Improvement in acupoint selection for acupuncture of nerves surrounding the injury site: electro-acupuncture with Governor vessel with local meridian acupoints
2015-01-18GuanhengHeJingwenRuanYuanshanZengXinZhouYingDingGuanghuiZhou
Guan-heng He, Jing-wen Ruan,, Yuan-shan Zeng, Xin Zhou, Ying Ding, Guang-hui Zhou
1 Department of Acupuncture, the First Affliated Hospital, Sun Yat-sen University, Guangzhou, Guangdong Province, China
2 Division of Neuroscience, Department of Histology and Embryology, Zhongshan School of Medicine, Sun Yat-sen University, Guangzhou, Guangdong Province, China
3 Rehabilitation Department, People’s Hospital of Dongguan Shilong, Southern Medical University, Dongguan, Guangdong Province, China
Improvement in acupoint selection for acupuncture of nerves surrounding the injury site: electro-acupuncture with Governor vessel with local meridian acupoints
Guan-heng He1, Jing-wen Ruan1,*, Yuan-shan Zeng2, Xin Zhou1, Ying Ding2, Guang-hui Zhou3,*
1 Department of Acupuncture, the First Affliated Hospital, Sun Yat-sen University, Guangzhou, Guangdong Province, China
2 Division of Neuroscience, Department of Histology and Embryology, Zhongshan School of Medicine, Sun Yat-sen University, Guangzhou, Guangdong Province, China
3 Rehabilitation Department, People’s Hospital of Dongguan Shilong, Southern Medical University, Dongguan, Guangdong Province, China
Peripheral nerve injury not only affects the site of the injury, but can also induce neuronal apoptosis at the spinal cord. However, many acupuncture clinicians still focus only on the injury site, selecting acupoints entirely along the injured nerve trunk and neglecting other regions; this may delay onset of treatment effcacy and rehabilitation. Therefore, in the present study, we compared the clinical effcacy of acupuncture at Governor vessel and local meridian acupoints combined (GV/LM group) with acupuncture at local meridian acupoints alone (LM group) in the treatment of patients with peripheral nerve injury. In the GV/LM group (n = 15), in addition to meridian acupoints at the injury site, the following acupoints on the Governor vessel were stimulated: Baihui (GV20), Fengfu (GV16), Dazhui (GV14), and Shenzhu (GV12), selected to treat nerve injury of the upper limb, and Jizhong (GV6), Mingmen (GV4), Yaoyangguan (GV3), and Yaoshu (GV2) to treat nerve injury of the lower limb. In the LM group (n = 15), only meridian acupoints along the injured nerve were selected. Both groups had electroacupuncture treatment for 30 minutes, once a day, 5 times per week, for 6 weeks. Two cases dropped out of the LM group. A good or excellent clinical response was obtained in 80% of the patients in the GV/ LM group and 38.5% of the LM group. In a second study, an additional 20 patients underwent acupuncture with the same prescription as the GV/LM group. Electomyographic nerve conduction tests were performed before and after acupuncture to explore the mechanism of action of the treatment. An effective response was observed in 80.0% of the patients, with greater motor nerve conduction velocity and amplitude after treatment, indicating that electroacupuncture on specifc Governor vessel acupoints promotes functional motor nerve repair after peripheral nerve injury. In addition, electromyography was performed before, during and after electroacupuncture in one patient with radial nerve injury. After a single session, the patient’s motor nerve conduction velocity increased by 23.2%, indicating that electroacupuncture at Governor vessel acupoints has an immediate therapeutic effect on peripheral nerve injury. Our results indicate that Governor vessel and local meridian acupoints used simultaneously promote functional repair after peripheral nerve injury. The mechanism of action may arise from an improvement of the local microenvironment in injured nervous tissue, as well as immediate effects of Governor vessel and local meridian acupoint stimulation to ensure the continuity between the peripheral and central nervous systems.
nerve regeneration; peripheral nerve injury; acupuncture; electroacupuncture; Governor vessel acupoints; local acupoints; electrophysiology; spinal cord; motor nerve conduction; functional repair; neural regeneration
Funding:This study was supported by the Guangdong Province Science and Technology Plan, No. 2010B030700008; the Guangzhou Science and Technology Plan Application Foundation, No. 2012J4300062; the Major Project of Science and Technology Plan of Dongguan City in 2012, No. 2012105102022.
He GH, Ruan JW, Zeng YS, Zhou X, Ding Y, Zhou GH (2015) Improvement in acupoint selection for acupuncture of nerves surrounding the injury site: electro-acupuncture with Governor vessel with local meridian acupoints. Neural Regen Res 10(1):128-135.
