医生-护士-药师协作干预心血管疾病疗效的系统评价β
2015-03-03苏娜,罗敏,徐
苏 娜,罗 敏,徐
(四川大学华西医院药剂科,四川 成都 610041)
医生-护士-药师协作干预心血管疾病疗效的系统评价β
苏 娜,罗 敏,徐
(四川大学华西医院药剂科,四川 成都 610041)
目的系统评价医生 -护士-药师协作干预心血管疾病患者治疗效果。方法计算机检索 MEDLINE,EMbase,CENTRAL,WanFang,CNKI,VIP数据库,查找医生-护士-药师协作干预心血管疾病患者的随机对照试验(RCT),检索时限截至2015年3月。采用RevMan 5.3.0软件进行Meta分析。结果最终纳入12个RCT。协作组较常规组显著降低患者收缩压和舒张压[RR=-0.41,95% CI(-0.68,-0.14),P=0.003]和[RR=-0.10,95%CI(-0.14,-0.06),P<0.000 01];协作组较常规组显著降低患者的总胆固醇[RR=-0.44,95%CI(-0.72,-0.16),P=0.002]。两组患者的病死率和住院率,差异无统计学意义(P>0.05)。结论医生-护士-药师协作对于心血管疾病患者的血压和血脂控制有效,但远期疗效有待更多高质量、大样本、长期随访的RCT加以验证。
医生;护士;药师;协作;系统评价。
全世界超过1/3的25岁以上成年人受到高血压的影响,每年高血压导致900多万人死亡,其中半数死于心脏病和中风[1]。预计到2030年,有2 330万人将死于心血管疾病[2-3]。2007年,我国首次引进多学科协作模式(multi-discipinary team,MDT)[4],这是一种国际新型的团队合作医疗模式。通过欧美的多年实践[5],认为其是一种系统化、模式化的临床医疗方式。我国传统的医疗模式是医生与护士合作,对患者进行治疗干预。但随着我国临床药学的发展,临床药师越来越多地参与联合诊疗,提供用药咨询服务,促进合理用药。国内外已经开展了一些关于药师参与医疗团队的治疗效果研究,但研究结论不一致。有研究认为,有药师参与的联合诊疗能改善患者的预后,提高药物疗效[6-7]。但是也有一些研究[8-9]认为,药师在临床医疗团队中所起作用很小,甚至对患者的结局指标起消极作用。本研究中拟通过循证医学方法,评价国内外医生-护士-药师(physicians-nurses-pharmacists,PNP)协作干预心血管疾病疗效研究的文献。
1 资料与方法
1.1 文献的纳入和排除标准
纳入标准:随机对照试验(RCT);心血管疾病包括高血压、高血脂、心脏病等;PNP协作干预对比常规干预措施(药师未与医生和护士相互协作);结局指标为血压、血脂、死亡率、住院率。排除标准:非RCT;非PNP协作干预;重复报道;报道信息量太少以至于无法利用;会议。
1.2 检索策略、资料提取与方法学质量评价
以“physicians”“nurses”“pharmacists”“collaboration”“医生”“护士”“药师”“合作”为检索词,检索Cochrane图书馆(2015年第1期),MEDLINE(Ovid SP,1946~),Embase(1974~),CNKI(1978~),VIP(1989~),WanFang(1986~),检索时限均截至2015年3月;手工检索其他相关杂志。此外,追溯已纳入文献和相关综述的参考文献。文献检索结果以数据库形式保存,采用量表方式提取文献基本信息。由2名研究者根据纳入与排除标准独立筛选文献、提取资料并评价质量,然后交叉核对,必要时致电原文作者以确定试验具体实施过程,如遇发生分歧讨论解决或交由第3名研究者协助裁定。按照Cochrane偏倚风险评估工具(5.1.0)对纳入研究的方法学质量进行评价[10]。
1.3 统计分析
