 8640, Chinese People’s Armed Police Forces, Dingzhou 073000, China;3.Department of Neurology, Changhai Hospital of Second Military Medical University, Shanghai 200433, China
Objective To study application value of the low molecular weight heparin calcium in re-occlusion patients in the process of thrombolysis with alteplase. Methods Forty-four patients with acute cerebral infarction admitted into this hospital in 2010-2014 were divided into observation group(n=23) and control groups(n=21).The former received low molecular weight heparin calcium combined with alteplase.The outcome scores were evaluated according to the National Institute of Heath Stroke Scale(NIHSS) before treatment and 1 d, 14 d after thrombolysis,the modified Rankin Scale (mRS) score after thrombolysis 90 d were observed,and the mortality, hemorrhagic transformation as the safety indicators were evaluated. Results There were significant differences in efficacy outcome rate (78.3%, 42.9%, respectively) between the two groups at 14 days (P<0.05). There were no significant differences between the two groups in the incidence of mortality and cerebral hemorrhage (symptomatic and non-symptomatic intracerebral hemorrhage) at 90 d. There were significant differences between the two groups at 90 d in mRS score (2.00±1.51, 3.10±1.76, respectively,P<0.05). Conclusions The treatment of the low molecular weight heparin calcium combined with alteplase in patients with aggravation of signs and symptoms in the process of thrombolysis can improve neurological function with satisfactory results.
acute cerebral infarction;alteplase;thrombolysis;re-occlusion;low molecular weight heparin calcium
朱立勋,硕士,主治医师,E-mail: zhulixun2011@sina.com
1.200336,上海市同仁医院神经内科;2.073000 定州,武警8640部队医院内一科;3.200433 上海,第二军医大学附属长海医院神经内科
陆学胜,E-mail:lxssh@126.com
R743.3