Introduction
Functional recovery of peripheral nerve injury is a slow process. This may be because of the length of time needed for neural regeneration and functional reconstruction, but treatment methods may also contribute to the delay in recovery (Jin et al., 2013; Ma et al., 2013). Clinicians often consider peripheral nerve injury as isolated local damage, and focus on treating the problem only at the site of the injury, especially when using non-drug therapies. In acupuncture, the acupoints selected are almost entirely along the injured nerve trunk (Chan et al., 1999; Dong et al., 2008; Sheng et al., 2008). However, peripheral nerve injury does not simply cause local damage (Gu et al., 2004), but can also induce apoptosis of individual spinal cord neurons in corresponding segments of the spinal cord (Gong, 2002; Lv et al., 2005; Wu et al., 2006; Lu et al., 2007). Neuronal apoptosis has little impact on the surrounding tissue structure, and the morphology and function of adjacent neurons or parts of glial cells remain normal. However, ignoring the treatment of spinal cord segment lesions may hinder a patient’s rehabilitation. Based on the above understanding, clinicians should not only focus on local injury, but should also pay attention to the treatment of secondary apoptosis of spinal cord neurons. Therefore, the traditional prescription for clinical acupuncture, which only selects the acupoints around the local injury (Li et al., 2013; Xia et al., 2013), must be adjusted accordingly. Few studies have addressed this to date. Therefore, in the present study, we determined the effcacy of a novel acupoint principle compared with the traditional method, and discussed its possible mechanism.
According to the meridian theory, the Governor vessel extends along the center of the spine, overlapping the spinal cord. Spinal cord injury is therefore often thought to be associated with Governor vessel injury, and Governor vessel acupoints are usually selected to treat spinal cord injuries or diseases. The vessel can also stimulate local segments of spinal cord tissues, causing the secretion of large amounts of neurotrophin-3 (Zhang et al., 2012), which can provide a suitable microenvironment for spinal cord injury repair. Here, we selected Governor vessel acupoints to treat spinal cord lesions arising from peripheral nerve injury.
The purpose of the present study is to improve the clinical effcacy of acupuncture by enhancing our understanding of acupoint selection. Using an approach that diverges from the traditional acupoints principle, we selected Governor vessel acupoints located on the segment of apoptotic spinal cord neurons that corresponded to the injury site, in combination with the local acupoints around the injured nerve. We used electrophysiological tests to determine the repair status of the injured peripheral nerve and to investigate the electrophysiological mechanism underlying acupuncture therapy of peripheral nerve injury.
Subjects and Methods
Subjects
This study was approved by the Ethics Committee of the First Affliated Hospital, Sun Yat-sen University, China. The study was divided into two stages: in the frst stage, we compared the clinical effcacy of electroacupuncture at local meridian acupoints alone with acupuncture at Governor vessel and local meridian acupoints combined; in the second stage, we investigated electromyographic responses to the combined method. A total of 50 patients with peripheral nerve injury were enrolled from the Acupuncture Department of the First Affliated Hospital of Sun Yat-Sen University, China in accordance with the diagnostic and inclusion criteria listed below. Thirty patients were recruited for the frst stage and divided randomly (using a random number table) and equally into two experimental groups: local meridian acupoints alone (LM) and Governor vessel with local meridian acupoints (GV/LM) (Table 1).
For the second stage, an additional 20 patients were recruited. The demographic data for these 20 patients is shown inTable 2.
Diagnostic criteria
With reference to Surgery (Wu et al., 2006): (1) patient has sensory nerve, motor nerve and autonomic nerve damage; (2) tendon refex is reduced or absent; (3) electrophysiological test indicates single or multiple peripheral nerve damage, including axonal changes and demyelination.
Inclusion criteria
(1) Patient has a diagnosis of peripheral nerve injury; (2) is aged 18-75 years; (3) has electrophysiologically-confirmed peripheral nerve damage such as demyelination; (4) is willing to join this randomized controlled study and (5) has signed the informed consent form.
Exclusion criteria
Patients with mental disorders, liver or kidney dysfunction, circulatory system diseases, or transmissible infections were excluded.
Acupoint prescription
LM group
The following acupoints were selected at the injury site: radial nerve: Jianyu (LI15), Binao (LI14), Quchi (LI11), Hegu (LI4), and Yangxi (LI5); ulnar nerve: Qingling (HT2), Xiaohai (SI8), Zhizheng (SI7), Wangu (SI4), and Houxi (SI3); median nerve: Quze (PC3), Daling (PC7), Neiguan (PC6), and Laogong (PC8); peroneal nerve: Yanglingquan (GB34), Guangming (GB37), Juegu (GB39), and Qiuxu (GB40); tibial nerve: Yinlingquan (SP9), Sanyinjiao (SP6), Diji (SP8), and Lougu (SP7); sciatic nerve: Huantiao (GB30), Ciliao (BL32), Zhibian (BL54), Yanglingquan (GB34), Weizhong (BL40), and Juegu (GB39); brachial plexus: Jianyu (LI15), Binao (LI14), Quchi (LI11), Waiguan (SJ5), and Baxie (EX-UE8).
GV/LM group
The following acupoints were selected: (1) Acupoints on the Governor vessel: nerve injury in the arm: Baihui (GV20), Fengfu (GV16), Dazhui (GV14), and Shenzhu (GV12); nerve injury in the leg: Jizhong (GV6), Mingmen (GV4), Yaoyang-guan (GV3), and Yaoshu (GV2). (2) Local acupoints at the injury site were as described in the previous group.