采用由Cochrane协作网提供的RevMan 5.3软件进行Meta分析。分类变量采用相对危险度(RR)为疗效分析统计量,各效应量均以95%CI表示,并绘制森林图,以α=0.05为检验水准[11]。首先,采用 χ2检验对纳入研究进行异质性检验(临床异质性和方法学异质性),同时根据 I2判断异质性的大小,I2≤25%为低度异质性,25%<I2<50%为中度异质性,I2≥50%则为高度异质性[12]。若各纳入研究结果同质性好(P>0.1,I2<50%),则采用固定效应模型进行 Meta分析,反之则采用随机效应模型进行Meta分析。根据异质性产生原因对各研究进行亚组分析。必要时,行敏感性分析。对于无法合并的指标行描述性分析。
2 结果
2.1 文献检索结果及纳入文献特征
文献筛选初检出3 093篇英文文献和30篇中文文献,经逐层筛选,最终纳入12个RCT[13-24],均为英文文献,见表1。共纳入心血管疾病患者8 930例,包括高血压,高血脂和心力衰竭。文献描述性分析结果见表2。

表1 纳入研究的基本信息
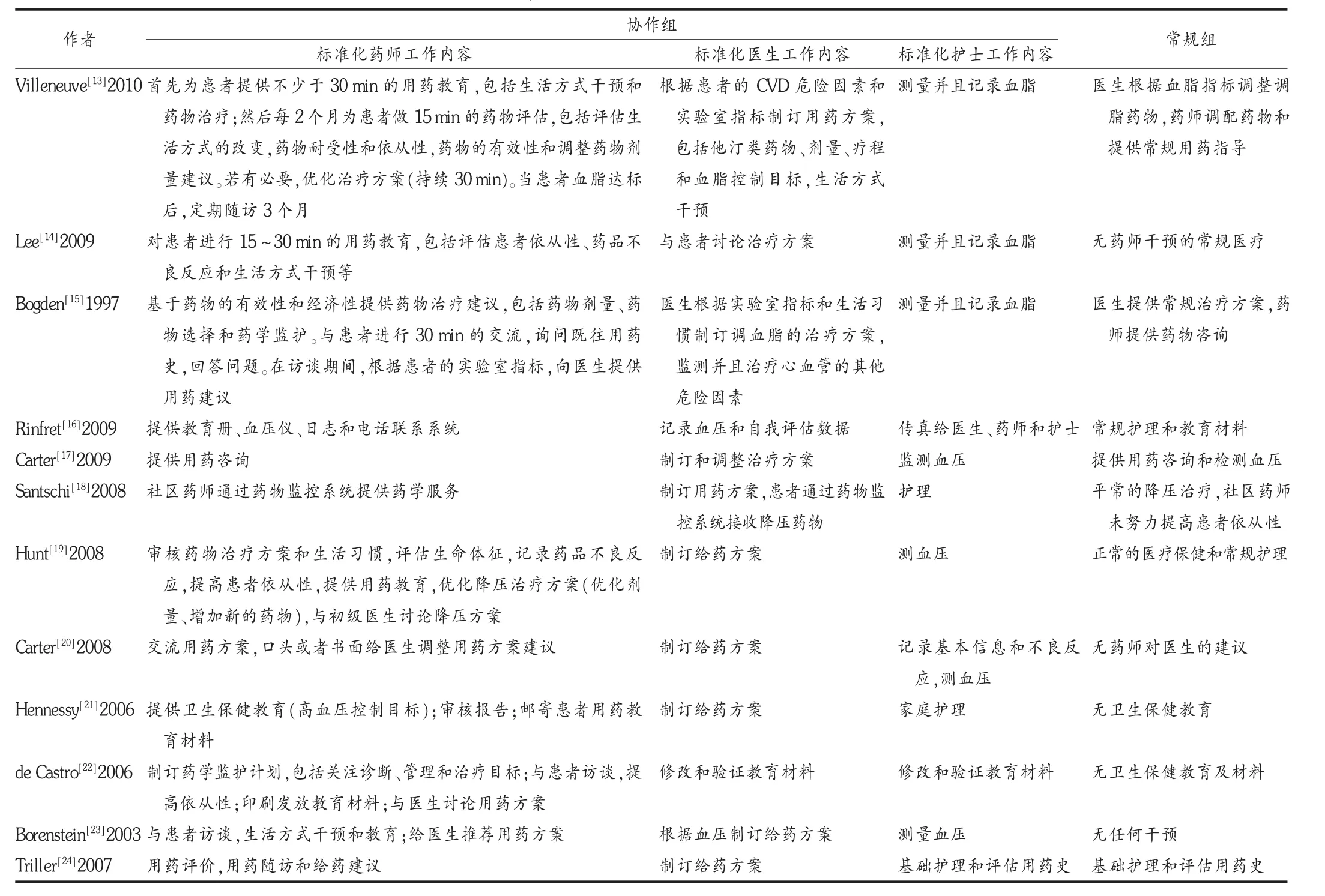
表2 纳入文献的描述性特征
2.2 纳入研究的方法学质量评价
12个 RCT中,有 9个 RCT[13-20,22]应用随机数字法表进行随机分配,判定为“低偏倚”;其他研究均在文中提及“随机”而未进行详细描述,判定为“不清楚”。2个RCT[20,22]提及“双盲”,判定为“低偏倚”。只有 7个 RCT[13-16,19-20,22]提及盲数据分析者,判定为“低偏倚”。5个 RCT[13-15,19-20]提及分配隐匿的方法,判定为“低偏倚”。2个 RCT[13-14]提及“不完整数据”。6个 RCT[13-14,16-19]选择性报道是“低偏倚”,2个RCT[14,19]无“其他偏倚”。
2.3 有效性评价
SBP:有 9个 RCT[13,15,17-23]报道。Meta分析结果显示,协作组SBP降低优于常规组[RR=-0.41,95%CI(-0.68,-0.14),P=0.003],见图1。
DBP:有 9个 RCT[13,15,17-23]报道。Meta分析结果显示,协作组DBP降低优于常规组[RR=-0.10,95%CI(-0.14,-0.06),P<0.000 01],见图2。
TC:有2个RCT[13,15]报道。Meta分析结果显示,协作组TC降低优于常规组[RR=-0.44,95%CI(-0.72,-0.16),P=0.002],见图3。
LDL-C:有2个RCT[13-14]报道。Meta分析结果显示,协作组LCL-C低虽优于常规组,但差异无统计学意义[RR=-2.04,95%CI(-5.51,1.43),P=0.25],见图4。
HDL-C:有 2个 RCT[13-14]报道。Meta分析结果显示,协作组HDL-C降低劣于常规组,但差异无统计学意义[RR=0.20,95%CI(-0.05,0.45),P=0.12],见图5。
TG:有2个 RCT[13-14]报道。Meta分析结果显示,协作组 TG降低虽优于常规组,但差异无统计学意义[RR=-0.92,95%CI(-2.75,0.90),P=0.32],见图6。
死亡率和住院率:1个 RCT[24]纳入心力衰竭患者,研究结果显示协作组和常规组患者死亡率分别为22.08%(17/77)和18.18% (14/77),差异无统计学意义(P=0.67)。住院率分别为 54.55%(42/77)和 58.44%(45/77),差异无统计学意义(P=0.63)。

图1 PNP协作组与常规组患者SBP变化的Meta分析

图2 PNP协作组与常规组患者DBP变化的Meta分析

图3 PNP协作组与常规组患者总TC变化的Meta分析