Acupuncture procedure
After routine disinfection of the acupuncture sites with 75% alcohol, we used stainless steel disposable acupuncture needles (0.35 mm diameter, 25 mm length; Suixin brand, Suzhou Hualun Medical Appliance Corporation, Suzhou, Jiangsu Province, China) for the treatment. The needles were placed approximately 1 cun deep into the selected acupoints. After manipulation by hand to achieve the desired sensation, the needles were connected to the electroacupuncture apparatus (Ying Di KWD-808-I Multi-Purpose Health Device; Changzhou Yindi Electronic Medical Device Corporation, Changzhou, Jiangsu Province, China). A sparse-dense wave with a frequency of approximately 2/100 Hz was selected and the magnitude of the stimulation was as great as each patient could tolerate. The needles were withdrawn after 30 minutes of treatment. The procedure was conducted for 6 weeks, once a day, fve times per week (30 sessions in total).Clinical testing
Stage 1: clinical response
The therapeutic efficacy of the two acupuncture methods was examined by evaluating the motor and sensory functions of the patients’ affected limb before and after the course of treatment, using the method recommended by the British Medical Research Council (Zhu et al., 2007). Treatment response was ranked as follows: excellent (sensory and motor function recovered to ≥ S3+and ≥ M4, respectively); good (composite function recovered to S3 or M3, or pure sensory or motor function recovered to ≥ S3+or ≥ M4); average (composite function recovered to S2 or M2, or pure sensory or motor function recovered to ≥ S3 or ≥ M3); poor (function ≤ S1 and/or ≤ M1).
Stage 2: electromyography
Acupuncture was performed in 20 additional patients using the GV/LM method. Electromyography was carried out before and after the treatment to detect the motor and sensory nerve conduction velocity as well as the latency and amplitude of different nerve injuries in order to determine the nerve repair status. Keypoint 4-channel electromyography (Dantec, Alpine Biomed ApS, Skovlunde, Denmark) was used to measure motor and sensory nerve conduction velocity, latency, and amplitude in different nerve injuries. For motor nerve conduction, we used disposable skin electrodes and placed the cathode of the electrode over the distal nerve. The anode was placed over the proximal nerve. The recording electrodes were over the muscle belly, and the reference electrode was placed over the tendon. The ring electrode was placed between the stimulation and recording electrodes. We recorded the peak-to-peak amplitude and latency of compound muscle action potentials on the muscle controlled by the injured nerve. The nerve conduction velocity was calculated as the distance between the distal and proximal ends of the nerve divided by the difference between the distal and proximal latencies. Sensory conduction was measured orthodromically by the ring electrode. The stimulating electrode was placed at the tip of a fnger or toe. The cathode was at the proximal end of the nerve to the anode. Recording electrodes were placed over the nerve trunk, close to the stimulation site. Reference electrodes were placed at the opposite end of the nerve trunk to the stimulation site. A ground wire was fxed between the stimulating and recording electrodes. The latency period was measured, and sensory conduction velocity was calculated as the distance between the stimulating and recording electrodes divided by the latency.
Electromyographic responses to treatment were ranked as follows: Complete (motor and sensory functions returned to normal; electrophysiology returned to normal); excellent (motor and sensory disorders notably improved; electrophysiology not returned to normal but motor and sensory conduction velocities increased by ≥ 5 m/s); moderate (motor and sensory function slightly improved; motor and/or sensory conduction velocity increased, but by < 5 m/s); ineffective (no improvement, or worsening, of motor or sensory function; no increase, or possible decrease, in motor and sensory conduction velocities relative to baseline).
Statistical analysis
All data were analyzed using SPSS 17.0 software (SPSS, Chicago, IL, USA) and conformed to a normal distribution. Counts were expressed as percentages and analyzed using the chi-square test; measurements were expressed as the mean ± SD. Independent sample t-tests were used to compare two groups, while a paired t-test was used for comparing data obtained before and after treatment. P < 0.05 was considered statistically signifcant.
Results
Quantitative analysis of participants
In the frst stage, a total of 30 patients were enrolled and assigned equally and at random to the LM and GV/LM groups. Two patients dropped out from the LM group. There were marginally more male patients than female patients in both groups. The patients were aged 18-40 years and the duration of their illness was < 2.5 years. Before treatment, there were no statistically signifcant differences between the groups in terms of gender, age, or duration of illness (P > 0.05;Table 1). In the second stage, 20 patients were enrolled, with no drop-outs.
Comparison of good or excellent response rates between the GV/LM and LM groups
In the GV/LM group (n = 15), functional response was ranked excellent in four patients and good in eight patients, with a combined good and excellent rate of 80%. In the LM group (n = 13), treatment response was ranked excellent in three cases and good in two cases. The good or excellent response rate was 38.5%, significantly lower than that in the GV/LM group (P < 0.05;Table 3), indicating that the therapeutic effect of electroacupuncture at Governor vessel acupoints combined with local meridian acupoints is more clinically effective in the treatment of peripheral nerve injury than the use of local meridian acupoints alone.
Electromyographical comparison of sensory conduction between before and after electroacupuncture along the Governor vessel and local meridian
The sensory conduction velocities of the radial and ulnar nerves were signifcantly greater after treatment than before treatment (P < 0.05,Table 4). The latencies for these nerves were also improved after treatment (P < 0.05).
However, no signifcant differences were found in the latency, potential amplitude, or sensory conduction velocity of the median, tibial or peroneal nerves (P > 0.05).
Electromyographical comparison of motor conduction between before and after electroacupuncture along the Governor vessel and local meridian
The motor conduction velocities of the radial and tibial nerves were signifcantly increased after treatment (P < 0.05,Table 5). Treatment also improved the potential amplitude for these nerves (P < 0.05). However, the difference in latency was not statistically signifcant before and after treatment (P > 0.05).
In the median nerve, treatment improved the latency, potential amplitude, and sensory conduction velocity (P < 0.05,Table 5). The latency and potential amplitude of the ulnar and peroneal nerves were also significantly improved after treatment (P < 0.05,Table 5), but motor conduction velocity was not signifcantly different (P > 0.05).
Clinical effcacy
The total effective therapeutic rate was 80.0% in the 20 patients (Table 6). Six patients had not received any prior treatment before entering the study, and in fve of those (83.3%) the treatment was effective. There were 14 patients who had received other therapies before entering the study, and their effcacy rate was 78.6%. The difference between these effcacy rates was not signifcant (P > 0.05). Although this study had a relatively small sample size, these results suggest that electroacupuncture is clinically effective in peripheral nerve injury whether or not the patient underwent previous treatment attempts.
Typical case
Figure 1shows radial nerve motor conduction electromyography before, during and after electroacupuncture in an 18-year-old female patient in the GV/LM group who suffered from radial nerve injury for 2 months.Figure 2shows electromyography traces of motor and sensory conduction in the radial nerve before and after treatment in the same patient.
Discussion
The peripheral nerve and the cell bodies of its corresponding spinal cord segments are physiologically and pathologically interdependent
A neuron consists of a cell body and cytoplasmic processes. The cell bodies are located in the brain or spinal cord, and the processes, which constitute the peripheral nerve, innervate the target tissue, which can be a long distance from the cell body. As two parts of the same neuron, the cell body and cytoplasmic processes are interdependent under physiological and pathological conditions. The peripheral nerve is mainly composed of long nerve fibers or axons and has no capacity to synthesize the proteins and lipids necessary for injury repair, but rather depends on the neuronal cell body. However, the survival of the cell body also relies on the functional integrity of the axon (Roy et al., 1999). To survive and maintain physiological function, the neuronal cell body communicates through its axon with peripheral target tissues and Schwann cells, which release neurotrophic factors. Thus, the cell body of a neuron and its axon are physiologically interdependent, which in turn determines their relationship with each other under pathological conditions. Peripheral nerve injury causes apoptosis of corresponding neuronal cell bodies (Wu et al., 2006). After peripheral nerve injury, nutrient transport is interrupted or obstructed, causing the cell bodies to lose target-derived neurotrophic factors, resulting in apoptosis (Himes et al., 1989). Because adult neurons cannot divide or proliferate, the decline in neuronal number will lead to a decreased number of peripheral nerve fbers. This pathophysiological relationship will affect the time and extent of functional recovery after peripheral nerve injury. Therefore, to ensure the injured peripheral nerve has renewable materials available, preventing neuronal apoptosis is an important strategy to improve the structural and functional recovery of peripheral nerves after injury. This is why we aim to improve acupuncture therapy in this feld.
The apoptosis of spinal motor neurons and spinal ganglion sensory neurons induced by peripheral nerve injury is not widespread and does not involve the whole spinal cord, but is associated with neurons that are related to the damaged peripheral nerves. For example, after cutting the rat sciatic nerve on one side, the ipsilateral L4-6anterior horn motor neurons, sensory neurons and sciatic nerve all express p75, a low affinity nerve growth factor receptor, which induces neuronal apoptosis; however, no expression is found at the injury site (Yun et al., 2001). This suggests that selecting acupoints along the injured peripheral nerve in combination with those along the Governor vessel in the corresponding spinal segments will improve therapeutic outcome.
Electroacupuncture on specifc Governor vessel acupoints promotes functional repair after peripheral nerve injuryIn the frst stage of this study, a higher rate of good and excellent clinical responses was observed in the GV/LM group than in the LM group, indicating that the therapeutic effect of electroacupuncture on Governor vessel and local acupoints combined was better for the successful treatment of peripheral nerve injury than restricting treatment to local meridian acupoints. In the second stage, the total effective rate was 80.0%, with the greatest effect on motor nerve conduction. Electroacupuncture on specific Governor vessel acupoints appears to promote functional repair after peripheral nerve injury, particularly in terms of motor conduction. We also calculated the total effective rate after 30 days of acupuncture in 14 patients who had received other treatments before entering this study. Acupuncture effcacy wasnot signifcantly different between patients with or without previous treatment attempts, indicating that acupuncture at both sites is effective regardless of treatment history. The sample size was small, so a larger sample size should be used in future studies.