图4 PNP协作组与常规组患者血浆LDL-C变化的Meta分析

图5 PNP协作组与常规组患者血浆HDL-C变化的Meta分析

图6 PNP协作组与常规组患者TG变化的Meta分析
3 讨论
国家卫生和计划生育委员会要求:三级甲等医院配备临床药师,并参与多学科联合诊疗,提供用药咨询服务,促进合理用药。临床药师除日常工作外,还要参与医疗团队工作,包括为医护患提供咨询服务、审核处方、患者用药教育、个体化给药监测、开展药学查房、对重点患者实施药学监护和建立药历、参加病例讨论、参加会诊等。虽然国内外已经开展一些关于药师参与医疗团队后的治疗效果研究,但PNP在协作诊疗中各自工作内容不一致,故无参考价值。
本研究结果显示,通过PNP协作组干预后,临床疗效的指标包括血压和胆固醇的控制均优于常规组,且差异有统计学意义。虽然一项RCT[24]显示协作组和常规组比较死亡率和住院率无统计学差异,但仅有1篇,可能存在发表偏倚。总结PNP协作组的工作内容发现,药师干预工作主要包括对患者的教育、对患者的随访工作、用药管理、反馈治疗信息给卫生保健者、评价危险因素和实验室指标、对其他卫生保健者的教育等;医生干预工作主要包括与患者讨论治疗方案、制订用药方案、接受药师建议调整用药方案、患者教育;护士干预工作主要包括基础护理工作和记录患者用药史、测量并记录患者血脂和血压、患者教育、记录患者药品不良反应。
综上所述,通过PNP协作组干预后,患者的主要临床指标均优于常规组。药师在医生-护士团队中发挥了显著的作用。但由于本研究检索策略的局限性,可能检索到PNP协作的文献不足,大多数研究结果均为阳性,不能排除发表偏倚的存在,期待高质量的多中心随机对照试验进行验证。
[1]World Health Organization.The global burden of disease:2004 update[R/OL].2008.http://www.who.int/healthinfo/global_burden_disease/2004_ report_update/en/.
[2]World Health Organization.Noncommunicable diseases prematurely take 16 million lives annually,WHO urges more action[R/OL].2015.http://www.who.int/mediacentre/news/releases/2015/noncommunicable-diseases/en/.
[3]Mathers CD,Loncar D.Projections of global mortality and burden of disease from 2002 to 2030[J].PLoS Med,2006,3(11):e442.
[4]中国普外基础与临床杂志编辑部.多学科协作模式——MDT的探讨[J].中国普外基础与临床杂志,2007,14(3):283.
[5]Peterson ED,Albert NM,Amin A,et al.Implementing critical path ways and a multidisciplinary team approach to cardiovascular disease management[J].The American Journal of Cardiology,2008,102(5A):47-56.
[6]Kaboli PJ,Hoth AB,McClimon BJ,et al.Clinical pharmacists and inpatient medical care:A systematic review[J].Archives of Internal Medicine,2006,166(9):955-964.