Table 1 Baseline data of the 30 patients in stage 1

Table 3 Clinical effcacy of electroacupuncture in the Governor vessel with local meridian acupoints (GV/LM) group and the local meridian acupoints (LM) group
Possible mechanisms of electroacupuncture on specifc Governor vessel acupoints for peripheral nerve injury
(1) Electroacupuncture on the Governor vessel improves the microenvironment of the nervous tissue and stimulates neurotrophic factor release
After sciatic nerve injury, the metabolic microenvironment of the lumbar spinal cord shows reduced acetylcholinesterase activity and increased acid phosphatase activity, the main causes of apoptosis in the affected neurons (Zhang et al., 2002; Yan et al., 2013; Chen et al., 2014). Therefore, reducing the toxicity of the microenvironment is one of the important ways to prevent neuronal apoptosis. Furthermore, electroacupuncture stimulation increase acetylcholinesterase expression in spinal cord tissue after peripheral nerve injury (Wang et al., 2009). It can be presumed that electroacupuncture on Governor vessel acupoints combined with local acupoints can also increases acetylcholinesterase expression in spinal cord tissue, which helps to adjust the toxic environment and prevent secondary impairment of neurons. This may be the primary mechanism for peripheral nerve injury treatment. In addition, electroacupuncture on theGovernor vessel can also stimulate local spinal cord tissue to secrete large amounts of neurotrophic factor 3 (Li et al., 2012; Zhang et al., 2012), effectively preventing or delaying neuronal apoptosis. Therefore, an important mechanism underlying the treatment of peripheral nerve injury by electroacupuncture on the Governor vessel is a reduction in tissue toxicity and stimulation of neurotrophin release, which provides a microenvironment conducive to nerve repair.
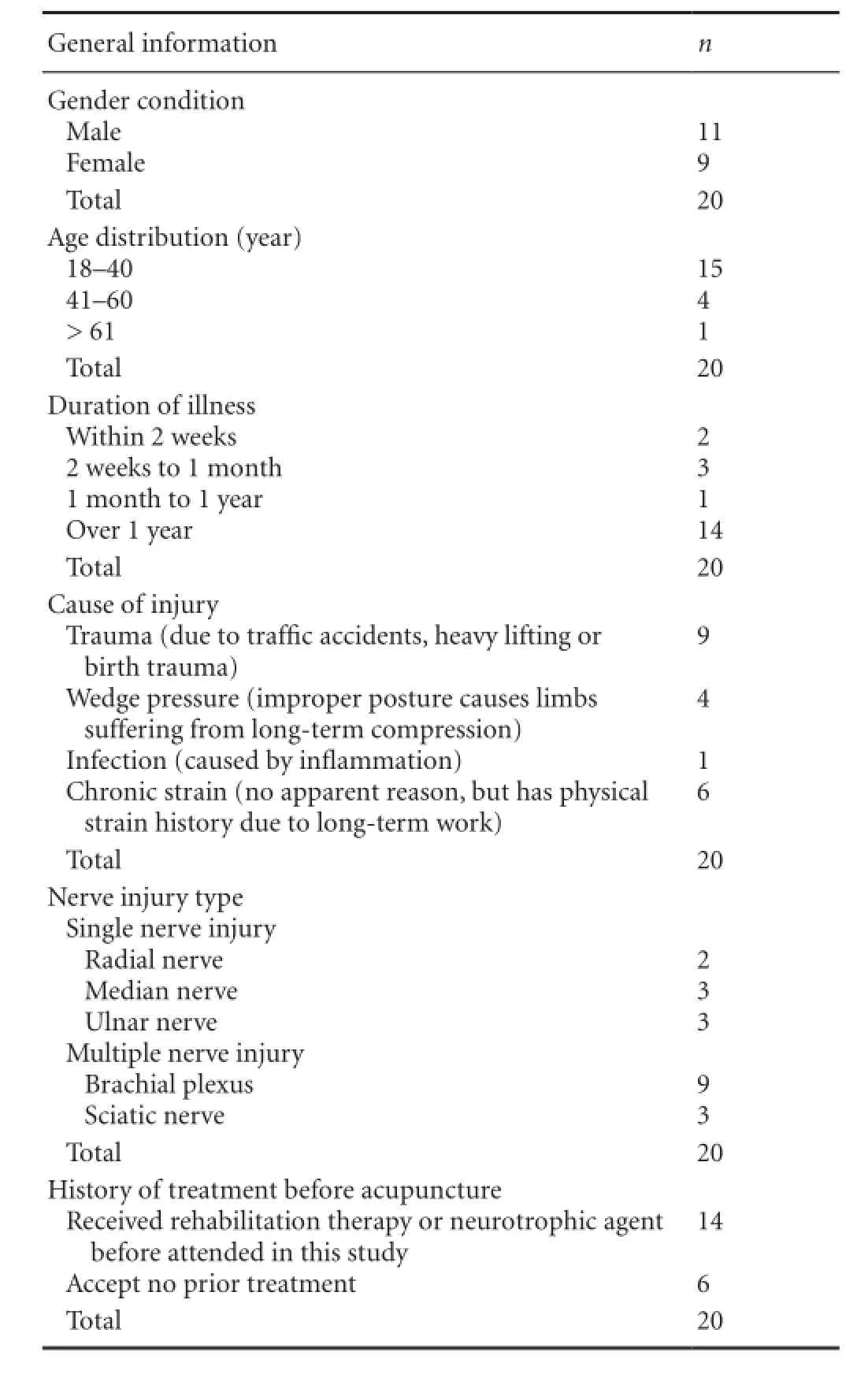
Table 2 Demographic data for the 20 patients in stage 2
(2) Immediate effect of electroacupuncture on Governor vessel acupoints ensures continuity between the peripheral and central nerve
FromFigure 1, electromyography revealed considerable changes in radial nerve motor conduction before, during and after electroacupuncture. The immediate therapeutic effects of electroacupuncture on the Governor vessel are evident. Electroacupuncture on both the Governor vessel and local acupoints can provide temporary continuity between the damaged peripheral nerve and the central nerve, thereby ensuring the supply of nutrients between neuronal cell bodies and maintaining neurotrophic factors, a lack of whichwould cause neuronal apoptosis. Providing this assistance may shorten the repair process for damaged nerves, and can also provide a basis for nerve regeneration.