[7]Macdonald CJ,Stodel EJ,Chambers LW.An online interprofessional learning resource for physicians,pharmacists,nurse practitioners,and nurses in long-term care:benefits,barriers,and lessons learned[J].Inform Health Soc Care,2008,33(1):21-38.
[8]Salter C,Holland R,Harvey I,et al.“I haven′t even phoned my doctor yet.”The advice giving role of the pharmacist during consultations for medication review with patients aged 80 or more:qualitative discourse analysis[J].British Medical Journal,2007,334(7 603):1 101.
[9]Royal S,Smeaton L,Avery AJ,et al.Interventions in primary care to reduce medication related adverse events and hospital admissions:Systematic review and meta-analysis[J].Quality and Safety in Health Care,2006,15(1):23-31.
[10]Higgins JPT,Green S.Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0[EB/OL].[2011-03-05].The Cochrane Collaboration.http://www.cochrane-handbook.org.
[11]Higgins JPT,Green S.Cochrane Handbook for Systematic Reviews of Interventions Version 5.0.0[EB/OL].[2011-03-05].The Cochrane Collaboration.http://www.cochrane-handbook.org.
[12]Higgins JPT,Thompson SG.Quantifying heterogeneity in a meta-analysis[J].Stat Med,2002,21(11):1 539-1 558.
[13]Villeneuve J,Genest J,Blais L,et al.A cluster randomized controlled Trial to Evaluate an Ambulatory primary care Management program for patients with dyslipidemia:the TEAM study[J].CMAJ,2010,182(5):447-455.
[14]Lee VW,Fan CS,Li AW,et al.Clinical impact of a pharmacist-physician co-managed programme on hyperlipidaemia management in Hong Kong[J].J Clin Pharm Ther,2009,34(4):407-414.