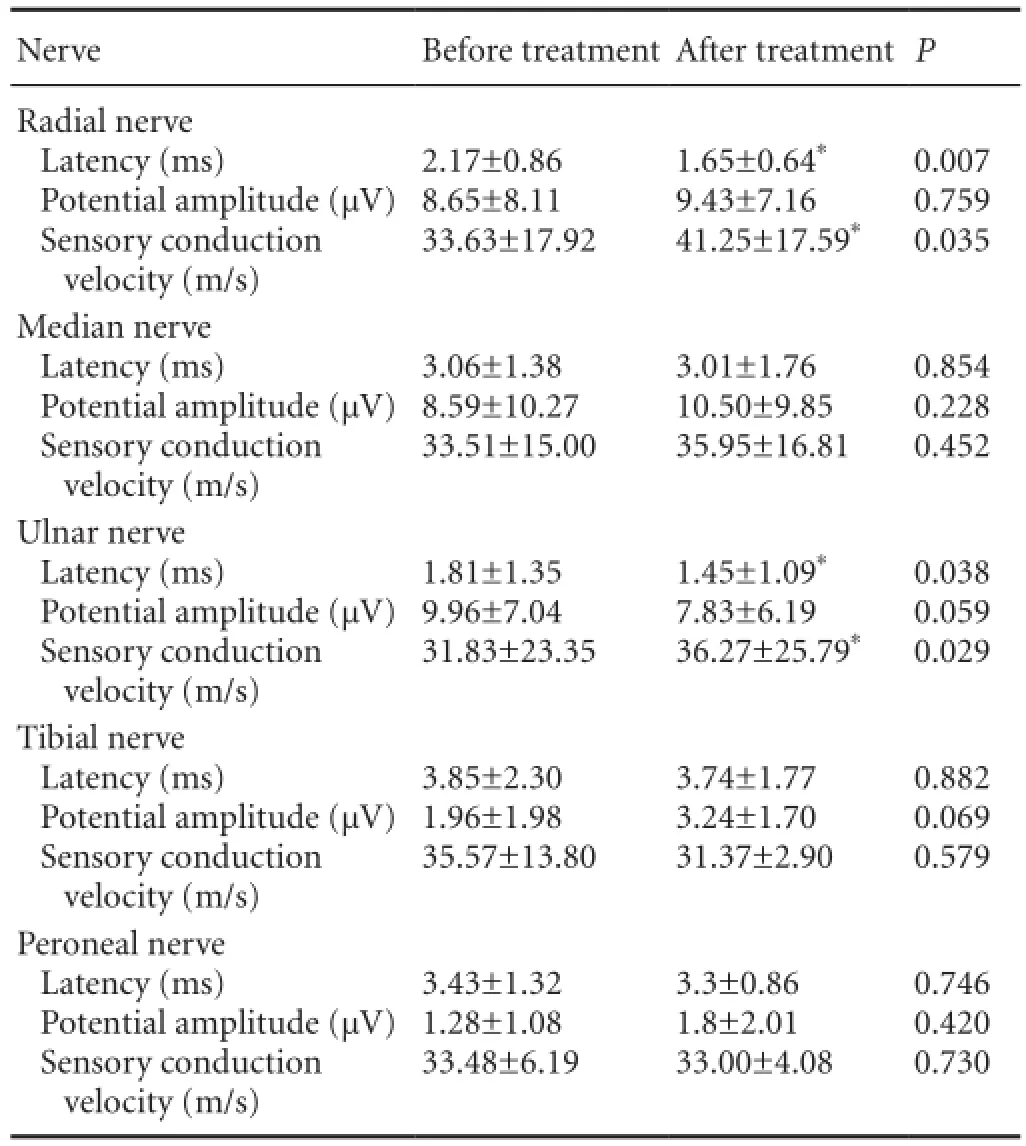
Table 4 Sensory nerve conduction before and after 30 sessions of electroacupuncture on Governor vessel and local meridian acupoints

Table 6 Therapeutic efficacy of electroacupuncture on Governor vessel and local meridian acupoints in 20 patients in stage 2
Interestingly, electroacupuncture had little effect on sensory nerve conduction (Figure 2), consistent with our fndings that after 30 days of treatment, motor nerve conduction recovered well, whereas sensory nerve conduction recovery was poor.
Together, our results indicate that the current treatment options have little effect on sensory nerve recovery over a 30 day observation period. Sensory nerves may require a longer treatment time to achieve the desired effect, or perhaps a larger sample size would have revealed an effect on sensorynerve conduction. This delayed recovery of sensory function compared to motor function is related to the regeneration of motor neuron axons after peripheral nerve injury, which dominates muscular branches, known as prioritization of muscle branch reinnervation (Richard et al., 2005; Zheng et al., 2010; Maeda et al., 2013). Moreover, it is also associated with axons retreating to the cell body after peripheral nerve injury (Witzel et al., 2005). Synapses around neuronal axons also withdraw from the surface and, after nerve regeneration, barriers to axonal morphology restoration remain, which is also one of the important reasons why recovering sensory function is diffcult (Watson et al., 1974). Therefore, in reconstructive surgery on denervated tissue, neuron dendrite growth must be guided towards its original target tissue; this will be our key scientifc research question in the future.

Table 5 Comparison of motor nerve conduction between before and after 30 sessions of electroacupuncture on Governor vessel and local meridian acupoints
In conclusion, electroacupuncture on specific Governor vessel acupoints appears to effectively promote functional repair after peripheral nerve injury. The mechanism may relate to the Governor vessel improving the local microenvironment and ensuring continuity between the peripheral and central nerve. Therefore, the preferred acupoint prescription for peripheral nerve injury should focus on two sites, the injury site and the spinal cord, i.e. simultaneous electroacupuncture on the Governor vessel and local meridian acupoints. A limitation of the present study is the small number of subjects; however, a trend is evident and more indepth studies with larger sample sizes should be performed to confrm our results.

Figure 1 Electromyograms of radial nerve motor conduction before, during and after electroacupuncture in an 18-year-old female patient with radial nerve injury for 2 months.

Figure 2 Electromyography of radial nerve motor and sensory conduction before and after electroacupuncture.
Acknowledgments:We are very grateful to Yin-xing Liang from Department of Electrophysiology, the First Affiliated Hospital, Sun Yat-sen University, China, who contributes to the operation of electromyography.
Author contributions:JWR designed the research. GHH and XZ performed the research and collected the data. GHH and JWR analyzed the data and wrote the paper. JWR, YSZ, YD and GHZ took charge of technical or material supports. All authors approved the final version of the paper.
Conficts of interest:None declared.
Chan BZ, Shao JS (1999) The clinical observation of the curative treatment of peripheral nerve injury. Shanghai Zhen Jiu Zazhi 18:16-17.
Chen XH, Li RY, Zhang GD, Lin HB, Wu XW, Lin YJ, Zheng F (2014) Possible mechanisms of cholecystokinin promoting sciatic nerve regeneration. Zhongguo Zuzhi Gongcheng Yanjiu 18:1700-1705.
Ding Y, Yan Q, Ruan JW (2010) Electro-acupuncture promotes survival, differentiation of the bone marrow mesenchymal stem cells as well as functional recovery in the spinal cord-transected rats. BMC Neurosci 10:35.
Dong ZG, Pan YH, Liu YY (2008) Electric acupuncture plus point injection in the treatment of ulnar nerve injury of 31 cases of clinical observation. Heilongjiang Yi Yao Ke Xue Zazhi 31:102.
Gong FL (2002) Medical immunology. Beijing: Science and Technology Publishing House 258-261.
Gu YD (2004) Several basic problems of diagnosis and treatment of peripheral nerve injury. Yixue Linchuang Yanjiu 21:449-450.
Himes BT, Tessler A (1989) Death of some dorsal root ganglion neurons and plasticity of others Following sciatic nerve section in adult and neonatal rats. J Comp Neurol 284:215-230.
Jin WH, Wei ZR, Sun GF, Tang XJ, Wang DL (2013) Autologous peripheral blood stem cell transplantation for treatment of peripheral nerve injury. Zhongguo Zuzhi Gongcheng Yanjiu 17:181-185.
Li SC, Lu PS, Lao JX, Deng C, Gu TT (2013) Effcacy observation on traumatic nerve injury treated with different acupuncture therapies. Zhongguo Zhen Jiu 33:993-995.
Li WJ, Pan SQ, Zeng YS (2010) Identifcation of acupuncture-specifc proteins in the process of electro-acupuncture after spinal cord injury. Neurosci Res 67:307-316.