[15]Bogden PE,Koontz LM,Williamson P,et al.The physician and pharmacist team.An effective approach to cholesterol reduction[J].J Gen Intern Med,1997,12(3):158-164.
[16]Rinfret S,Lussier MT,Peirce A,et al.The impact of a multidisciplinary information technology-supported program on blood pressure control in primary care[J].Circ Cardiovasc Qual Outcomes,2009,2(3):170-177.
[17]Carter BL,Ardery G,Dawson JD,et al.Physician and pharmacist collaboration to improve blood pressure control[J].Arch Intern Med,2009,169(21):1 996-2 002.
[18]Santschi V,Rodondi N,Bugnon O,et al.Impact of electronic monitoringof drug adherence on blood pressure control in primary care:a cluster 12-month randomised controlled study[J].Eur J Intern Med,2008,19(6):427-434.
[19]Hunt JS,Siemienczuk J,Pape G,et al.A randomized controlled trial of team-based care:impact of physician-pharmacist collaboration on uncontrolled hypertension[J].J Gen Intern Med,2008,23(12):1 966-1 972.
[20]Carter BL,Bergus GR,Dawson JD,et al.A cluster randomized trial to evaluate physician/pharmacist collaboration to improve blood pressure control[J].J Clin Hypertens(Greenwich),2008,10(4):260-271.
[21]Hennessy S,Leonard CE,Yang W,et al.Effectiveness of a two-part educational intervention to improve hypertension control:a cluster-randomized trial[J].Pharmacotherapy,2006,26(9):1 342-1 347.
[22]de Castro MS,Fuchs FD,Santos MC,et al.Pharmaceutical care program for patients with uncontrolled hypertension.Report of a double-blind clinical trial with ambulatory blood pressure monitoring[J].Am J Hypertens,2006,19(5):528-533.
[23]Borenstein JE,Graber G,Saltiel E,Wallace J,Ryu S,Archi J,et al.Physician-pharmacist comanagement of hypertension:a randomized,comparative trial[J].Pharmacotherapy,2003,23(2):209-216.
[24]Triller DM,Hamilton RA.Effect of pharmaceutical care services on outcomes for home care patients with heart failure[J].Am J Health Syst Pharm,2007,64(21):2 244-2 249.
Efficacy of Collaboration between Physicians-Nurses-Pharmacists for Cardiovascular Disease:A Systematic Review
Su Na,Luo Min,Xu Ting
(Department of Pharmacy,West China Hospital,Sichuan University,Chengdu,Sichuan,China 610041)
Objective To evaluate the effectiveness of collaboration between physicians,nurses and pharmacists for cardiovascular disease.M ethods Randomized Controlled Trails(RCTs)of collaboration between physicians,nurses and pharmacists for cardiovascular disease were retrieved from MEDLINE,EMbase,CENTRAL,CNKI,VIP and WanFang.The retrieved studies were screened according to the inclusion and exclusion criteria,the quality of included studies were evaluated,then performed meta-analyses with The Cochrane Collaboration′s Revman 5.3.0 software.Results 12 RCTs of collaboration between physicians,nurses and pharmacists for cardiovascular disease were included.The results of meta-analyses showed that the change in systolic blood pressure,diastolic blood pressure and total cholesterol was significantly reduced in the collaboration group than in usual care group[RR=-0.41,95%CI(-0.68,-0.14),P=0.003], [RR=-0.10,95%CI(-0.14,-0.06),P<0.000 01],[RR=-0.44,95%CI(-0.72,-0.16),P=0.002].There was no statistically significant difference in the death rate and hospitalization rate between the collaboration group and usual care group.Conclusion Collaboration between physicians,nurses and pharmacists is effective for cardiovascular disease.But its long-term efficacy still needs to be confirmed by performing more high quality,large sample RCTs with long term follow-up.
physicians;nurses;pharmacists;collaboration;systematic review
R952
A
1006-4931(2015)19-0051-05
2015-05-13)
β四川省软科学研究计划项目,项目编号:2014ZR0088。