Li WJ, Pan SQ, Zeng YS (2012) Electro-acupuncture upregulates CGRP expression after rat spinal cord transaction. Neurochem Int 61:1397-1403.
Lu XM, Wang YT,Y u Y (2007) Research of apoptosis and mechanism of dynamoneure following sciatic nerves in rats. Zhongguo Xiandai Yixue Zazhi 17:1169-1172.
Lv Y, Liu SH, Ge XM (2005) Effect of sciatic nerve injury due to different causes on gene expression in corresponding segment of spinal cord. Ganran Yanzheng Xiufu 6:78-71.
Ma HB, Zhang RM (2013) Chemically extracted acellular allogenic nerve and accompanying peripheral vein for repair of facial nerve defects. Zhongguo Zuzhi Gongcheng Yanjiu 17:3325-3332.
Maeda Y, Kettner N, Lee J (2013) Acupuncture evoked response in contralateral somatosensory cortex refects peripheral nerve pathology of carpal tunnel syndrome. Med Acupunct 25:275-284.
Richard R, Rajesh J, Thomas C (2005) Peripheral pathways regulate motoneuron collateral dynamics. Neuroscience 25:9406-9412.
Roy M, Sapolsky R (1999) Neuronal apoptosis in acute necrotic insults: why is this subject such a mess. Trends Neurosci 22:419-422.
Sheng YX, Wang GX, Yang WZ (2008) Curative effect observation of electroacupuncture treatment for radial nerve injury. Shanxi Zhongyi 29:885-887.
Wang DY (1997) Acupuncture treatment of 30 cases of peripheral nerve injury. Zhongguo Zhen Jiu 17:726.
Wang RH, Liu HY (2009) effect of electroacupuncture on acetylcholinesterase in spinal cord tissue after sciatic nerve injury in rabbits. Shanxi Zhongyi 30:232-233.
Watson WE (1974) Cellular response to axotomy and to related procedures. Br Med Bul 30:112.
Witzel C, Rohde C, Brushart TM (2005) Pathway sampling by regenerating peripheral axons. Comp Neurol 485:183-190.
Wu D, Liu Q, Chen JC (2006) Peripheral nerve injury in rats of spinal motor neurons morphology observation. Shandong Yiyao 46:23-24.
Wu ZD,Wu ZH (2006) Surgery. 6thed. Beijing: People’s Medical Publishing House.
Xia Q, Liu XW, Wang XL, Tao Y (2013) Effcacy observation of carpal tunnel syndrome treated with electroacupuncture. Zhongguo Zhen Jiu 33:700-702.
Xiao GR, Hao H, Zhao QL (2007) Observation on therapeutic effect of electro-acupuncture combined with functional training for treatment of peripheral nerve incomplete injury of the upper limbs. Zhongguo Zhen Jiu 27:329-332.
Yan LP, Liu YG, Wu XT, Li SD, Ma C (2013) Effect of electroacupuncture intervention on N-methyl-D-aspartic acid receptor expression in spinal cord in rats with chronic constrictive injury of the sciatic nerve. Zhen Ci Yan Jiu 38:380-385.
Yun FM, Qin JQ, Jiang LX (2001) The expression of p75 following peripheral nerve injury in rat. Zhongguo Linchuang Jiepou Zazhi 1:71-72.
Zhang F, Hong GX, Wang FB (2002) Protective effect of basic fbroblast growth factor on motor neurous in anterior horn of spinal cord after sciatic nerve injury. Zhong Guo Zu Zhi Hua Xue Yu Xi Bao Hua Xue Zazhi 11:59-62.
Zhang K, Zeng YS, Qin LN (2012) Effects of governor vessel electro-acupuncture on expression of neurotrophin-3 in rat spinal cord injured early. Jiepouxue Yanjiu 34:411-414.
Zheng LL, Xiao B (2010) Survival and of motoneurons after brachiai lnjury. Zhongguo Kangfu Lilun yu Shijian 16:1031-1033.
Zhu JK, Luo YX, Chen TY (2007) Modern peripheral nerve surgery. Shanghai: Shanghai Scientifc and Technical Publishing House.
Copyedited by Slone-Murphy J, de Souza M, Wang J, Qiu Y, Li CH, Song LP, Zhao M
*Correspondence to: Jing-wen Ruan, ruanjw@163.com. Guang-hui Zhou, zhouguanghui2072@163.com.
10.4103/1673-5374.150720
http://www.nrronline.org/
Accepted: 2014-08-29
杂志排行
中国神经再生研究(英文版)的其它文章
- Neural Regeneration Research (NRR) Instructions for Authors (2015)
- Hypersensitivity of vascular alpha-adrenoceptor responsiveness: a possible inducer of pain in neuropathic states
- Neural regeneration after peripheral nerve injury repair is a system remodelling process of interaction between nerves and terminal effector
- Acute carbon monoxide poisoning and delayed neurological sequelae: a potential neuroprotection bundle therapy
- Prediabetes and type 2 diabetes implication in central proliferation and neurogenesis
- Clinical strategies to enhance nerve regeneration